
by Dr Fredric Coe | Jun 10, 2018 | Uncategorized
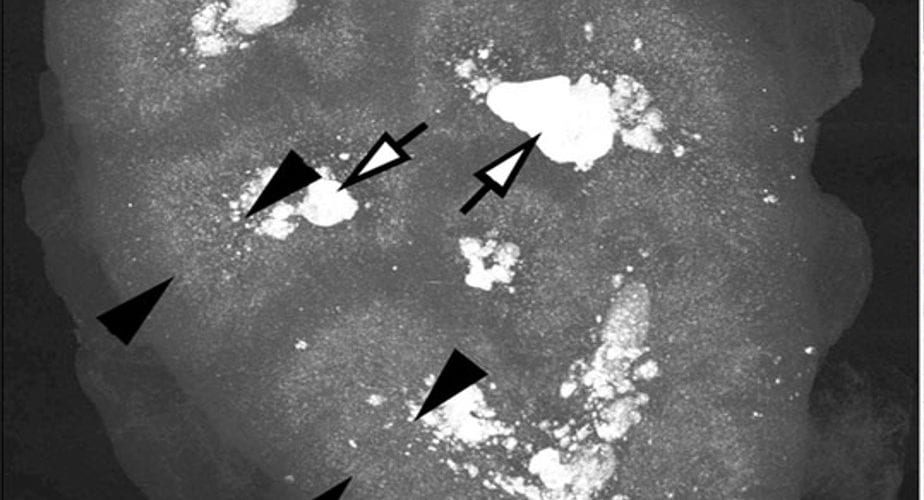
Every stone former needs fasting serum and 24 hour urine testing. Likewise important, kidney stone analysis and review of images – CT scans especially. Medical evaluation is what physicians do. They integrate the testing with the history of stones and everything...
by Dr Fredric Coe | May 11, 2018 | CASES, For Doctors, For Patients, For Scientists
Bariatric surgeries can injure kidneys by raising urine oxalate excretion. This latter causes kidney stones, and raises risk of acute and chronic oxalate nephropathy. Overall, their benefits far outweigh these risks, especially when patients and physicians take proper...
by Dr Fredric Coe | Feb 15, 2018 | For Doctors, For Patients, For Scientists
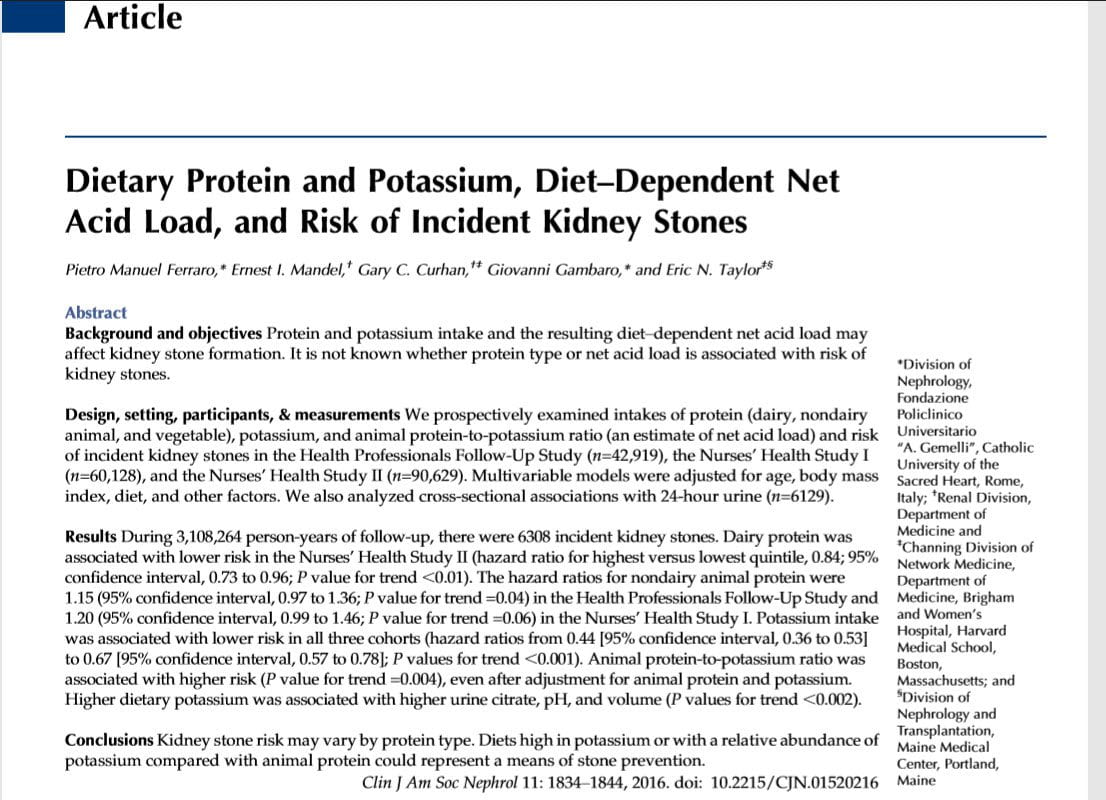
Gary Curhan and Eric Taylor have given us many insights into how diet might influence kidney stone risk. I think this new article by them and their colleagues a great opportunity for close reading and practical use of a high quality research paper remarkably germane...
by Dr Fredric Coe | Jan 2, 2018 | For Doctors, For Patients, For Scientists
Unfortunately producing stones means higher risk of hypertension and kidney disease. But most of the diet changes and even first line medications for stone prevention also lower blood pressure. Here is how that works. The featured painting, Vincent Van Gogh, The...
by Dr Fredric Coe and Jill Harris, LPN | Nov 6, 2017 | For Doctors, For Patients, For Scientists
Elsewhere we have described an innovative web based course aimed at reducing kidney stone risk factors via improved diet. Briefly, the course helps patients whose physicians have prescribed diet and fluid changes implement those changes, by teaching them to choose the...