
Case 5: Severe Hyperoxaluria
Severe hyperoxaluria – always worrisome, never something to dismiss or even wait a long time thinking about. The Vegetable Seller’ by Flemish painter Joachim Beuckelaer (c.1534-1574) seems a perfect image for this exercise in vegetable excess. He was never...
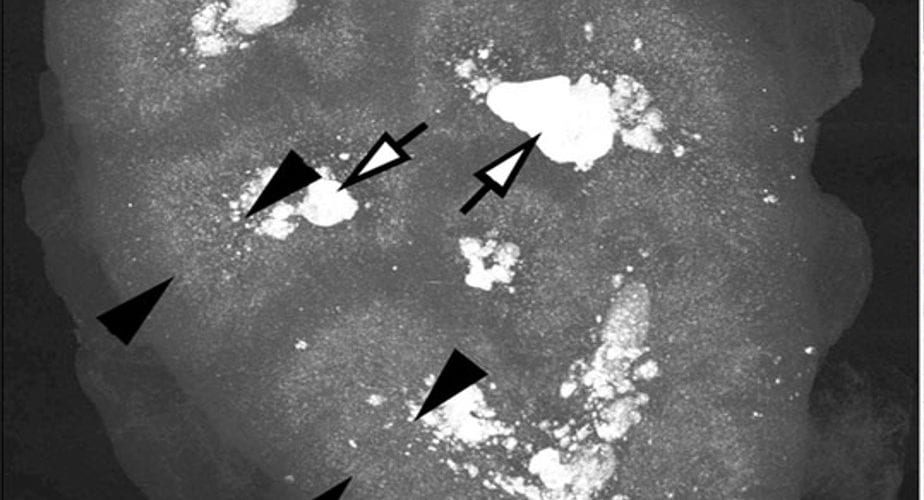
CASE 4: MEDULLARY SPONGE KIDNEY
Medullary sponge kidney (MSK) is more spoken about than witnessed, and more witnessed than accurately diagnosed. This patient adds to the 12 we have described in our publication, and adds also in having a very long and evolving history with one of us (FLC). We write...
Case 3: A Success Story
This is a first for the site, and perhaps it should have been a feature long ago. After all the generalizations and reviews there is something wonderful about a single instance that contains all the elements of a topic in the kind of instructive detail we can get only in life itself. Pat – who has permitted me to use his name and data – forms calcium stones and has idiopathic hypercalciuria and a job that makes hydration a problem. For treatment I wanted to use low sodium diet to lower his urine calcium excretion and if possible avoid thiazide diuretics just because of his job which is outside and in summertime poses serious heat loads. MIchelle, his wife, created a reliable low sodium diet for him as proven by multiple follow up tests and that reduction of sodium lowered urine sodium and stone risk, as one might expect. I asked her to share her experience in doing this, and she responded with this wonderful article. It helps that she is a professional writer! I am indebted to Michelle and Pat for their story, and I hope you like it.
CASE 2: A Calcium Oxalate Stone Former
CLINICAL FINDINGS A man in his fifties formed his first stone in the early 2000’s and his last 6 months ago. There was a single passage event a year or two after the first stone at which time he was given hydrochlorothiazide 25 mg daily. A right SWL procedure...
CASE 1: A stone Former
CASE 1: A Stone Former. As you will see, this is a person with considerable numbers of stone attacks who has certainly produced large stones in the past, but he posed major problems in deciding if stones were active and is therefore a perfect place to start. His many laboratory abnormalities are just wonderful for thinking about stone pathophysiology.