What is Cystinuria and Who Gets It?
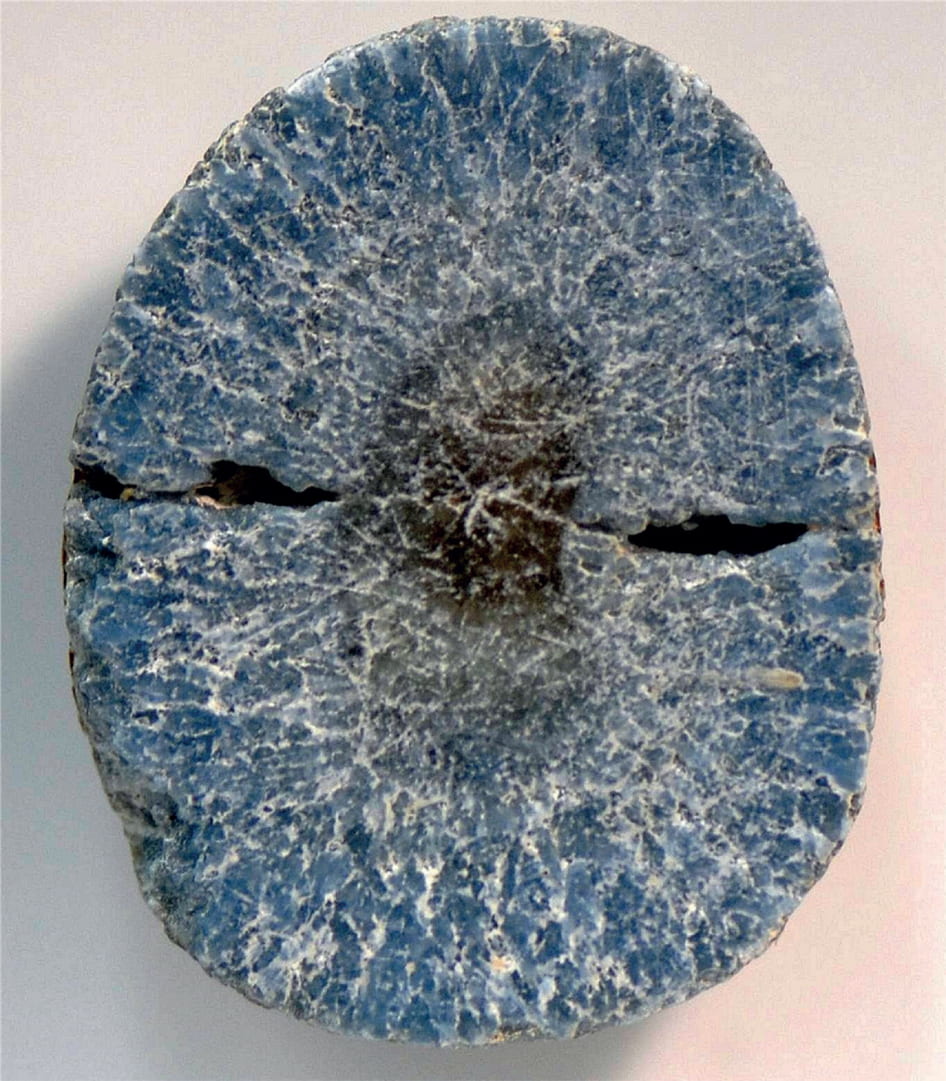
 Cystinuria is a rare genetic disorder that results in abnormally high level of cystine in the urine. High levels of cystine in the urine predispose to kidney stone formation, so patients are diagnosed when they present with kidney stones. The featured image shows the first such stone.
Cystinuria is a rare genetic disorder that results in abnormally high level of cystine in the urine. High levels of cystine in the urine predispose to kidney stone formation, so patients are diagnosed when they present with kidney stones. The featured image shows the first such stone.
Much of what is known about human genetic disorders is summarized in a remarkable resource which some of you might want to consult. Here are some salient facts about the disease. Cystinuria occurs in 1 in 7,000 people worldwide. As the disorder is genetic, there is variability in its occurrence based on who your ancestors were. For example, it occurs in 1 in 100,000 people in Sweden, but is far more common in Israeli patients of African origin: 1 in 2,500. In the United States, the incidence is about 1 in 15,000 individuals. While clearly rare, it is responsible for 2-3% of all kidney stones, and is even more common in kids (about 5%) as stones are generally less common in the young. Because of the genetics of cystinuria, it is not uncommon to have siblings afflicted with the disorder, particularly in larger families. It is important to note that cystinuria is a different disorder from cystinosis, which I will not discuss further here.
What is Cystine Anyway?
Cystine is a non-essential amino acid, meaning that our bodies are able to make it from other proteins (and that we don’t need to obtain it from the diet). Cystine is formed from two molecules of cysteine, another amino acid, that are connected via a disulfide bond.
Cystine is found in multiple tissues, including tendons, skin and hair. For example, whether you have straight or curly hair is determined by the number of cystine disulfide bonds that you have. Hair products that make your hair curly promote formation of the cystine disulfide bonds, while hair relaxers work to break these bonds apart. How curly your hair is has no bearing on your risk of stone disease, however.
What Is the Problem in Cystinuria?
Patients with cystinuria have an abnormally functioning protein in the part of the kidney that is responsible for reabsorbing cystine (and a few other amino acids). The abnormality is also in the intestine, but this is does not seem to be of clinical significance. Because cystine is generally very insoluble, it precipitates in the kidney and leads to formation of kidney stones. Patients with cystinuria typically begin to form and pass kidney stones in childhood, though later diagnoses can also happen. Compared to other kidney stone types, cystine stones tend to grow bigger and faster, often in both kidneys. A stone that grows to take up a large part of the kidney called a staghorn stone is a particularly troubling, and not uncommon, complication.
What Causes The Disease?
Cystinuria is generally an autosomal recessive disease, so an individual has to inherit two abnormal copies of a gene (one from each parent) that is responsible for cystine transport within the kidney. In rare instances, only one defective copy of a gene may be inherited, but in these situations the abnormal levels of cystine in the urine are lower than in the classic form. This generally means that there is a lower likelihood of stone formation, all other things being equal.
I have been told that I have cystine stones – now what?
It is critical to prevent stone formation in people with cystinuria as these stones can get very big very quickly. Not only do people with cystine stones undergo a high number of procedures and surgeries, but also compared to the more common stone types, their kidney function is more often impaired.
The biggest key to preventing cystine stones (as most others) is to maintain a very high fluid intake. In the case of cystine stones, we can estimate exactly how much a person needs to drink by their total daily cystine excretion, which can be obtained from a 24-hr urine collection – or better yet several. Once we know how much cystine, on average, a person makes, we can determine how much fluid intake is necessary.Typically, at least 3-4 liters of urine are required daily, and often much more than that. Variety helps to maintain such high intakes.
We also know that making the urine more alkaline (less acidic) is a cornerstone of therapy in patients with cystinuria. Some patients with cystine stones have a high urine pH (how we measure the level of acid excretion in the urine) naturally, but others require medication to increase the urine pH. The most commonly used medication is potassium citrate.
In addition, we know that making dietary changes can also help decrease the amount of cystine in the urine, which can help prevent recurrent stone formation. Decreasing the amount of salt in the diet (the lower the better, but at a minimum less than 2300 mg per day) as well as moderating protein intake can be very helpful.
What If Dietary Changes, Fluids, and Urinary Alkalinization Are Not Enough?
Frequent monitoring with 24-hour urine collections is key to make sure that urine cystine concentrations remain in a safe range. In a subset of patients, low dietary sodium intake, increased fluid intake, and urinary alkalinization will still not be sufficient to decrease urine cystine concentrations to safe levels. Others will not be able to comply with the necessary changes despite their best efforts. In those circumstances, your doctors can consider using a thiol-binding medication such as tiotropin or d-penicillamine. These medications may have a variety of side effects, so your doctor will have to monitor your blood tests closely.
The medications act by competition. Two cysteine molecules combine together to make one cystine molecule. The drugs resemble cysteine and can combine with cysteine to form ‘mixed disulfides’ two dissimilar molecules linked through their sulfur atoms. These mixed molecules are far more soluble than cysteine. In principle, one might think such molecular elegance would be a perfect cure, but drugs with free sulfur atoms combine with many kinds of proteins and when they do this the immune system may recognize them and react against them, causing a drug reaction.
Because of such complications, one tends to reserve drugs for those patients who cannot control their stones with fluids, and diet changes. Unfortunately such patients are not uncommon.
Have had this disease since childhood. Had staghorn , left kidney removed at 18 years old. Thanks. Go to hospital almost yearly to remove blocked stones
Hi Paul, Cystinuria surely is a bad stone disease, and loss of a kidney an especial hazard. You already probably know about the importance of nocturnal hydration, sometimes overlooked. Some stone testing vendors have cystine supersaturation – Litholink is one of them. Their testing panel is of particular value for people like you who have so much trouble. You need to keep the 24 hour average SS below about 0.5 to allow for peaks during the night or even daytime. Alkali are worth it, though a weak addition; moderation of protein intake likewise. The thiol drug is very helpful if you are tolerant of it, but I would not rely on it so much as use it WITH hydration, the latter as if there were no drug. Regards, Fred Coe
Yes, stagnorn calculi. At age 21, I had stones removed from left kidney, then right kidney removed. No diagnosis then. Two years later, another stone. I was fortunate to be at Mass General Hospital where a Harvard Medical School researcher was interested in my case and diagnosed cystenuria. Good timing: Cuprimine has recently been approved for treatment. No ill effects from the medication. FIFTY years later, no additional stones and my left kidney is functioning very well. Lucky!
Hi Elayne, Thank you for helping another patient. Of note, modern drugs now are available above cupramine as in the article. Regards, Fred Coe
Thank you for posting this info. I am 38 years old and have had cystinuria with large stones since birth. I am unique as I also have PKD type 2. I currently take potassium citrate and tiopronin and have been stone free for 5 hrs. Thanks
My wife is very sick with these stones. She’s been in the hospital more this year than she’s actually been at home. She passes stones almost once a week. She’s taking Thiola but no luck with it. We need more help if possible…
Hi William, This is a difficult disease in some cases because cystine supersaturation can be hard to reduce and not all commercial vendors produce a urine cystine supersaturation measurement. I have emailed you directly. Regards, Fred Coe
Started having stones at age 6… I have had multiple surgeries and pass them every week… The pain is the worst… I hate this disease…cysteine stones
Dear April, Cystine stones are indeed very serious and hard to control. In my own work the most important part is very high urine volumes day and night + potassium citrate to raise urine pH above 7 + reduced sodium and protein intake, but it sounds like that has not been enough in your case. Your comment does not specifically post a question so I cannot add more. Regards, Fred Coe
Can you give me a general recommendation on when a stone-forming patient should be tested for cystinuria? As I understand it, the nitroprusside test can easily be false-negative, but genetic testing can cost close to $1000, and I’d like to get an idea of when enough suspicion of the disease is enough to justify the costs of testing.
My husband has had stones since age 21 (first stone surgery, unfortunately testing the retrieved stone came back as “inconclusive”) and stone surgery twice. He gets major kidney colic episodes at least twice a year, sometimes more. He hasn’t had another stone tested, although we will be trying harder to catch one. Throughout his life, he has complained of episodes of sulphurous-smelling urine. The doctors always give him antibiotics for this, but urine cultures almost never find any bacteria. This seems odd to me, but I don’t know how often urine cultures fail to culture genuine infections.
He recently had a CT scan ordered because of severe kidney colic pains (again), and there were several 3 – 7mm stones in each kidney. The stones were radio-opaque. They did not find any radio-opaque stones in the ureters, although his kidney colic pain location has been moving lower from the upper flank, to the lower pelvis, for several weeks. Is it extremely unlikely that a CT scan would miss a cystine stone? The doctors tell us the odds of there being a stone that a CT scan misses are almost zero, even a cystine stone.
Does this combination of symptoms point enough suspicion at a cystinuria diagnosis to warrant spending quite a bit of money on the testing, or am I grasping at straws here? I am hoping to find a reason he has such recurrent stones, and has had for so long. Dietary management under Calcium stone assumptions has proved of no value in reducing the number of stone episodes.
Hi Jackie, The sure way to diagnose cystinuria is those stones. Stone analysis will reveal cystine in all cases, along with any additional crystals that might be present. No stone should be inconclusive from a stone lab – in some cases there are no crystals, but otherwise you need a better lab.The nitroprusside test is quite sensitive, actually, and gives false positives. It sounds like the problem here is your physicians are not getting the laboratory support they need and deserve in order to take care of your husband. Here is a pretty good plan for how to proceed with stone prevention. The stones themselves are very important as you have surmised and if the lab cannot get a reliable answer they need to return the samples so a better lab can do the work. Stone analysis is quite routinized and failure to identify crystals is not common. I will correct your type. Regards, Fred Coe
I have had cystinuria for 45 years and for all of that time I have been taking Penicillamine tablets, along with 3 litres of water, diluted juice and weak tea and coffee, which I list each day to make sure I reach my total.
During this time I stopped taking the medication for a while and ended up with staghorn cystine stones which were removed surgically. A couple of other times when my drinking was not good due to traveling, I formed small stones which were removed with laser treatment. Penicillamine has worked for me.
Hi Sandy, Thank you for sharing. The drug is indeed valuable. High fluids are the base of treatment, as you imply, and work well with the drug. As you point out formation of new stones can be rapid and they can become large in a hurry. Regards, Fred Coe
And we’re so very fortunate to have that medication available to us! I just can’t figure out why it’s so expensive.
Our 2-year-old daughter is suspected to have cystinuria. She goes for surgery this week to remove a large, fast growing stone. She does seem to have had all the symptoms in the past, and was septic one week after her first birthday, credited to an undiagnosed kidney infection. We are trying to wrap our minds around this diagnosis. She receives 4 doses of the potassium citrate solution a day, as well as hydrate, hydrate, hydrate. I have 2 questions, that hopefully you can shed some light on. 1. She has not seemed to be in pain for the past year. Once we have this large stone removed, I am guessing that it has been blocking other stones from passing. So, should we expect pain? 2. We also have a 4-month-old son. When we asked if we should have him tested, the doctor suggested just waiting until he’s potty-trained. Is that a general recommendation about this disorder? or do you think we should insist on having him tested? Appreciate your thoughts and time.
Dear Desirae, Cystinuria is an autosomal recessive genetic disorder – almost always – so your son has a 1 in 4 chance of having it. He would have a 50% chance of being a carrier but that is a benign and common situation. I would not bother to test him until later, and a simple spot urine will do – if negative he does not have the disease. As for your daughter the main issue is very high urine volumes for life – as early as possible and given she has had large stones perhaps a thiol agent. This is a disease for peds specialists in cystinuria management and very urgent she have such. Like all stone diseases cystine stones cause obstruction and foster infection, but these grow fast and large and so are very dangerous unless controlled. Warm regards, Fred Coe
My 8 year old, who has a serious metabolic liver disease (Glycogen Storage Disease 1b) was found to have a stone last month, after flank pain, an elevated urine WBC (23) and metabolic derangement that persisted despite her usual GSD treatment. Given her GSD, we assumed it would be uric acid or calcium related, but a 24hr urine profile for Cystinuria was done (sent to Mayo) and all levels were elevated– with arginine and lysine being as much as 3.5x the upper limit. We are awaiting appointments with her geneticist and a new urologist, but are wondering if this one test is enough for diagnosis? She hasn’t passed the stone and an u/s of her other kidney was not performed, so we don’t know what else might be there. Kidney stones run in our family and I have a history of drug resistant kidney infections and hydronephrosis, which makes us wonder about the genetic link. Are there particular doctors you’d recommend for pediatric cystinuria, particularly with medically complex children? Given the seriousness and management required for GSD (which ranges from metabolic crisis to chronic neutropenia and inflammatory bowel disease), we want to have the most experienced doctors to weigh in and be able to coordinate care with her other specialists. Any insight would be great appreciated!
Hi Blair, cystine, arginine and lysine are all basic amino acids and the elevation suggests some transport shared defects, but risk of stone from increased urine cystine depends upon the quantities present in the urine. I believe the GSD is causing what may be minor transport defects and the amounts of cystine are too small to support stone formation. The one test is certainly not sufficient to diagnose a second – potentially unrelated – genetic disease like cystinuria. In Type 1 GSD the common cause of stones is high urine calcium and low urine citrate, and I know of no reported cases of combined cystinuria and GSD Type 1; however I am always willing to learn. If there is doubt about the significance of the urine cystine Litholink Corp – LabCorp subsidiary – produces a urine cystine supersaturation test that is patented to them and very definitive. Ask your geneticist if the amounts of cystine warrant such extra testing. Regards, Fred Coe
Thank you for the insight! I don’t think there is any thinking at this point that the GSD and cystinuria would be related. Her uric acid is well controlled, though her UA calcium was high (this was the original assumption– that these were calcium stones). I’ll definitely ask about the additional testing. It’s possible that the lab that did her whole exome testing might be able to run the Next Gen Cystinuria panel with the sample they have on hand. If that’s the case, we’ll ask about that too. Can a very high protein diet skew the Cystinuria 24hr Profile test? Would it potentially lead to elevated urine amino acids as well?
Hi, Like you I much doubt cystinuria is an issue. Very high protein can increase urine cystine very modestly. The high urine calcium is well known in GSD Type 1. The dibasic amino acids are elevated as you noted, and perhaps this is diet. Overall I am not overly concerned about the cystine. Regards, Fred Coe
I will be starting Thiola and to be honest I am quite scared to take it due to the potential side effects. I currently have a blood disorder of Polycythemia and am worried it could affect me in a negative way.
Hi Lesa, You are prudent given a primary blood disorder. Your hematologist needs to determine safety. He/she has special expertise and can make a proper assessment. The question is beyond the reach of the persons preventing your stones. Regards, Fred Coe
I’m a medical assistant and mother of a 9 year old girl, whom has recently been had a dx of kidney stones. I was able to collect some during her recent hospital stay, they were sent to the lab. No word back yet, but from the appearance of the stones (And continuation of her symptoms) they look like cystine stones. I will shortly be taking her to see a pediatric nephrologist in NOLA, and was wondering what questions etc should I bring up with that doctor. What should I take note of that may make it easier for them to treat her? I’m asking not only as a mom but as a trained CCMA .
Hi Crystal, If the stones are cystine everything depends on keeping cystine supersaturation down. The drugs can have side effects so I always try my best with high fluids, low sodium – reduces cystine losses – and alkali, as well as a normal – not overly high – protein intake. Drugs are an add on when these measures fail. So the diet and fluid measures are up to you, as you imply and as you pursue them it makes treatment with drugs – the medical side – a lot easier and potentially can permit lower drug doses. Regards, Fred Coe
Dr. Fred,
Several months ago I passed around 17 stones over two days. Fun, fun. I knew to get them tested immediately because my older brother was diagnosed with cystinuria, but only after he had had several surgeries, one that almost killed him. He is taking potassium citrate and is still forming stones and has a cashew size stone embedded in scar tissue in his right kidney. That being said, I now have the disease. I have basically become a vegan, but can’t help the urges for animal protein and sometimes cheat. I am former military SF, so by habit I drink loads of water (3 to 4 liters a day) and keep sodium to a min. The problem I am having is keeping my muscle mass and even most vegan/plant based protein powders have cystine from the plants or whatever they are using in the ingredients. My big question is, how do I and many others with this disease get the proper amount of protein to sustain and build muscle mass? Should I be that afraid of steak, eggs, cheese, fish, shellfish and all the best foods in life? I have my first 24hr pee test this week, so I figure that will tell all on my cheating. I do not want to end up on the operating table and feel that this can be managed by diet, but I need PROTEIN! Thanks in advance for your time and response.
Jeffery Reavis
Hi Jeffery, I gather you have cystinuria. Protein restriction is only one of a group of treatment options and not one that will work well for you. Management of this condition is indeed vexing and you should discuss with your physicians whether they might want you to obtain a more specialized consultation to help in planning such treatment. The article on this site is introductory and I am sorry I have not written a more detailed one. Very high urine volumes, low sodium diet, alkali, and even meds all work well together – their effects are additive. Direct measurements of cystine supersaturation are available from commercial testing vendors. Regards, Fred Coe
My 13yr old son had an egg-sized cystine stone removed June 5. August 10 he noticed his urine stream weakening. Is it possibly he could have another stone in that short of time?
Hi Allanda, Yes, possibly. Cystine stones grow rapidly. Be sure treatment is fully adequate all the time! Regards, Fred Coe
Dr. Coe,
Thank you for all the helpful Q&A’s! I really appreciate the help, since this disease is very complex and is sometimes difficult to find answers too. I have cystinuria and have a quick question.
Since Methionine is high in fish/seafood, is fish oil (for omega 3’s) harmful for us who have cystinuria?
Thanks!
Jeffery
Hi Jeffery, This ancient but lovely article shows that feeding homocystine can increase urine cystine and mentions that methionine does the same presumably via conversion to homocysteine. Here is a very modern view of the same thing; there is a well established pathway from methionine to cysteine – the monomer of cystine. So, yes. Regards, Fred Coe
Hi Dr. Coe; First I’d like to thank you for this very informative website. I’ve learned so much from you and appreciate your hard work and the sharing of information you’ve found. Like other kidney stone patients, I’m very grateful to you and for you. As a kidney stone patient, I began having stones only 2 1/2 years ago (I’m years old). As of this year they’re coming fast and steady, at every 2 to 3 weeks, and I am exhausted. I discovered your website as well as Jill’s Facebook page only 2 months ago, after great frustration over the lack of information I was receiving from my urologist. I just received some lab results in the mail. It says that my last stone was “cystine, qualitative”. Does this mean I have cystinuria? It certainly would explain my past several months. My question to you, other than the one above, is that do you think my urologist is giving me adequate care? I see him several times each month this year (and frankly, I cannot afford to visit any longer!) we take a CT kub scan, a urine sample, sometimes sign me up for a shock wave lithotripsy with stent. I’ve been hospitalized in both October and November due to the stent and pain issues. Thanks to your website, I’ve begun the diet and drinking lemon water, had my 24 urine test (very informative!), and I’m told, have had 20 CT kub scans over the past 2 1/2 years, with recommendation to no longer receive them due to radiation over exposure. I feel like I’m running in a hamster wheel with no good results. However, I live in a smaller city (Eugene, Oregon) and this is the only urology practice in our county. I have been forced to cancel my upcoming appointments as I’m so deeply in debt due to the kidney stone costs. I simply don’t know what to do! Would you please consider my situation and make any recommendations that may help me? Or am I at the correct place in this situation? I’m just exhausted and getting no where, hence quite frustrated. Any suggestions would be more than welcome! And please forgive me if this is the wrong platform for me to ask general yet personal questions. I will be ever so grateful for any suggestions and/or recommendations you may have. Thank you very much!
Hi MaryAnn, If you do have cystinuria you need care at a university center. Is there not a stone program at the university in Oregon? I found this one. My advice is to try to get the pictured physician to see you. Cystine stones can grow very fast and be hazardous. Regards, Fred Coe
Thank you so very much, Dr. Coe. You’ve given me great hope!
I was diagnosed via biopsy and blood and urine tests in 2014 with idiopathic hyperoxaluria, but your Web site led me to look back at my last 24-hour urine sample about two years ago. That report found “marked hypocitraturia” with urine citrate at 223 mg/day. My pH was 5.616. At the time of the test I was taking 20 mEq of potassium citrate twice a day (40 mEq daily) for the hyperoxaluria. Since that time my eGFR has improved to Stage III kidney disease. Recently, my primary doctor was concerned about my potassium and suggested I eliminate the potassium citrate. I mentioned this 2016 report to him, and he said to reduce the potassium citrate to 10 mEq once a day. My nephrologist said either no potassium citrate tablets or one 10 mEq tablet per day would be fine. Do I have hypocitraturia, or is this hypocitraturia incidental to my hyperoxaluria diagnosis? Is there a frequency with which I should have 24-hour urine tests? Should I be drinking more water? I now drink at least 84 ounces a day and pursue a very strict diet.
Hi CHristy, you do not mention the urine oxalate. How high was it?? Regards, Fred Coe
Hi Dr. Coe, I was diagnosed with cystinuria (stones are 100% cystine). Is there a doctor and or a dietician you can refer me to in South Florida that specialize is this rare hereditary disorder. I’m in Broward county, Fort Lauderdale area.
Hi Tracy, Your disease poses problems in medical prevention and surgical management, and I do not know of a stone center near you. The university program at Miami is closest and although I do not recognize the faculty perhaps one or more have taken on an interest in your problem. The alternative is travel to a center. You are right in wanting care from physicians who have managed a number of patients like you. Regards, Fred Coe
Hi Dr. Coe,
Thank you for this great website, which is very helpful and informative. I am writing because my daughter, who is 24 years old, has had a very extensive history with cystine kidney stones. She lives in Scottsdale, Arizona, and both her urologist and her nephrologist, have said they have never seen anything like the problems that she is experiencing with cystine stones. She is otherwise a very healthy, active 24 year old, who was a college athlete (she played tennis). She is very health conscious and she exercises every day and eats very healthy. Her first experience with kidney stones was when she was in high school. In the 7 or 8 years since then, she has been hospitalized 8-10 times due to kidney stones and has had at least 40 stones removed. In October, 2016, the had her worst experience to date with kidney stones as she was hospitalized for over a week due to a large, dense stone being lodged in her urether, which lithotripsy failed to make a dent in. As a result, urine backed up into her kidney, causing a severe kidney infection. Her urologist ultimately had to perform a percutaneous nephrolithotomy by inserting a tube into her back that ran into her kidney to remove the stone. He not only removed the stone lodged in her urether, but he also removed approximately a dozen other stones that were in her right kidney. The stones were tested, which revealed that they were 100% cystine stones. As a result, she currently gets an ultrasound and an x-ray every six months because her stones get so big so fast. In March, 2017, her urologist removed another dozen or so stones that were in her left kidney.
Despite drinking approximately 100 ounces of water per day and taking potassium citrate for six months, the ultrasound/x-ray that she had in September, 2017 showed that she had developed a 1.3 centimeter stone in her left kidney in the past six months. Consequently, her urologist went in and removed this stone in October, 2017. Every time she has stones removed she has to get a stent that remains in for approximately a week and usually causes her a lot of discomfort and pain. Within the past week, her doctors discovered that she now has a large stone approximately 2 centimeters in her right kidney and a similar size stone in her left kidney, both of which developed just within the last six months. This is despite being on Potassium Citrate and Sodium Bicarbonate. She was also prescribed Thiola, but had to discontinue taking this drug to because she developed severe rashes and itching. Her cystine levels are fairly high, as her 24 hour cystine excretion for a 24 hour period is about 1,000 mg. Her sodium intake (Na) intake is 160, which I understand is not too bad.
These cystine stones are causing her to suffer every time she has a procedure done, and appear to form at least every six months. Her doctors in Scottsdale do not seem to have any answers, and we are desperate for help. Any suggestions that you can provide would be tremendously appreciated! Thank you for taking the time to read this and respond. Lee.
Hi Lee, When cystine stones come so often and so fast despite apparent high fluid intake and meds to raise urine pH the problem us usually some indeterminacy in fluids over the day or night, or perhaps, the fluids are not enough to lower cystine SS far enough given the amounts of cystine she loses in her urine. This is complex because figuring out the former needs some finesse – people often miss a critical period even when very smart and trying hard. Overnight may be the worst of it. I can offer to see her, which might just be worthwhile, but apart from that I am really too far away to be of any significant help. You are right – this situation cannot be left as is. Regards, Fred Coe
Hi Dr. Coe. Thank you for your response. I would like to make an appointment for her and I to see you. What is the best way to do that? Lee.
Hi Lee, My secretary is Kathleen Dineen 773 702 1475; tell her how you got to me and that the problem is cystinuria. If your daughter has not had cystine evaluation via Litholink, we need to get it from that company or do it here. It is special testing. Please check. My private email is coe@uchicago.edu. Regards, Fred Coe
She needs to watch her salt intake and reduce the amount of animal protein. Also, add 2 tablespoons of lemon juice to each liter of water she drinks each day, which should be about 5 liters. I am 53 and have had over 50 operations to keep my kidney stones at bay. My left kidney is now very small. You can stop the stones by taking penacilamine, but there can be some side effects – you would need to investigate this.
For those of us with cystinuria, what is the ok amount of animal protein that we can consume daily? I have suffered with this disease for 20 years now, I have had several different types of surgeries (10 surgeries in 10 weeks) to rid the egg sized stones in each of my kidneys. I have been to several university studies with no more information given than my regular urologist. I live in Missouri and have even went through director of urology Barnes hospital St. Louis, MO as my doctor. But still not finding any different treatments or meds than my urologist hadn’t already told me. I am now going to attempt to take Thilo to see if I can tolerate it. Otherwise, if this does not work, what other medicines or treatments should be tried. I have already taken the Urocit-K (80 mEq) daily. Can not take the depencinalamin as I am allergic to penicillin. Any suggestions?
Hi Juanita, The secret in cystinuria is to measure urine cystine supersaturation and use it to guide fluids, alkali, and drugs if needed. Only Litholink sells such a test, but it is excellent and you need it. Usually it takes 4 or more liters of urine volume a day to bring supersaturation down, and enough potassium citrate to raise urine pH near 7.9. As for protein intake, go to the lower edge of normal – 0.8 gm/kg/d. If you can achieve a SS below 0.5 with these measures stones should abate. If not, consider the drugs. Remember, fluids – urine volume – needs be high all day and you need to get up at least once a night to keep from making crystals. Regards, Fred Coe
Hello, I am currently living in the Philippines. Retired here in July 2016. I was living in Augusta, Ga where I was diagnosed as having custine stones in my left kidney. The Army hospital there removed two stones that were blocking the urethra. In November 2017, I had another attack, same problem, same kidney. The stone was extracted an having heard horror stories about wat kidney stones look like I was shoked to see that the stone appeared to look like a pebble. I went a while without problems and in Dec 2017, I had another attack..one stone about 8.9mm. The Urologist here suggested doing shock wave treatment, in Jan 2018 had the procedure done and all went well. Begining Feb, I had another attack, this time they found three stones, again in my left kidney. The big on blocking th urethra was 1.8 CM..the other two were higher in the kidney smaller one is 6mm and the one next to it 8.9mm. The 1.8 was again addressed with shock wave and a stent placed in the urethra. Painfull. Went back to check the status of the stones two weeks later, and apparently the large stone broke into two large horizontal sections. The top half was pulverized while the second joine the other two in the higher position..last week we again used the shock wave to address the larger stone..if this went well they will yet again use shock wave to attempt to pulverize the two smaller stones. I was put on strict diet, given 15mg potassium citrate 3 X a day, and I have begun to drink approximately3 1/2 lt of alkaline water 9.4 ph a day..are all these shockwave treatments dangerous to my kidney? My left kidney seems to be the only one involved in the production of stones. Anything more I can do? Thankyou for reading this long dissertation.
Hi Sal, Cystinuria is a complex disease. Treatment is based on very high urine volume – up to 4 liters or more a day and throughout the evening and night. The potassium citrate is good. The big problem is to keep the hydration steady as stones can form rapidly. If things continue with so many surgeries, there are medications your physicians can use. Regards, Fred Coe
Hi Dr. Coe,
I have two questions regarding my followup with my uroligist.
1. What type of evaluation or screening and test do you recommend for those of us with cystinuria?
I know that the Litholink 24 hour urine sample for cystine stones is recommended, but now often should this be done a year. What about ultrasound, xray or c.t scan. I’ve read that the xray has low to no stone visibility and c.t scans are better but should be limited due to exposure to radiation. Is this correct? What about ultrasound?
2. How often should one have these follows up with doctor if one is not presently in any pain?
Thank you
Hi Tracey, The Litholink testing is ideal; I founded the company and designed their special testing. LabCorp now owns it but continues this important service. I would try for a supersaturation below 0.5 and have ultrasound to follow stone size and number. CT is a lot of radiation and I would limit them to no more than yearly or even less depending on the US results. Be careful to keep fluids high and even throughout the day and night. Regards, Fred Coe
Hi Dr Coe, whether are cystinurea and other amino acid reabsorbtion and excretion cause of defeciency of them in body and consequently some due complications?
Hi shramee, in cystinuria blood levels of cystine may be low, but I know of no complications from that. Other diseases involving loss of amino acids vary from benign to serious, so I cannot say in general, but they do not cause stones. Regards, Fred Coe
Hi Dr. Coe,
I am a dietitian. Can you please tell me the physiology behind limiting sodium for Cystine stone formers? I understand the rationale for other types of stones with the relationship to calcium, but I would like to understand it here as well. I like to be able to explain the mechanism to my patients simply so they can understand the “why” of the restriction.
Also, I am having a very hard time finding reliable information for methionine levels in food. What do you use? Would you say that as long as a person is keeping protein to 0.8 gm/kg, this will help keep methionine levels in check? Is 0.8 gm/kg your recommendation for the general Cystine stone forming population?
In a nutshell – adequate fluids to produce 3-4 liters of urine output, consistent fluid intake throughout day and even upon wakening in the night, low sodium, avoiding excessive protein – is this the diet advice for this patient group?
Lastly, I have a patient, Cystine stone former, that adds a BCAA supplement to his water. I understand methionine is not part of the ingredients, but I still feel uncomfortable with it. Any thoughts in particular to Cystine stone former and this type of supplement?
Thank you thank you for your continued guidance!
Hi Marilyn, Cystinuria arises from a defect in one or another proximal tubule transporter. Low sodium diet increases total PT sodium and water reabsorption via increase in angiotensin 2 activity (and probably increased sympathetic nerve traffic as well). The overall increase will increase all amino acid reabsorption as a byproduct, cystine included. The diet sodium is, as you know, not low but at the present US optimal of about 65 mEq/day. BCAA do not include cystine and do not produce it, so I think it is irrelevant. Warm Regards, Fred
Dr Coe,
Our daughter has just been diagnosed with Cystinuria and her doctor immediately wants to put her on medication. She is 22 years old, college athlete and otherwise very healthy. She had her first stone in Jan and has since passed 7 other stones. This is has a total shock to us all. I am worried about the long term effects of the medication. Should we try diet changes and fluid intake first? Would you consider evaluating her? We live in NC but will do whatever we need do to make sure she receives the best possible care. Thank you.
Hi Beverly, I would advise using Litholink cystine testing with supersaturations – one of their routine commercial products. Fluids enough to keep 24 hour cystine supersaturation below 0.5 should reduce stone formation well in most cases and perhaps make the drugs unnecessary or at least permit very low dose. Monitoring the drug, if used, also needs the Litholink testing as only they have systems the drugs do not interfere with. Your physician can place the order as a special kind of stone testing, and your and your daughter can read the cystine SS values as well as s/he. If things seem complicated, you can of course come to see me and I can take care of all this for her. Regards, Fred Coe
Just curious… I was diagnosed with Cystinuria 30+ years ago when my family was routinely screened after my sister was diagnosed with it after having kidney stones. I’ve never had a stone, nor do I take mispotcit anymore (stopped that 10 years ago) and I don’t follow a low sodium, low protein diet. I drink about 2l fluid a day. My count was vey high when diagnosed and doctors couldn’t understand why I never formed stones. How common is it to have asymptomatic Cystinuria – I ask as I can’t find much info on it?
Also, is there a link with memory issues? In the last 6 years or so, I’ve noticed my memory has small blanks in it that only after prompting, do I start to recall what I forgot. It worries me as I used to have a really good memory. Only other medical info that’s a little unusual is I have asymptomatic hypotension (92/60) and had pre-eclampsia (235/140) with my first pregnancy. I mention these in case there’s an underlying thread. Thanks in advance.
Hi Deirdre, screening positive may not mean real cystinuria, but I gather your 24 hour urine cystine excretion rate was measured and found high. How high matters a lot, as stones are a mechanical consequence of too much cystine to dissolve in the urine volume produced. Your physicians need to be sure how much urine volume you need to undersaturate your urine. Litholink performs excellent cystine testing and I would recommend you get a 24 hour urine done by them for this. If you already did, they provide a cystine SS value. Just because you never formed a stone does not mean you will not, and if you have not had imaging you may have one. So be sure of all of the forgoing. Regards, Fred Coe
Dr. Coe
I have recently been forming cysteine bladder stones in the past 3 years and now have completed my 4th operation to have them removed. Size of a quarter. My younger brother and older sister have developed these types of kidney stones for years (since their twenties-they are now mid fifties and sixties). My other brother had his first bladder stone operation but it was uric stone. Mine have all tested to be cysteine. My brother and sister have been on potassium citrate for years and have not developed bladder stones.(but have had kidney stone operations infrequently). I have discussed recently with my urologist about going on potassium citrate but he states that is for kidney stones not bladder stones. I have increased my water consumption after this recent surgery. Should I try Crystal LIght, or bicarbonate tablets. Otherwise, I am in excellent health and taking no other medication. I really don’t want to start pill medication if i can avoid it. Seems like the lemon juice in water would work also to help me. With extremely busy worklife, it is hard to get this water down during the day but I am committed to trying a program. Each surgery costs me my deductible approximately 2k a year. My urologist seems hesitant to do anything regarding this. My recovery from surgeries is instant so it has not been a problem. I will be turning 60 soon but don’t want to continue the surgery route. Thiola seems interesting but extremely expensive! all these routes of medication see expensive. Is there a diet program for lowering cysteine. My wife is lost and needs help. I am not a big meat eater, just occasionally, and typically only eat one meal a day. Vegan diet seems like a big lifestyle change though. We live close to chicago and UM in AA. thanks for this webpage as i am becoming more proactive in my care. Should I get a second opinion? It is a respected doctor who has helped me with stricture issues, prostate cancer, etc. etc. but i dont get the hestitancy towards trying to treat this.
Hi Dan, You have cystinuria, it is in your family, and you would benefit from more stable and focused prevention aimed at cessation of more stones. If you can come to Chicago, we can provide for you. Our secretary, Karen Niswander, is at 773 702 1475. She can arrange for you. Regards, Fred Coe
have been diagnosed with Cystinuria. I live in Orange County CA which is near Los Angeles CA.
Could you suggest a nephrologist or a center in this Area who is versed in the management of this condition?
Hi Anne, Your condition can be controlled very well, but you should be in a university based program. I believe UCI is in Orange County. Dr Ralph Clayman is a superb talent and friend of mine who I would contact for help. Feel free to use my name as a reference. Regards, Fred Coe
Dr Coe,
I am not sure if it is appropriate to ask my question here, or in private. Please remove this message if it is inappropriate.
As someone with homozygous cystinuria I am interested in finding out what causes the condition’s severity to be so highly variable, and why it tends to have a more severe course in males. (Beyond structural abnormalities, and the fact males have a longer ureter etc.)
Have you, or any other researchers, noticed – if only anecdotally – anything similar between cystinurics who are more severely affected, and cystinurics who are less severely affected? (Traits or circumstances which may seem unrelated to the condition such as height, personality, disposition, alcohol consumption etc.)
When I was first diagnosed with cystinuria I read about an androgen-dependent form of the condition which affects certain breeds of dog. For those unfortunate animals, they are at least lucky in that the cystinuria can be cured by medical and surgical castration.
Unless I am mistaken, my understanding is that humans do not have an equivalent androgen-dependent form of cystinuria, and so there is no equivalent cure.
However, as a layman I still wonder: Have serum sex steroid hormone levels been investigated with regard to cystinuria and differences in disease severity (e.g., stone size, frequency, cystine excretion levels, cystine crystalluria)?
While there may not be an androgen-dependent form of cystinuria in humans, do you think it is possible that testosterone could still play a role in disease activity – and severity – for at least some cystinurics? Do you know if testosterone levels have been studied in humans with cystinuria, and ruled in or out as a factor with the condition?
If there is anything you can talk about along these lines, please do so!
Regards,
Peter
Hi Peter, In a brief look in PubMed under cystinuria and androgen, I found no useful article. Under cystinuria and sex I found this recent article showing a higher prevalence of hypertension among male cystinurics age 16-40; I found this rather nerdy article on cystine solubility being lower in male urine and some fancy measurements to try to find out why. This article and the preceding one mention that males have a worse course vs. females as if it were received wisdom, and this confirms your question. In fact, cystinuria has a variable course vis renal disease even though the genetic causes are few and well defined. But no articles mention the male sex hormone per se as crucial. Regards, Fred Coe
I have a dog with cystinuria. From what I’ve found in my research, the androgen dependent type is only found in canines. I just neutered my Pointer a few months ago and hoping it works!
But you may want to contact Dr. Giger and/or Dr. Henthorn at UPenn. They study cystinuria and may be able to answer this question more definitively for you.
Dr Coe,
Many thanks for your reply. I have had a chance to review each of the PubMed articles and no doubt will have questions in the future since the condition is, alas, a lifelong companion. For now, may I simply ask if you know of someone in Australia with expertise (or an interest) in cystinuria? Although I reside in Queensland, if you know of anyone in Australia, it would be a good start!
Regards,
Peter
__
To Christine,
I hope that the neutering of your Pointer proves to be a permanent cure! Thank you for the two names, I will pursue them. I am curious to learn how and why neutering can cure the androgen-dependent form of the condition.
Hi Peter, It is far away and I know no one to recommend. But in general for such an uncommon disease a university based physician is better as more likely to have accumulated experience. Regards, Fred Coe
My son wasdiagnosed with cystenuria at age 4 and is now 23. He has been passing stones much more frequently lately. Could this be related to his using whey protein powder.
Hi Alex, Cystinuria is an inherited disease of renal amino acid transport. Marked protein loading can raise methionine and cystine absorption and worsen urine cystine excess. Whey does indeed contain considerable methionine – processed to cystine. I would stop it. Regards, Fred Coe
Thank you. I will pass this in to my son.
Dr. Coe,
I’m from germany and had my first kidney stone in march 2019 (Age 36) which required no surgery. They send the stone to the lab and said it is an Cystin Stone. I’m not sure but my urologist said he does not think is it Cystin. I do not have a chance for a second lab check. The only thing I have is a self made picture (https://imgur.com/a/OreNQyS). The stone was about 1cm/0,4inch. It looks like we do not have this much 24h urin check ups since no one does it. Do you know if there are more stones growing – are they grow in the same kidney or any tips how to detect if it was an Cystin stone? Thank You.
Hi Christian, The lab found the stone to be cystine, and it looks that way, so let’s assume the lab is right. Cystinuria needs treatment. If you cannot get 24 hour urine cystine excretion measured – remarkable given that Germany is a very highly advanced country! – assume that is the correct answer and maintain a very high urine volume – 4 liters/day of urine if possible, and add either potassium citrate medication (your physician needs to do this) and/or considerable fruits and veggies to raise urine pH and thence cystine solubility. CT scanning is ideal to detect these stones, and ultra low dose machines have so lowered radiation that risk is minimal. Be careful because these stones can grow rapidly and become very large. As for your physician, perhaps he knows something I do not as he seems to believe the lab is incorrect. I would discuss this with him/her, because cystine stones are very easy for labs to identify. Regards, Fred Coe
Hi Dr Coe, my beautiful 9 month old baby has found to have cystinuria incidentally found during a urine metabolic screen. So far asymptommatic. I’ve scared myself silly reading online and worrying about his future. Can we control this? Is there hope for new medications/treatment in the future? Do people manage an ok quality of life? I need some Hope here. Thanks for your time.
Hi Erin, Yes; cystinuria can be controlled, people grow up normally and can live long lives. But you should seek medical care for your baby at a center that has expertise in this disease. The screen may not be the full cystinuria but just the trait – heterogeneous not homologous – and if so it is without any risk at all. I do not know where you live but if I did I could try to suggest places for you. Regards, Fred Coe
Thanks Dr Coe
I live in Sydney. Still waiting for genetic results but our specialist feels it’s likely homozygous given his cystine level was 400.
Hi Erin, He does indeed as that is a lot of cystine. Nothing works so well as high fluids, from the beginning. Likewise a diet rich in fruits and veggies – as possible over time – to maintain high urine pH. You need a specialized clinic for this problem, as it is not common. Fred
Hi,
Ì was diagnosed with Cystinuria at the tender age of 16. Since then I have lived with or more correctly struggled with the disease and the impacts on my life and career. It has stolen many important moments in my life and the prevalence of stones is increasing as I get older. I’m now 42 and currently have 3 stones in my left kidney 2x 17mm and 1x 10mm.
My question is why is the recurrence increasing.? Im overweight and over the past 12 months have embarked on a weightloss journey, lower in carbs and higher in protein, is this the cause? Should I be considering a vegetarian diet? I take 150mg captopril per day under the instruction of my Nephrologist, but they are getting bigger and more regular.
Any suggestions would be welcomed.
Thanks
Melinda
Hi Melinda, Cystinuria is a very complex stone disease, and measurement of urine supersaturation with respect to cystine of great value. In the US Litholink provides this measurement and I would suggest it be made for you and used as a gauge of treatment success. I am free to recommend this special test and company even though I was its founder, as I nor my family have any present financial relationship to Litholink which is owned by LabCorp. Ask your physician is she/he is in favor of this. Regards, Fred Coe
I’ve finally after 8 years and 5 operations been diagnosed. I am under the amazing team at Guys Hospital in London. My question is what is a safe urine oh level for someone with cystinuria? I am ranging from 6-8 throughout the day?
Hi Samantha, cystine solubility increases with urine pH up to above 7. The problem is calcium phosphate crystallization, but if you are maintaining a very high urine volume – hopefully – and do not have high urine calcium – determined by 24 hour testing – a high steady pH around 7 or more is beneficial. Regards, Fred Coe
Hello Dr. Coe. I a m a 60 year old male who was diagnosed with Cystinuria 30 years ago. I actually saw you as a patient at University of Chicago referred by Dr James Lingeman after he performed a number of stone removal procedures. I was hoping to get a referral for a nephrologist with some experience with the condition in the southeastern Michigan area. Please let me know if you have any recommendations?
Thank you, Michael
Hi Michael, I am afraid I do not have a name in mind, exactly. Perhaps south east Michigan is closer to Indianapolis than Chicago and Dr Lingeman can provide care. Sorry. Regards, Fred
Check out the International Cystinuria Foundation Facebook, and website. The facebook site is a closed group, but we have over 1000 members. This question comes up often in our group conversations.
Hi Kathryn, Good advice, thanks for posting it. Regards, Fred
Hello Dr Coe. Is it possible for someone to have cystinuria but to not produce/pass stones?
In our family, two of my children have cystinuria (both produce stones regularly). This means that I am a carrier of the gene. My mother is in her mid-70s and is then (by extension) also a carrier (we know there are more people in her close family with cystinuria). She has never had any stones (that she’s aware of). She hasn’t been tested for cystinuria.
However, she has frequent kidney infections (three/four times per year) that make her really unwell.
She experiences fever, chills, weakness, slight nausea, frequent urination, high blood & high leukocytes count in urine.
She doesn’t experience flank/back pain/renal colic, though.
Her doctor prescribes antibiotics that clear up the infection.
I wonder if the underlying problem here might be kidney stones/cystinuria?
Would you recommend a CT to check if there are some stones lying in her kidney that are triggering this recurrent issue?
Do you think it would be worth requesting a 24-hour urine test to confirm that she has cystinuria?
Thank you in advance for any advice.
/Maria
Hi Maria, the easiest way to determine your mother’s risk is a urine test for cystine. Carriers have low levels usually and cannot make stones. It is true some are higher. A CT is also reasonable – ultra low dose protocol works for stones. Regards, Fred Coe
Many thanks. We’ll try to arrange a CT to check for a possible stone. Her doctors have ordered various scopes/tests in recent years to determine why she so frequently has blood in her urine and her regular UTIs. No cause was identified.
But she hasn’t been checked for stones/cystinuria. We’re only now suspicious that it might be the cause because of the recent diagnosis in the grandkids.
Thank you.
I have Cystinuria. I’ve known since I was 24yrs old when I ended up in the ER with an obstructed 15mm stone that the bypassed for 4 months with a tube until insurance agreed to let them do lithotripsy on me. I’ve since had several more lithotripsies, nephrostomy tubes (again waiting 4 months) until they approved basket retrievals and so many things I can’t even remember anymore. I’ve been abused by physicians who decided I was being a baby and did a basket retrievals while I was in a storage room without any pain medication whole I screamed in pain. A nurse even quit stating, “I’m didn’t sign up for this garbage”. Anyways, I’ve passed a couple dozen stones a year for awhile there. I wasn’t talking care of myself. Depressed over losing my business because I was hospitalized over and over while passing stones and being treated for infections. I’ve nearly died several times. Septic infections the first time. Took months to recuperate. I’ve had many IV antibiotics and fluid for dehydration. Central Line PICC lines. At home for 3-4 months at a time on an IV. I’m on SSI now and the depression from it is keeping me in bed 98% of the time. This disease has taken my life and after a couple dozen physicians either not educated or caring enough to take care of me I’ve given up. I read everything I can and been guinea pigd so bad by one Dr that my stones went from cystine to calcium oxalate after told to take huge amounts of C vitamin for months I became completely impacted on both sides. Then this quack did a stone analysis, saw I passed a calcium stone and yelled at ME telling me I’m drinking too much milk and get out of his office!!! I could write a book! Ha! After all this the only treatment I’m doing now is trying to learn how to drink so much water I float away and stones float out. Any advice you have I’d be interested in though. Thank you, Sandra Eileen
Dear Sandra, If your stones have been cystine, and you passed a calcium stone perhaps it was a lab error – mix up with another patient, or perhaps calcium phosphate if you take large amounts of alkali for the cystinuria, or perhaps other errors, but withal your care has not been ideal. I would think your physicians might want to obtain a second opinion for you or refer you to a center for stone disease. If you say where you live I could suggest possibilities. Regards, Fred Coe
I’ve been dealing with this miserable existents of cystine stones for 45 years! I’ve been laught at, ridiculed, even thrown out of emergency rooms by incompetent doctors. Someone help us poor Bastards who suffer every day!!!!!!
Hi Stan, Cystine stones are indeed preventable, and hardly a matter for mirth or other bad behavior. I would seek consultation at a referring center and get proper treatment. Because of COVID all of us do telemedicine so you can have your pick. Fred
Hi Azisman,
Thanks for sharing this post. I must say this is the best article I have read on Cystinuria ever. Please I read that cystine solubility increases with ph of the urine. How true is that?
Hi Imtiaz, it is true. Potassium citrate to raise urine pH is part of conventional cystine stone prevention. Regards, Fred Coe
I’m so glad I found this article. I was just diagnosed with cystinuria after major kidney surgery to remove stones at 45 yrs old! I’ve had 6 surgeries so far this year. I had a nephrectomy tube for 6 months and have been hospitalized numerous times for sepsis. Ive been through a lot this year in every aspect of my life…so I’m glad when my newest urologist was able to finally remove the stones and save my kidney. He also was able to diagnose me and has prescribed Potassium for me. He said he’s never had a patient with cystinuria and he is very committed to getting me well and improving my quality of life. I’m very fortunate for that because before I was referred to him I couldn’t see the light at the end of the tunnel and felt like a Guinea pig for my previous Dr. I’m actually from Chicago and now live in Georgia can you recommend anyone in Georgia that maybe my Dr can consult with on suggestions for my treatments? I’m just sooo ready to get back to my life especially my 7yr old son. Thank you in advance for any recommendations you may have.
Hi Nijiysha, cystinuria needs special treatment. The author of the study you read, Dr Anna Zisman, does all of our cystinuria work. Her secretary is Banita Williams 773 792 1475 – and she can arrange a telemedicine consult for you that can help direct your physician as the drug treatment for your condition. Regards, Fred Coe
If my brother and sister have cystinuria does that mean I do also and just haven’t had stones yet or do I just have The faulty gene from our parents?
Hi Lidia, It means you are most likely a carrier for the trait. Your physician can order a urine cystine screening test and find out. Regards, Fred Coe
Hi my son has his first stone at just 8 months he is now 18 months know we are still weighting on janetics test to confirm he also gets red hands and feet do enyone els get this?
Hi Tez, Cystinuria is diagnosed from high urine cystine and from the stone composition. I presume that is why you wrote on the cystinuria page. Genetic testing is informative but not specially important for treatment. Red hands are not part of cystinuria. Likewise your note does not make clear if indeed he has cystinuria or some other stone disease. Usually causes of stones in infancy can be diagnosed from urine collections. Regards, Fred Coe
A Significant and Sustained Reduction in Cystine Excretion?
I hope you are doing well, and I also hope this isn’t too long. Over the past 70 years, various pharmaceuticals and supplements have been investigated to reduce cystine levels in cystinuric patients, with limited success and inconsistent results across studies, albeit typically on a small scale. It’s been suggested that modifiable environmental factors may partially account for variations in cystine excretion among cystinurics, alongside unidentified genes.
As we approach 2024, penicillamine remains the sole treatment for cystinurics in Australia to reduce cystine excretion and thereby suppress further stone formation, given adequate urine volume. This is the reason for my reaching out: I am seeking your initial reaction. In your experience, does the reduction in cystine excretion shown in the table below align with what is observed in patients under standard treatments like penicillamine or tiopronin? Or does it more closely reflect the variable rate of cystine excretion in untreated patients? Here, ‘untreated’ refers to having not used thiol medications, alkalising agents, or undergone urological procedures (despite the passage of cystine stones up to 6 mm), and having not made any specific dietary adjustments (e.g., reduced sodium, protein, methionine intake).
The table below includes two key columns: “Cystine per gram of creatinine,” showing actual amounts, and a hypothetical “Cystine concentration per 3 litres of urine” to contextualise the excretion values, considering a daily urine output of 3 litres is sustainable for many motivated cystinurics.
Considering these data (9 measurements over 6.5 years) and momentarily overlooking the inherent limitations of observational data for a single patient, might we tentatively infer that pharmaceutical agent ‘A’ significantly reduces cystine excretion (in this one case)? Or are these variations within the expected range for the natural course of untreated cystinuria? If not due to the consistent use of ‘A,’ what other explanation could account for these data?
I apologise if the forum’s font has affected the table’s alignment and readability. If you copy and paste it into a text editor with a fixed-width font, it should become clear.
+———+———+———+———–+———————–+
| | Urine | Cystine | Cystine | ‘A’ | Cys mg/L if |
| Date | Vol (L) | (mg/L) | (g/Cr) | Status | urine 3L/Day |
|———+———+———+———–+————-+———|
| 2017-06 | 5.65 | 642 | 1887 mg/g | NO | 1209 |
| 2018-06 | 5.25 | 153 | 469 mg/g | YES | 268 |
| 2018-09 | 5.5 | 142 | 569 mg/g | YES | 260 |
| 2020-02 | 5.81 | 137 | 502 mg/g | YES | 265 |
| 2020-12 | 4.31 | 137 | 336 mg/g | YES | 197 |
| 2021-09 | 5.5 | 205 | 583 mg/g | YES | 376 |
| 2022-03 | 5.27 | 127 | 402 mg/g | YES | 223 |
| 2023-05 | 2.98 | 343 | 522 mg/g | YES | 341 |
| 2023-12 | 2.96 | 936 | 1590 mg/g | NO | 923 |
+—————————————————————–+
NO = ‘A’ not administered for several consecutive months prior to the 24-hour collection.
YES = Daily administration of ‘A’ for several consecutive months, with varying doses before some of the 24-hour collections.
Overall, the table indicates that consistent administration of pharmaceutical agent ‘A’ correlates with a notable reduction in cystine per gram of creatinine and overall cystine concentration in urine, particularly when compared to long periods without ‘A’s administration, suggesting a potential impact on cystine excretion rates.
The first and last 24-hour measurements, when ‘A’ was not administered for several consecutive months, indicate a urine volume significantly over 3 litres is necessary to prevent or delay further cystine stone formation. Hence there is some urgency to my reaching out to you.
If you find ‘A’s apparent effect intriguing, I can share additional details via email, including any medical records (full 24-hour collection results, CT scans, etc.) for verification. Currently, I’m looking for an unbiased initial impression: could there be potential in ‘A’?
Regards, Peter
P.S. Rest assured, the mysterious agent ‘A’ is neither ‘chanca piedra’ nor the notorious Radithor of yesteryears; it’s a well-established prescription medication with a long-standing history in clinical use, typically outside of the scope of kidney stones.
Hi Peter, It looks very convincing to me. I presume it looks so to you as well. Thanks for sharing, Fred
Thank you for your response, Dr. Coe. The data does look very convincing to me. The two highest cystine excretions correspond with periods without ‘A’, and my calculations suggest a less than 3% chance of this being coincidental, leading me to reach out.
I’d like to mention ‘A’ via email, especially since it has become somewhat “politically incorrect” (it is a cheap medication that used to be available over-the-counter). My ideas on its efficacy in reducing cystine levels are speculative (and I may be wrong, and it may all be a wild coincidence), so your insight would be greatly valued. If ‘A’ effectively lowers cystine levels, at least in severe cases, it could be an alternative to high-dose CBTDs like penicillamine, which is often poorly tolerated.
May I email you? Or, if you prefer, feel free to contact me at the email address associated with this reply.
Regards, Peter
Hi Peter, The topic is not without interest, but is more or less in the realm of research than clinical care. Even so I have a partner with a special interest in cystinuria. Feel free to email me. I will be vacationing for February but will try to answer you. If it seems of potential interest and we can be of help I or my partner can correspond with you. I will not disclose your compound without your permission. But I cannot guarantee strict confidentiality as I am using a common email platform. Regards, Fred Coe
Apologies for the formatting issues with the table in my previous message. Below is the same data presented in CSV format for clarity:
Date,Urine Vol (L),Cystine (mg/L),Cystine (g/Cr),’A’ Status,Cys mg/L if urine 3L/Day
2017-06,5.65,642,1887 mg/g,NO,1209
2018-06,5.25,153,469 mg/g,YES,268
2018-09,5.5,142,569 mg/g,YES,260
2020-02,5.81,137,502 mg/g,YES,265
2020-12,4.31,137,336 mg/g,YES,197
2021-09,5.5,205,583 mg/g,YES,376
2022-03,5.27,127,402 mg/g,YES,223
2023-05,2.98,343,522 mg/g,YES,341
2023-12,2.96,936,1590 mg/g,NO,923
Alas, I am unable to reply to my previous comment to correct the table as it is not yet approved.
Hi, I was diagnosed with cystinuria a few years back and have had to get a PCNL surgery to remove a staghorn stone. I was wondering what the impact of running is on people who have cystinuria? I love running and want to train for a marathon but have not been able to find any information regarding how it may impact my kidneys.
Hi Christine, this disease is very dangerous as stone are often large and damage kidneys. Your physicians need to determine the magnitude of the saturation from cystine and use either fluids and diet or one of the available drugs. As for running it is not unreasonable but fluids are vastly important to avoid new stone formation which can occur very rapidly. Regards, Fred Coe