
It was a comment by Dr. Robert Perlman, a friend and brilliant scientist in the field of evolutionary medicine, that set me off on what I can only call a historical and scientific pilgrimage, a pilgrimage to the beginnings of the modern guidelines. At the end of my most recent article on the guidelines and our present stone fomenting diet, he pointed out that the US diet guidelines are so influential and the new ones so helpful in management of kidney stone disease we all must question who creates them, and how.
The guidelines must have, he implies, the kind of elaborate and winding history one expects from a succession of governmental committees which, howsoever well served by volunteer scientific experts, can be subverted – by money, by entrenched beliefs, by dishonesty, even, but despite, in the long run, may arrive at good and measured conclusions.
I am back with my tale.
It is a tale of earnest and honorable endeavor spiced up with scandal and outrage.
It is a cautionary tale. Along my way I stumbled over what might be the roots of the modern and horrifying obesity epidemic. I found high placed scientists on the dole from the sugar industry, convicted by the very letters that prompted their dishonest writings. I read the flawed reviews they wrote in the New England Journal of Medicine and wondered at them. I sensed unsaid pressure from the Salt Institute pushing against the guidelines as they spoke for less sodium in our food.
But against all this I could not but admire the pluck and constancy of the successive committees of volunteer expert scientists who never stopped pushing back, fighting – if I can infer such a thought on their part – for better conditions of diet in this country. And, despite all, they have done well.
The painting by Evaristo Baschenis (1617–1677) seems about right for guidelines so aimed at grains and vegetables. He was largely forgotten until the resurgence of interest in Baroque art this past century. He worked in Bergamo as a portraitist and still life artist, with particular interest in musical instruments and things of the kitchen. The link is to a Met exhibition of his works in 2001.
A Momentary Introduction
In 1977 Senator George Mcgovern began a process of US diet reform that accomplished much good. He had chaired a Senate Select Committee on Nutrition and Human Needs whose 1977 report gave rise to the first diet guidelines, in 1980.
Subsequently, the USDA was asked to create a new public report every five years. Unlike the first one, subsequent reports were each to be guided by a scientific advisory committee composed of experts who could apply such science as they had to fashioning what they thought was a good way for American people to eat. The report of the advisory committee would then be used to fashion public guidelines. So every five years we have an advisory committee report and a set of public guidelines.
I am concerned here on this site mainly with the six items that directly affect stone disease: Calcium, sodium, potassium anion, refined sugar, protein, and oxalate intakes. Of the latter, almost nothing has been said in the Diet Guidelines. The rest have been discussed in a remarkably variable way. If obesity plays a role in stone genesis, then perhaps another aspect of the guidelines also matters.
Senator George McGovern
Born in 1922 in South Dakota, he enlisted in the US Air Force and served from 1942 – 1945 flying combat missions in the European Theater. After the war he graduated from Wesleyan University and in 1953 received a PhD from Northwestern University in history and government. He was elected as a Democrat to Congress 1957 – 1961 and then elected to the Senate where he served from 1963 to 1981. He chaired a Select Committee on Unmet Basic Needs, and another on Nutrition and Human Needs – the one that began the Guidelines. He was awarded the presidential Medal of Freedom in 2000 for his work on human nutrition.
Here he is with cans of sugared drinks whose numbers reflect rising use.
In common with almost all of the scientists who gave their time to the work of the nutrition movement Senator McGovern seems in every way an admirable citizen who used up his life in service to the needs of the people who elected him to high office.
History of the Guidelines
This brisk annotated precis from the government fits well with but does not exactly match what the primary documents say. The precis presents things as moving in a stately and cohesive manner, but arguments for higher or lower recommendations abounded and actual numbers offered to the public varied in turn. Even so, more or less, things began with the report of the Senate Select Committee led by a man who cared about nutrition and knew how to move matters forward, and did indeed move forward to their present shape.
The McGovern Report – 1977
 Hoary, aged, typescript and all, take a look: The ‘DIETARY GOALS FOR THE UNITED STATES’ .
Hoary, aged, typescript and all, take a look: The ‘DIETARY GOALS FOR THE UNITED STATES’ .
The year, 1977, had two presidents in it, as you remember: Gerald Ford and Jimmy Carter. We had ended our troubles about president Richard Nixon.
The first four goals of the report were increased consumption of carbohydrates (from vegetables and fruits) in favor of lower fat and especially saturated fat and cholesterol. The fifth goal was to reduce consumption of refined sugar to 15% of total calories. Consumption of refined sugars rose from about 40 pounds/person in 1905 to over 120 pounds/person by 1975. They recommended reduction of sugared soft drinks and baked goods.
The sixth goal was to limit intake of salt to five grams per day. Given the gram weight of sodium chloride of about 58, this would be 86 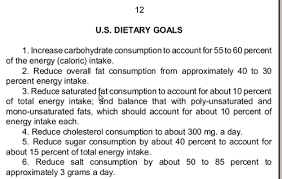 mEq/day of sodium, or 1,983 mg of sodium, slightly less than the present 2015 – 2020 tolerable upper limit.
mEq/day of sodium, or 1,983 mg of sodium, slightly less than the present 2015 – 2020 tolerable upper limit.
So of our five concerns we share with the broad world, calcium, sodium, potassium, sugar, and protein, the second and fourth were promulgated in almost their exact present form 40 years ago, and the third, potassium anion from fruits and vegetables, almost so although the critical element, potassium, is given only slight mention.
The Report came with its critics who were sceptical. In a supplemental forward, Senators Percy, Schweiker, and Zorinsky remarked that whereas the US Inter-Society Commission for Heart Disease Resources and the American Heart Association recommended, as an example, reduction of dietary cholesterol to below 300 mg, Canadian, and UK agencies were not convinced. These senators were concerned that a low fat diet juggernaut was beginning to roll, and caution was in order.
The Sugar Scandals
Perhaps they were right.
The lipid movement was never so firmly based as its supporters believed, and the resulting high carbohydrate low fat diet is widely thought a contributor to the massive contemporary rise in obesity. Of the four scientists who advised the Committee, Drs. Mark Hegsted, Philip Lee, Sheldon Margen, and Beverly Winikoff, one – Hegsted – disgraced himself by taking money from the Sugar Association. His boss, Dr. Fredrick J. Stare, the chairman of Harvard’s nutrition department, also took money from them.
The sugar scandals, the deceit, the base behavior of major academic figures is not for me to describe; here is a link to the NY TImes whose reporter can claim a power of historical narrative. The NYT article arises from this article in JAMA. Hegsted, under Stare’s supervision, perhaps, wrote at the behest of the Sugar Association, for pay, a review of the evidence concerning heart disease and nutrition, a review biased to favor the idea that sugar was harmless and fats malign. He was asked to discredit the work of a better scientist than he was, and did so. The New England Journal of Medicine published the article, and although financial bias was not then the issue it is now, one wonders at the reviewers and the Editor in Chief (Dr Joseph Garland was Editor in Chief until 1967 and thence responsible) that they could not detect its flaws. The NYT article points to another scandal concerning recent payments by Coca Cola to researchers who play down the dangers of sugared drinks.
Very recently the New York TImes has reported a nearly exact parallel. Scientists in the pay of the sugar industry published an analysis of the food guidelines concerning sugar and found the scientific studies that support the guidelines of poor quality. Just as the NEJM editor did 40 years ago, the editor of the journal – Annals of Internal Medicine, Dr. Christine Laine let the review stand despite obvious funding from the sugar industry. I find it difficult to sort out the problems with the review. Bias by paid authors is very possible; experts on nutrition – as I have said I am not one – violently disagree with the publication. On the other hand, this is the same journal that brought us what must be the most flawed and basically silly analysis ever written concerning evaluation and treatment of kidney stones – a field where I am an expert.
The systematic review, which is part of the ‘evidence based medicine’ school of thought is easily biased because readers can set up criteria for ‘quality’ and then use those criteria to choose or discredit papers. The application of criteria are invariably unbiased but the criteria are never fully objective even though often presented as such.
Special irony abounds here because the guideline committees are themselves advised by practitioners of the very same systematic review techniques as were used in this apparently flawed article. So we are treated to the spectacle of ‘unbiased’ systematic reviewers who completely disagree with one another.
Dr Laine surely must have known this disagreement as unexpected. Even if she were willing to publish writers paid by the sugar industry to review a matter essential to that industry, the conflict between two groups of experts using the same approach should have raised concerns. What did the reviewers think? Surely, being nutrition experts, they would recognize the conflicts immediately. The NEJM in the past and now the Annals seem easy prey.
The Surgeon General Report – 1979
Controversy and pushback the report engendered led to a second report whose findings were partly presented in the 1979 Report by the Surgeon General of the US. The Surgeon General Report covered smoking, alcohol, and many other aspects of US health, and among those diet changes such as ‘moderate dietary changes to reduce intake of excess calories, fat, salt and sugar;’. The document is humane, comprehensive, and within its time rather wonderful, but in treating of high blood pressure scarcely mentions the role of diet sodium: ‘Excessive salt in the diet and stress are factors not yet completely understood; they may contribute to the development in some cases of what is called “essential” hypertension in the 90 percent of patients in whom the disease is present without any known organic cause.’ Not exactly a ringing concern over what has come to be understood as a structural mechanism for high blood pressure!
I pause here and contemplate what was the main focus, lipids, for this was the beginnings of the ‘Heart Healthy’ diet. On page 11 of the document the authors note that we had increased our fat and reduced our carbohydrate consumption over the decades, this latter meaning use of starchy foods. Also, refined sugars had replaced starch with the result that the starch vegetables were on the wane in exchange for more fat and sugar. Populations that used more starch and less meat and fats suffered less from heart disease, and links were already made between blood lipids and heart disease, so a natural answer was to change our diet away from fats and refined sugar to more starchy foods.
If you want a sense of antique medicine, read the whole section, for it is here we move among the pillars and foundation works of the heart healthy movement that gradually took over and, some say, fomented the present obesity problems, others say saved us from the menace of coronary artery thrombosis.
The 1980 Guidelines
The report is a mere thing but began the era of ‘heart healthy’ high carbohydrate diets. There was no Scientific Advisory Committee for this first set of Guidelines but four experts provided assistance. I have already named them: Drs. Mark Hegsted – who defiled himself by shilling for the Sugar Association, Philip Lee, Sheldon Margen, and Beverly Winikoff.
 We should eat a variety of foods, it says, because we have a better chance of avoiding deficiencies. Calcium comes up in recommendations about milk but excesses are scorned and no one says how much milk. We now know it is 3 cups a day, and I think they knew then, or perhaps not. Fruits and vegetables are emphasized, as we would today but now we do it because of not only a general regard for their virtues but the potassium anion that is so important for blood pressure and, incidentally, for stone prevention.
We should eat a variety of foods, it says, because we have a better chance of avoiding deficiencies. Calcium comes up in recommendations about milk but excesses are scorned and no one says how much milk. We now know it is 3 cups a day, and I think they knew then, or perhaps not. Fruits and vegetables are emphasized, as we would today but now we do it because of not only a general regard for their virtues but the potassium anion that is so important for blood pressure and, incidentally, for stone prevention.
Part two is about maintaining a proper weight, and since this will always be present I will not review the matter again.
Parts 3 and 4 concern the switch to high starch diets and reduction of fats.
The idea was that ounce for ounce carbohydrates have less calories than fat, a true proposition, so it is easier to control weight eating them – beans, peas, nuts, seeds, whole grain breads, cereals and the like. As for meats, lean cuts, trim fats, reduce amounts; reduce eggs, cream, butter.
Reduced refined sugar is part five, and forceful – it has a modern ring. But, the major health hazard was tooth decay. Sugar was said to not be a factor in diabetes, nor will it promote vascular disease. It is a clean fuel, but not ideal because devoid of other nutrients and a source of empty calories. Overweight is mentioned as if separate from refined sugars, and we know that professor Hegsted was on the committee. Most important, the number in the 1977 report – less than 15% of total daily energy intake – is deleted.
Sodium reduction is also handled gingerly. It is recommended for those with high blood pressure. But the powerful demand of the source document that calls for below 1,900 mg of sodium is gone.
A five year rhythm of reports was codified into law.
The 1985 Guidelines
The lessons preached in 1980 are preached again almost unchanged, so there is little to say. Diet calcium is mentioned in relation to osteoporosis, but no goals are given. Sodium and refined sugar remain suspect but no goals there either. Because the wording is often unchanged one gets the sense that little of major importance has transpired.
This report was guided by a scientific advisory committee. The Scientific Dietary Guidelines Advisory Committee report is also slight with few references. It is notably terse and offers little serious analysis of scientific papers of the time. Perhaps, being the first such committee, the style and size was yet to evolve.
The 1990 Guidelines
 The Scientific Advisory Report is much larger and more analytic than in 1985.
The Scientific Advisory Report is much larger and more analytic than in 1985.
Although said to be in accord with the past these guidelines have subtle enhancements. Throughout there are references to bone disease and a need for more calcium. Osteoporosis is mentioned more explicitly, for example in overly thin people. The lipid and diet cholesterol content issues remain, and meats are singled out as sources of both, thence the persistent demand to reduce meat intake. Eggs remain suspect and using egg whites – a practice I personally find abominable on strictly culinary grounds – seems more prominent.
But milk servings – 2 or 3 a day are now highlighted, meaning that calcium intake now has an almost modern quantitative feel. Three cups of milk provide about 1,000 mg of calcium.
Use of fruits and vegetables remains as it was, as does the substitution of breads, cereals, pastas, rice, peas and beans for meats and fats.
Reduction of refined sugar is mentioned but the goal of below 10% of total calories is suppressed. The committee points out a few details that are interesting in view of what we know. ‘Avoid’ is replaced by ‘Use…in moderation’ in relation to sugar and salt, as an example. One can feel the pressure from the sugar industry and salt lobby pushing against what might reduce sales of sugared drinks or salted snacks.
An Intermission: Food Labeling
Within the massive list of US food policy changes, food labels are only one entry, but an entry of great importance.
After some political wrangling, THE NUTRITION LABELING AND EDUCATION ACT OF 1990 became law and led to the common labels we have now. This stately and academic reference covers the period from 438 AD to now, and includes references about the law. Here is a summary of the law. The US president at the time was George Bush senior, and the sponsor of the bill was Henry Waxman. The New York Times did a nice summary of what happened in the ensuing few years of wrangling before the new labels became a reality in stores.
Between the 1990 guidelines and the 1995 guidelines fell the shadow of food labels and those labels were controlled more by the FDA than the USDA which may possibly be more sensitive to the food industry.
A key element of the labels is correspondence with recommended daily allowances (RDA) for key nutrients. The current RDA values are here. Dietary reference intakes (DRIs) are very similar, and here are the tables for both the DRI and the tolerable upper limits. Both tables arise from the Food and Nutrition Board, Institute of Medicine, National Academies and in a later section I will tell you about the old RDAs and the new DRIs.
The Obesity Epidemic
 In the late 1980’s rising obesity first became apparent. This long and well referenced review gives a reasonable background on the topic. The nuanced and thoughtful author hesitates to ascribe obesity or its consequences to any one factor but, to many, the high carbohydrate diet first promulgated in the 1980 guidelines was a major cause. Here is a readable review from The guardian, sans references.
In the late 1980’s rising obesity first became apparent. This long and well referenced review gives a reasonable background on the topic. The nuanced and thoughtful author hesitates to ascribe obesity or its consequences to any one factor but, to many, the high carbohydrate diet first promulgated in the 1980 guidelines was a major cause. Here is a readable review from The guardian, sans references.
A not too recent review in the American Journal of Clinical Nutrition summarizes the carbohydrate obesity model in terms of excessive fructose (table sugar, or sucrose, is 1/2 glucose and 1/2 fructose). Fructose converts to fat as it is metabolized in the liver, and raises uric acid production; uric acid may directly cause vascular disease. A recent review of this complex topic seems supportive of the idea that fructose is a villain and is sharply critical of sugar industry funded studies that show the opposite it true. Finally, a well known journalist has done a wonderful review of the low fat obesity problem. To me industry bias seems certain, and like the tobacco industry aimed at delay of regulations. But I am not an historian of political history and leave off here.
The 1995 Guidelines
These guidelines inaugurated the now infamous USDA food pyramid whose base of grains and pasta, some say, fed the obesity epidemic .
.
They also promote calcium intake, especially for women and children.
Food labeling had become a reality and listed sodium upper limits at 2,400 mg/d, so the guideline quotes this figure which is far above what was called for in 1977.
Also, potassium is first mentioned by name and attached as a virtue of fruits and vegetables.
Vexed and political, sugar is handled with tongs. One must make clear – the guidelines say – that starches and table sugar are the same when metabolized, that table sugar and sugared drinks do not cause diabetes and that sugar is just another nutrient.
For sodium we have niceties of diction perhaps to comfort the Salt Institute: ‘A key objective… is to shift the tenor of this guideline toward dietary advice and away from primary focus on hypertension.’ But apart from bone mineral loss and worsening of stone risk from hypercalciuria, why would anyone care about sodium if not for hypertension. Hypertension is scary, so – I imaging the Salt Institute speaking – keep it from being too prominent. Nevertheless food labels were immutable, and with them the 2,400 mg sodium level.
It is interesting to compare this version with the source document from 1977 when less than 2,000 mg of sodium and less than 10% of calories from refined sugar were already recommended. Pushback was powerful.
So, what we have in 1995 is more about calcium and potassium sans numbers, but less stringency about sodium and sugar. But the labels were in place.
The 2000 Guidelines
One might call this the peak of the pyramid. Active men and women were to have 11 and 9 servings of rice, cereal, pasta daily, a huge carbohydrate load. The same two groups were to have 4 and 3 servings of fruits – reasonable indeed – it is what would give the needed potassium. Of beans, eggs, nuts, fish meat and poultry 7 and 6 ounces daily, and of milk and other dairy products – fat free if possible – 2 – 3 servings, this latter scanty to enough by modern standards.
Because of food labels, sodium was set at 2,400 mg upper amount. Calcium was not specified in units but on the labels as percent of daily needs, and no actual goal was set.
So, of our modern needs for stone formers we have sodium above where it was in 1977, calcium unspecified but moving upward, potassium at near modern levels, refined sugars not well specified, and protein at a low end. We were to eat a plant based diet and all would be well.
Sugar has, however, become a bit of a target. People were advised to avoid sweetened drinks. Salt and blood pressure were perhaps more linked and advice to moderate it more direct. For the first time the effect of sodium to raise urine calcium and deplete bone mineral is called out in a box and emphasized.
I find interesting the great emphasis on obesity which had become evident a decade before. The hope – that more vegetables and starches and less fat would work seems fey and strange, looking back. A great emphasis on exercise begins here, likewise in hope to correct the problem.
If you look at page 34 of the document (labeled as page 34 in the text because of front materials) you will see what I might call the new awakening. Low fat high carbohydrate diets are beginning to look dangerous because of diabetes and vascular disease. The writers are aware that too low a fat diet has the potential to create obesity. One wants ample fat but unsaturated. Diet cholesterol per se is no longer a concern.
Ars Nova 1997-2004
You might have wondered by now where all these numerical recommendations come from. The advisory committees are the efficient or immediate source, but numbers imply some science has been used and I have not yet mentioned where that science comes from.
The first attempts to quantify nutrients at a large scale government level were recommended daily allowances (RDAs) first provided in 1941 in service of nutrition of soldiers in World War 2. The RDA for any given nutrient is sufficient for 97 percent of the population. From the beginning the RDA estimates were set by committees of the National Academy of Science, and promulgated both as medical and public information and for guidance of US and nutrition standards. They were used in their original form right through the 2000 Guidelines. The Advisory Committees that guided the Guideline process relied on RDA values in all of their deliberations.
DRIs
In 1994 influential scientists came to believe that the RDA conceptual framework could not properly express all that modern science might have to offer and the US and Canadian governments jointly supported a new movement run by the Institute of Medicine (IOM) to develop a new suite of values called DRIs, or Dietary Reference Intake Components. The IOM is a branch of the National Academy of Science and had been hosting Guideline Advisory Committee meetings as
a continuation of its long history of providing scientific guidance for nutrition, but the new venture took things – as desired – into new kinds of nomenclature and possibly new numerical standards for nutrition.
DRIs contain Ears, RDAs, AIs and TOLs. The EAR, estimated average requirement, marks the level of a nutrient at which 50% of a population would be low. The 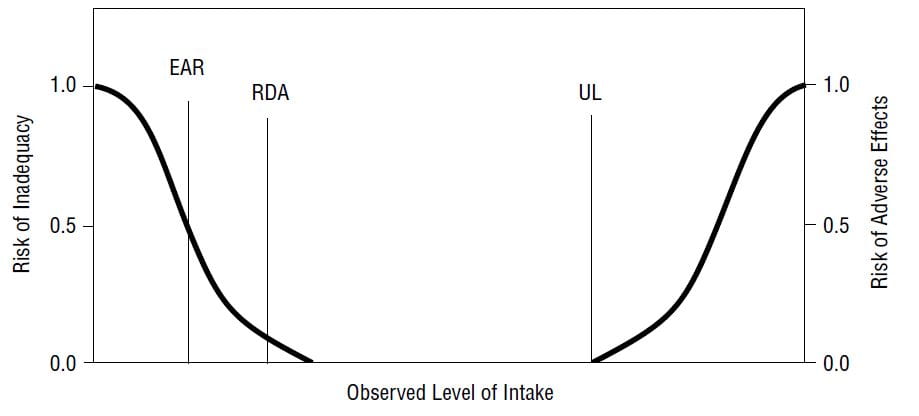 RDA remains, as it was, the average nutrient intake that is sufficient for the needs of 97% of a population. Adequate Intake (AI) is an observed or experimentally determined estimate of intake for healthy people assumed to be adequate for populations when an RDA cannot be determined. Tolerable Upper Limit (TOL, shown as UL on the graph) is the highest intake likely to pose no risk to almost all of a population.
RDA remains, as it was, the average nutrient intake that is sufficient for the needs of 97% of a population. Adequate Intake (AI) is an observed or experimentally determined estimate of intake for healthy people assumed to be adequate for populations when an RDA cannot be determined. Tolerable Upper Limit (TOL, shown as UL on the graph) is the highest intake likely to pose no risk to almost all of a population.
AMDRs
For fats, carbohydrates, and proteins which can substitute for each other to provide energy, EARS and the like are not ideal. One source of energy can substitute for another, so no one source can be a cause of inadequacy.
But any one nutrient can, in excess, increase risk of chronic diseases like heart disease or obesity. So the group defined Acceptable Macronutrient Distribution Ranges (AMDRs), the ranges of intake for each energy source below the point where it is associated with increased risk. Given endpoints like blood lipids or epidemiological correlations this can lead to the idea of low fat high carbohydrate diet, as an example.
It is easy to see how AMDRs can be obtained. One can study epidemiological correlations between use of each energy source and, as an example, heart disease, as was found for high fat intake – by some. If found, such correlation can give rise to experimental work in animals and the search for proxy biomarkers like serum lipids taken as risk factors for heart disease. Once such risk factors can be found correlated with heart disease, one can attempt to show that their reduction also reduced heart disease, as was found for statins. Thereupon one has an AMDR for fats and one can draw the shape of the food pyramid.
The dangers of the process are all too well known.
I will not reference my remarks, but some of us remember how gastric acid was, for ages, the obvious ’cause’ of peptic ulcer.
Erosive and nasty, how else could ulcers arise but from acid injury. People with extremes of acid production due to inherited disease had severe ulcers. When drugs came on the market to reduce acid production they healed ulcers. Perfect, and perfectly wrong.
No one imagined bacteria were the ’cause’ of gastric ulcers, because bacteria as a cause of gastric ulcers were what I might call radically unknown – radically unknown because unthinkable, unimaginable, hidden beyond reach of our imaginations from which issue the only true progress of science. The scientists who found the true cause were by their own description not very skilled in high science but they were imaginative and therefore able to see the truth.
The AMDR process has an inherent capacity to mislead because correlations can drive actions that imagination cannot control. It has a capacity to move forward without causal hypotheses that demand deduction of experimental tests that can disprove them. This is not intrinsic to the AMDR but rather results from the attractiveness of the imagery and metaphorical content behind the idea of a nutrient as causal of chronic disease. If one is to have reliable science, such an idea must ultimately arise within a hypothesis that leads to deduction of necessary experimental results without which the idea is falsified. But diet is a large scale matter, experiments are expensive, and proper science easily bypassed.
But how about EARs? How do they add to the RDA?
EARs AIs and TOLs
EARs, actually medians, not averages, work well for vitamins and minerals that have specific effects, toxicities and requirements.
As an example, vitamin A requirements need to be sufficient to permit adequate hepatic stores of the vitamin. In animals it is possible to determine dose response of vitamin and hepatic stores, and these can give some clues to humans. Serum vitamin A levels themselves do not measure hepatic stones well. Isotope dilution has been shown effective, and is an example of how human EARs could be obtained. This is a mere and rather old example, not meant to describe what is actually done now by vitamin A experts but rather to illustrate how they can work. Given an EAR one can calculate the RDA as the EAR + 2 standard deviations of the EAR distribution.
For calcium, bone balance studies performed for a century can define a range of intakes over which balance goes from negative to positive in men and women of various ages, and in children. In fact balance is a main technique used in setting needs. But EARs inherently require some form of dose response curve between two real number distributions – dose and effect. Without it and without the reasonable assumption of the normal distribution, it is not possible to extract the parameters of the normal function that give rise to medians and estimates of variance. No biochemical assay exists to permit generation of a dose response curve for calcium, so therefore AIs are used. TOLs come from epidemiological data relating calcium supplements to kidney stones, as an example.
What is Different from when RDAs Were Used?
Lets be clear, calcium requirements as early as 1977 were a lot like those presently proposed and balance data are ancient and as interpretable long ago as now. So in many instances I am not impressed that the DRIs have made a big difference. That may be naivete but I can read.
A big change is in methods and not so easy to spot unless you read into the technical sections of the reports. Whereas, for example, balance data, population data on bone mineral density vs. diet calcium, and effects of diet calcium on fractures all arise from only one source – peer reviewed scientific papers, and whereas prior advisory panel members could be given the papers to review and in fact were often not only expert readers of such papers but not rarely their authors, the new approach is based on meta analysis.
That is perhaps the big change.
Meta analysis has two parts. The first is a scrupulous harvest of usable papers, usable meaning good quality, good quality meaning well done, well controlled, suitable to the needs of the work and such. The second is an attempt to pool data from the studies to get a kind of average effect – for example I have myself pooled hundreds of balance studies – alas never published – to estimate calcium needs in stone formers.
This kind of work is expensive and someone has to pay for it. In general it is too hard for individual investigators otherwise employed to do formal paper screening and data pooling unless that is their professional niche. It is too time consuming for one to expect it from volunteer members of advisory committees. I found in commentary about the DRI movement notes about how advisory committee members serve as volunteers but the analysts are all paid. How else to do it?
So the DRI movement requires and consumes more money than did the older approaches, just as one would expect from the irreducible dependency of information handling on energy – money as the price of human energy.
Another change is what I might call a higher mathematical sensibility about statistical inference that arises from use of meta analysis.
People who do such work and those who use it tend to an architectural use of statistical inference, meaning they attempt through statistical inference to construct new and better approaches to patient care and in this case to – one might say – population care. They are, if not always mathematicians themselves, committed to the colder, less passional side of medicine and science, a side given to analysis more than to discovery.
In fact, I would not call their main work analysis at all but rather its opposite, for central to its architectural intent is the synthesis of data from many sources into a reliable material for the building of a conceptual framework strong enough to support action.
It is also not science, because scientists measure things and infer their causes. This breed of intellectual manipulates what others have measured, so are engaged in a form of synthesis from published work. To me that is scholarship.
It requires a new kind of intellectual, a different type of person than is usual in medicine and science, a colder and more distant person: colder because the harvester not the provider of data; distant because in touch with the results of work by others not with the baffling, indifferent, shape changing and career destroying madness of the world as it is, the world of our objective senses, whose complexity we try to understand by imagining causes we can never directly observe.
Astoundingly, from our point of view, not a lot changed in that restricting sodium and sugar, and being liberal with calcium were present in the McGovern Report.
But the reports from here on have more quantitative finish, panache, confidence, literacy. As I said, this costs money and requires one hire the quants who can do the finishing work.
The 2005 Guidelines
This is the first of what I might call scientifically driven reports. The dietary guidelines committee report is far larger than in the past and the guidelines are no longer proposed for the public so much as for experts in medicine, nutrition and public policy. The writers make clear that research data play a larger role and the presentation itself is different being filled with tables.
Things are quantitative. Present consumption is plotted in terms of what more or less is needed to meet goals. Goals are from EARs and AIs and AMDRs.
The DASH diet – essentially a protein moderate plant based diet with low sodium alternatives had been developed and shown to benefit systolic blood pressure, and its pattern became part of the template for the recommendations.
For the first time we have our essentials in quantitative form: calcium 1,300 mg; potassium 4,700 mg (about 100 mEq); and sodium ideally below 1,500 mg but practically still below 2,400 mg; protein was shown at 91 gm for men.
One might say with this report we are more or less where we are now, and where we need to be in respect to kidney stone prevention.
The 2010 Guidelines
 This report distinguishes itself from its predecessor by being the first to address an American public of whom the majority are overweight or obese. It is more or less is the 2015 report in substance.
This report distinguishes itself from its predecessor by being the first to address an American public of whom the majority are overweight or obese. It is more or less is the 2015 report in substance.
The guidelines advisory committee report is the first to have a bright colored front page.
Milk is now at 3 cups daily or 1,200 mg; sodium remains at <2,400 mg, potassium is 4,500 mg from fruits and vegetables, refined sugars are not favored, and protein is about 0.8 gm/kg/day.
Of greatest interest to me is the corpus of appendices now offered. They contain fascinating results of the national nutritional and health surveys (NHANES) and summarize innumerable studies both observational and trial. In essence the program has become scientific.
Perhaps one should credit EARs and AIs for the final result but I am sceptical. Sodium and calcium are much like they were ages ago, refined sugar as well. And I worry about the arm’s length distance of meta analysis from reality – a form of science that does research on what others have observed. In the long run, scientists must cope with the world, not with the residue of prior experimentalists and observers.
To me the process has fallen into the hands of capable and well intentioned scholars who have a kind of worrisome rhetoric. It is as though none but they and no method but their own can discern the truth within the mass of experiments that working scientists produce. Certainly those expert in such science, all experts, in fact, are suspect of bias.
We will see if this is true, as time wears on. After all, historians make much the same claim: That they can understand what was unclear to Caesar, to Alexander, to the Pharaohs, even.
Perhaps that is the truth.
The Fat Story
A consequence of Big Sugar’s meddling in science, the low fat diet remains. It has driven several generations to eat ‘heart healthy’ as if medicine knew what that was. Recently, and from another direction, the low fat story began to unravel. Here is a link from an excellent reporter about unpublished results from major trials showing that low saturated fat lowers cholesterol and lifespan. Like many medical myths this one has achieved near religious status and may be wrong. I will add more references about the unpublished studies. Ancel Keys – amazingly – was part of the one this reporter speaks about. Remember him? He took money from Big Sugar.
Where We Are At
I have no desire to review again the 2015 guidelines. I already devoted several articles to them. In the ramshackle influence ridden way of massive government projects the successive waves of advisory committees and guideline writers eventually came to the present recommendations that work wonderfully for me as a kidney stone physician and scientist. As for fats in the diet I can have no personal scientific view but plenty of scepticism in view of the history of what happened and clear evidence of industry meddling.
I do not think the high calcium, low sodium, low refined sugar recommendations will change much, nor the total protein recommendations nor yet the high fruit and vegetable recommendations, so as far as stone patients are concerned the present diet as recommended is ideal. As for oxalate, we are on our own as the molecule has not risen to national attention, and never will. High calcium intake with larger meals much reduces oxalate absorption.
I do believe diet cholesterol content has perished as an issue and with time low fat diets will go away as a means of increasing health. But obesity is our problem because it is a risk factor in stone disease. Here I would propound my own theories for reducing US obesity but I should not. It is a matter for others, and I dearly hope they get to it and offer real solutions.
As I said at the beginning, my friend Dr Robert Perlman, whose own work concerns evolutionary medicine, made a pointed remark about my article on the 2015 – 2020 guidelines and how we deviate from them in a stone causing way. His remark concerns limitations and foibles of the process and also the unfortunate intrusions of industry not always directed to the common good. Because of his remark I set out to understand the process, and this is what I have to offer back.
Fascinating- thanks for taking the time to share this history.
Thank you for the insightful article. I think I will read it again.
Thank you for the interesting and informative article.
Thank you for sharing your findings and thoughts.
Too bad more people won’t take the time to read this! Thank you.
Hi, You are right, too bad more people do not read the US diet guidelines. They are excellent. Fred