by Dr Fredric Coe | Feb 16, 2016 | For Doctors, For Patients, For Scientists
This little goodie started with my partner Dr Anna Zisman who to wanted us to have a simpler format for patients to follow in looking at their 24 hour urine lab reports. Answer five easy questions and get back a list of what you have to do with fluids and diet. Try it. Let me know if it works. If not, can you help make it better?

by Dr Fredric Coe | Feb 14, 2016 | For Doctors, For Patients, For Scientists
Well, here it is, the last pillar in the foundation. My goal is to enable patients to achieve successful stone prevention and I believe this requires a partnership with their physicians, a partnership in which they play a very active individual role. Patients after all are the ones who can manage diet, fluid intake, and life demands, only they can assure that 24 hour urine collections are representative of normal life, and, frankly, only they can decide on a life of long term prevention. Stones being rarely fatal and usually not a cause of progressive kidney disease, patients can elect prevention or not, and their physicians are in a role more like attorneys and accountants than authoritarian directors of events. But as in Eden, one can expect proper choices only if one has provided full knowledge, which I have set out to accomplish. By proper I mean most suitable to patients given full knowledge, for some may not care to exercise themselves so much as I think they must to be successful, whereas others may consider the work of prevention slight indeed compared to the consequences of continued stones. In any event, this article is the end of that cycle of enablement I can manage, and I put it here, as in all writings, as the chef puts out her best effort – to face the indifferent judgement of the gourmet.
by Michael Borofsky, M.D. | Jan 24, 2016 | For Doctors, For Patients, For Scientists
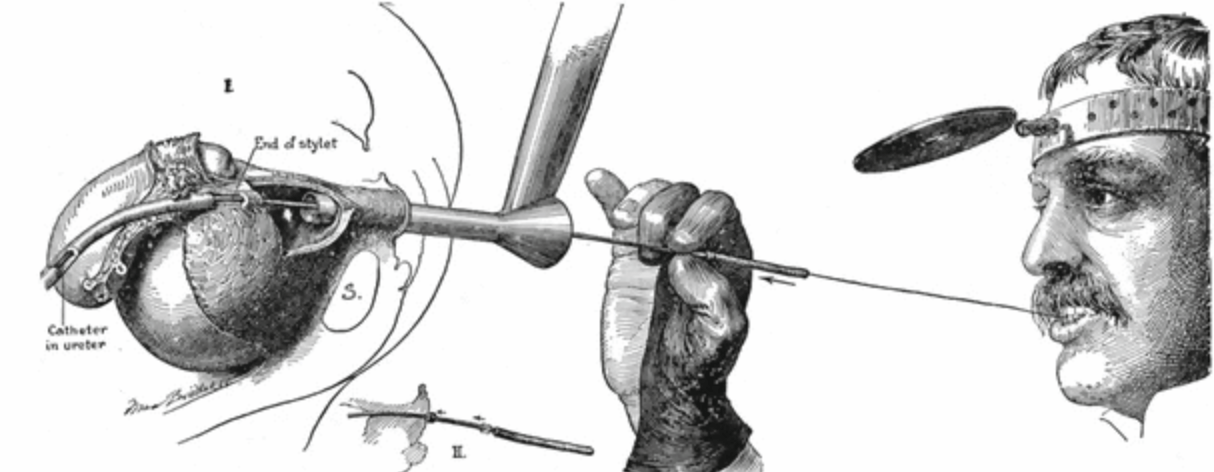
Dr. Mike Borofsky authored a favorite article on this site – Pain from Kidney Stones. Now, he has authored our first article on stone urology, meaning the urological surgeries used for treatment of stones in the kidneys and urinary tract. Ureteroscopy is fast becoming the preferred approach, outstripping shock wave lithotripsy and percutaneous lithotripsy. This is because the instruments for ureteroscopy offer superior optics and are flexible and small enough to get from the urethra up into the kidneys and into all of the crevices of the kidneys where stones form and lodge. Armed with tiny but powerful laser fibers, the new ureteroscopes permit surgeons to fracture stones in the kidneys and turn them into mostly harmless dust that passes silently for days or weeks thereafter, or into small fragments they take out during the procedure leaving not a speck behind. It is a brilliant time to be a young urologist and use these marvelous instruments to do what would otherwise require a far more complex and risky procedure (percutaneous nephrolithotomy) or depend upon an indirect and often incompletely effective one (shock wave lithotripsy).
by Dr Fredric Coe | Jan 11, 2016 | For Doctors, For Patients, For Scientists
These two articles cover the main stone types, and this new one on uric acid parallels the prior one on calcium stones. Like the calcium stone article it is meant for patients, although physicians might like some of the nuances. The purpose is not to make patients into their own physicians but to enable them to understand their own stone forming abnormalities. My ruling hypothesis is that patients want prevention, and will embrace and implement the changes needed with more enthusiasm and endurance if they fully understand the goals. LIkewise if they can themselves follow the effects of their efforts on stone risk factors they will believe that what they are doing has real meaning. I know that hypotheses are for disproving, and I know someone may well do a prospective double blind randomized trial, some day, to test mine. Right now, I believe in the idea because of Eden whose resident twosome were not just told about the tree but exactly why they should not eat of its fruit. I know it is an unfortunate comparison, given the outcome, but much effort was expended on education. My source for the details, apart from the Hebrew Bible, is Milton, J: Paradise Lost; Books V – Viii.
by Dr Fredric Coe | Jan 7, 2016 | For Doctors, For Patients, For Scientists
This site is meant to promote prevention and my current hypothesis is that enabling patients to read their own 24 hour urine tests with a professional eye will help achieve that aim. It is not an easy task. Lab reports, even the best of them, are dazzling arrays of numbers in often mysterious units. Even physicians have some work to do. But numbers are numbers and people can read them if they have the code. Here I have parsed out the main numbers for the calcium stones: Volume, calcium, oxalate, sodium, citrate and pH. Because this is the first article on reading this kind of report I also discuss collection quality, conversion of units – some labs report, as an example, calcium in mg/24 hour, others in mmol/24 hour, even mEq. So I introduce the simple conversions needed to use what I have written for a report with different units. Likewise I introduce how urine creatinine can be used to estimate collection quality. The supersaturation come at the end, as they should, being the final summary of everything. The tone is about that for trainees in nephrology or urology I have often worked with but with jargon elided and a focus on lab results per se. Those interested can follow the links into the thickets of the site which hold enough to satisfy most appetites. The main purpose is to enable patients to cast a cold eye on their own problems and on the results of treatment efforts so that in the event saturations can be effectively reduced and stone recurrence with them.
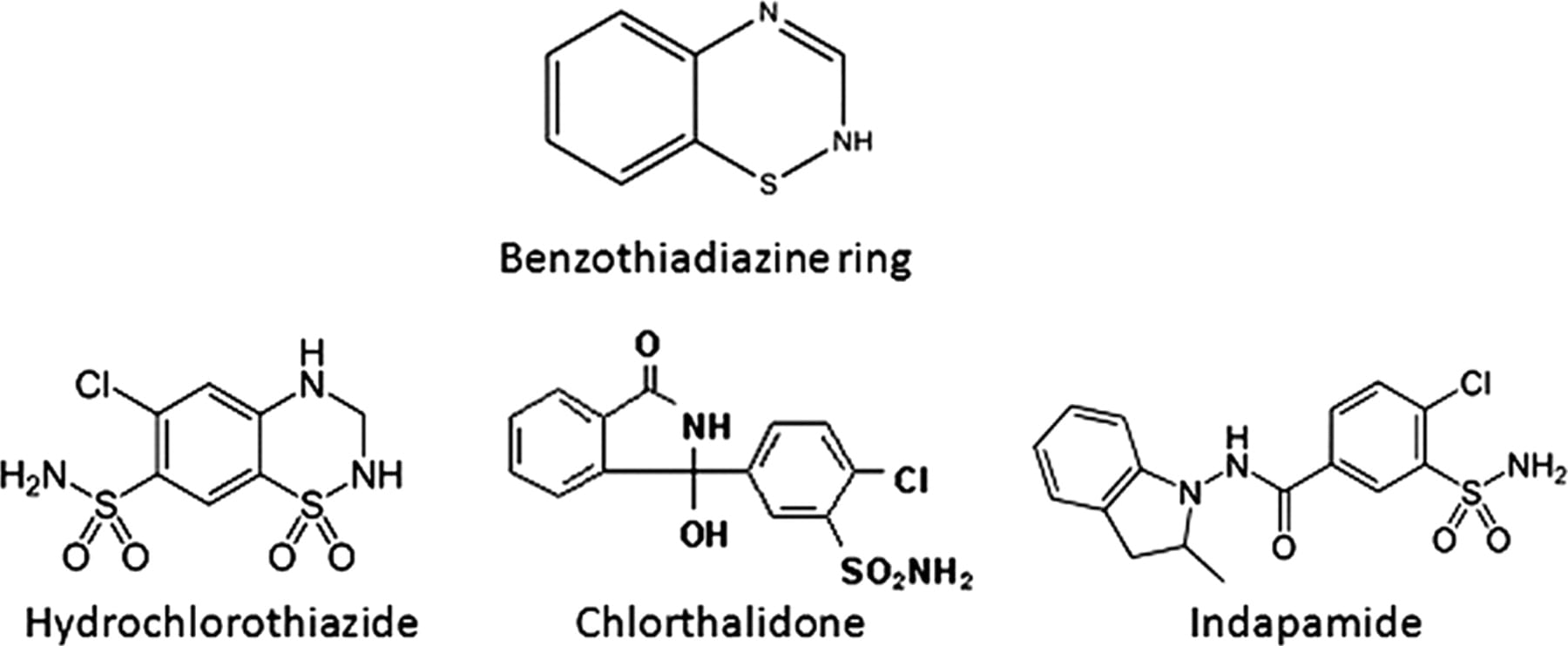
by Dr Fredric Coe | Dec 23, 2015 | For Doctors, For Patients, For Scientists
The thiazide type diuretics are able to reduce new stone formation and are an important part of stone prevention regimens. Here is all about these drugs: The trials that show they work; How they work; What they do for bone: Certain precautions in their use. To give a pill to someone is to throw a seed on unprepared ground – it is a sterile and doomed enterprise. All the features of prevention from diet and fluids and lifestyle come first, so that what one can do with them is being done. Then the drug will be most useful. And, you will know by the fall in urine supersaturation achieved. Whatever it was when stones were forming is too high, and real treatment means it has been reduced. After all that can be done without thiazide has been done, there will no doubt be residual supersaturation lowering needed, or one would not use the drug. The marginal benefit of the pill can be assessed by the extra fall in supersaturation it produces. Which supersaturations? Those related to crystals in the stones forming.
Five Steps to Stone Prevention