
OUR DIET PROMOTES STONES AND BONE DISEASE
I have summarized the scientific evidence that low intakes of diet calcium and potassium and high intakes of refined sugar and sodium and protein raise risk of stones and loss of bone mineral. I have pointed out that the recommended US diet specifically seeks to...
THE LOW FLOWS
Given that kidneys supersaturate the urine by conserving water, no treatment can be more immediate and direct than to drink more water than one needs so the kidneys can excrete it and in the process dilute the urine salts – which is to lower supersaturation. Alas, there are many patients who cannot or will not drink enough water, and it is these Joan Parks writes about in this article. Over our 40 years of collaboration very many patients with the problem of persistent low flow have come through our stone program at UC, but Joan and I never wrote a paper about them so much of what we found is buried in their charts. By way of redress, Joan has conjured up a lot of details that we think people will find valuable, even though they have not been shaped into the formal character of a scientific paper.
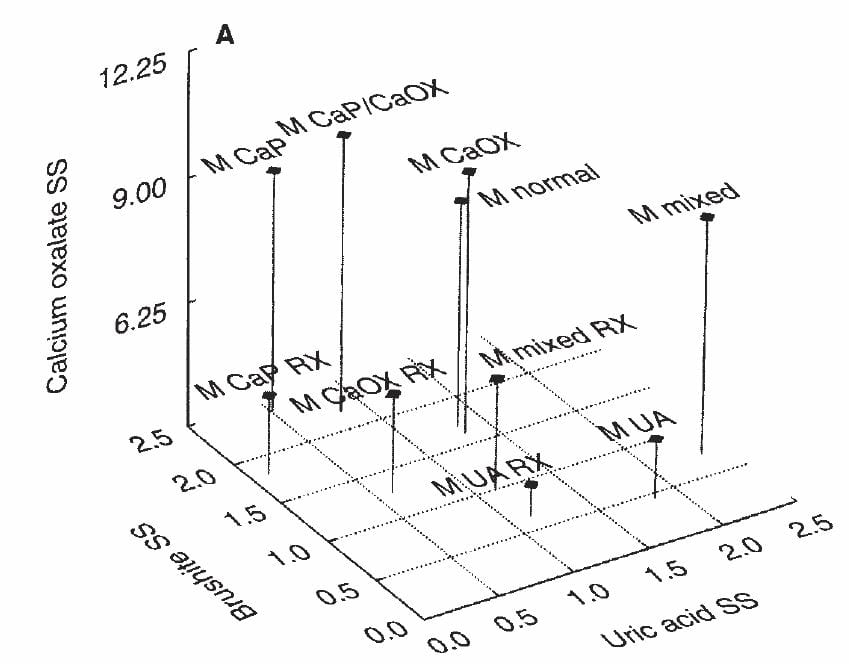
CLINICAL SUPERSATURATION
This is the essential basis for modern kidney stone prevention. I review its limitations, and how much information it provides on the pattern of stone risk factors for a given patient. Also, I show how much variation within a day hides in the 24 hour averaging and what you should do about it, and point out why you need at least two 24 hour urines before treatment. If you have signed up for my emails, read the one for this article because it explains how it is put together and best read.

CITRATE TO PREVENT CALCIUM AND URIC ACID STONES
Potassium citrate, thiazide diuretic agents, and allopurinol are the three medications that have a proven ability to reduce kidney stone formation.
Because fluids are so valuable and safe, we have emphasized their use as a basic treatment for all forms of stone disease. Here, I present the evidence that potassium citrate adds protection. The evidence is in the form of 5 trials that appear well done.
Some of the background for this article was already prevented in our discussion of the costs of this drug. Likewise, that discussion presented alternative sources of alkali that should more or less mimic the protective effects of the drug despite lack of direct trial data. I say this because the drug is a simple alkaline salt.
The article is written for anyone. Physicians will fill in more blanks than patients, but patients can easily analyse the numbers.