
 Up to this point we have considered only increase of urine volume as a means of stone prevention. The effect of increased urine volume is to reduce urine supersaturation with respect to stone forming salts and therefore reduce the risk of crystal formation which is the basis for kidney stones.
Up to this point we have considered only increase of urine volume as a means of stone prevention. The effect of increased urine volume is to reduce urine supersaturation with respect to stone forming salts and therefore reduce the risk of crystal formation which is the basis for kidney stones.
WHY CITRATE
Mechanisms
Supersaturation with respect to the calcium stones depends upon urine concentrations of calcium, oxalate, phosphate, and citrate, and, in the case of calcium phosphate stones, or uric acid stones, urine pH. Giving citrate salts can reduce urine calcium excretion and increase urine citrate. Urine citrate binds urine calcium in a soluble citrate complex, which reduced calcium salt supersaturations. Citrate inhibits crystal formation, growth and aggregation. The alkaline citrate salts can raise urine pH.
 Epidemiology
Epidemiology
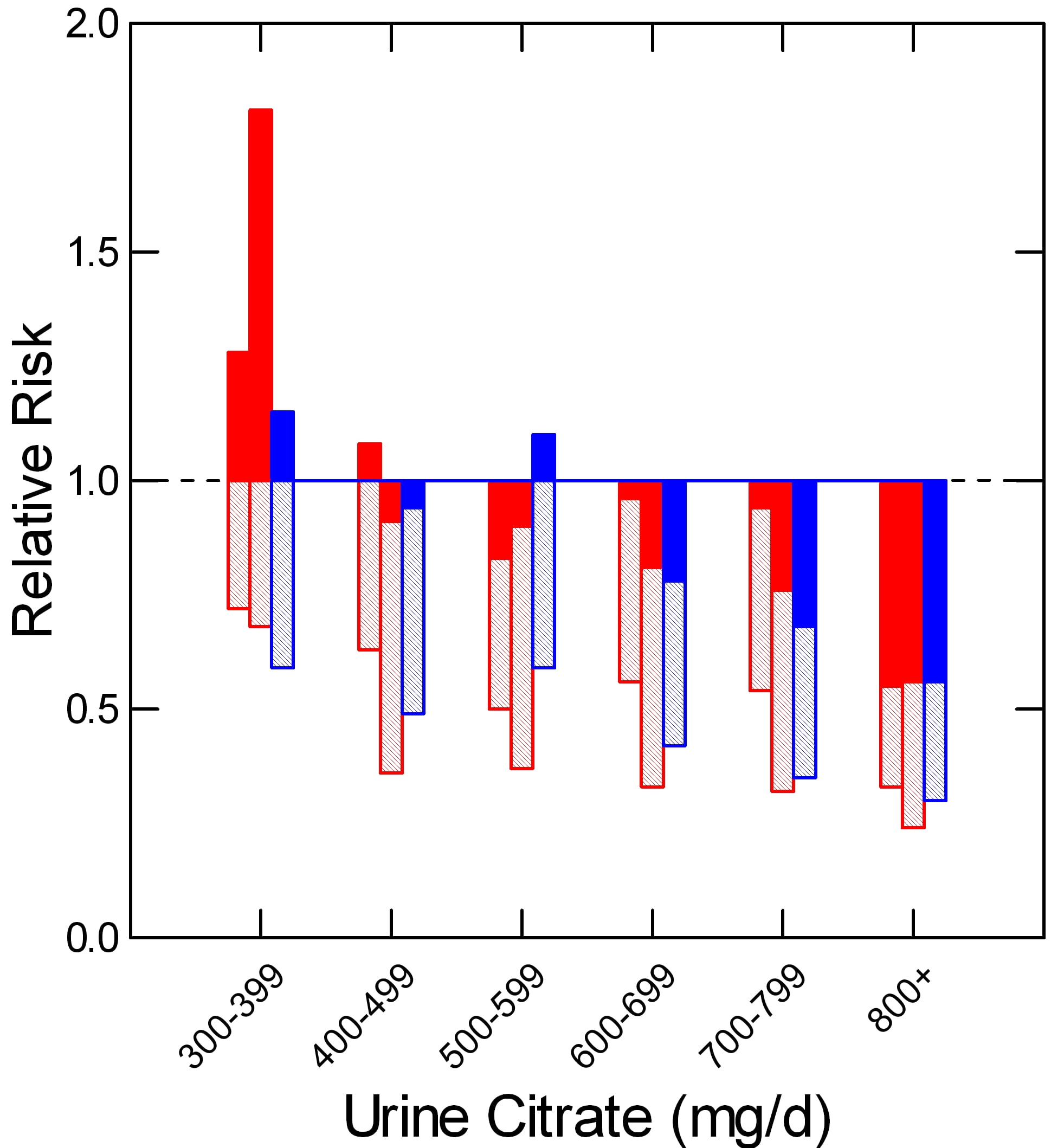
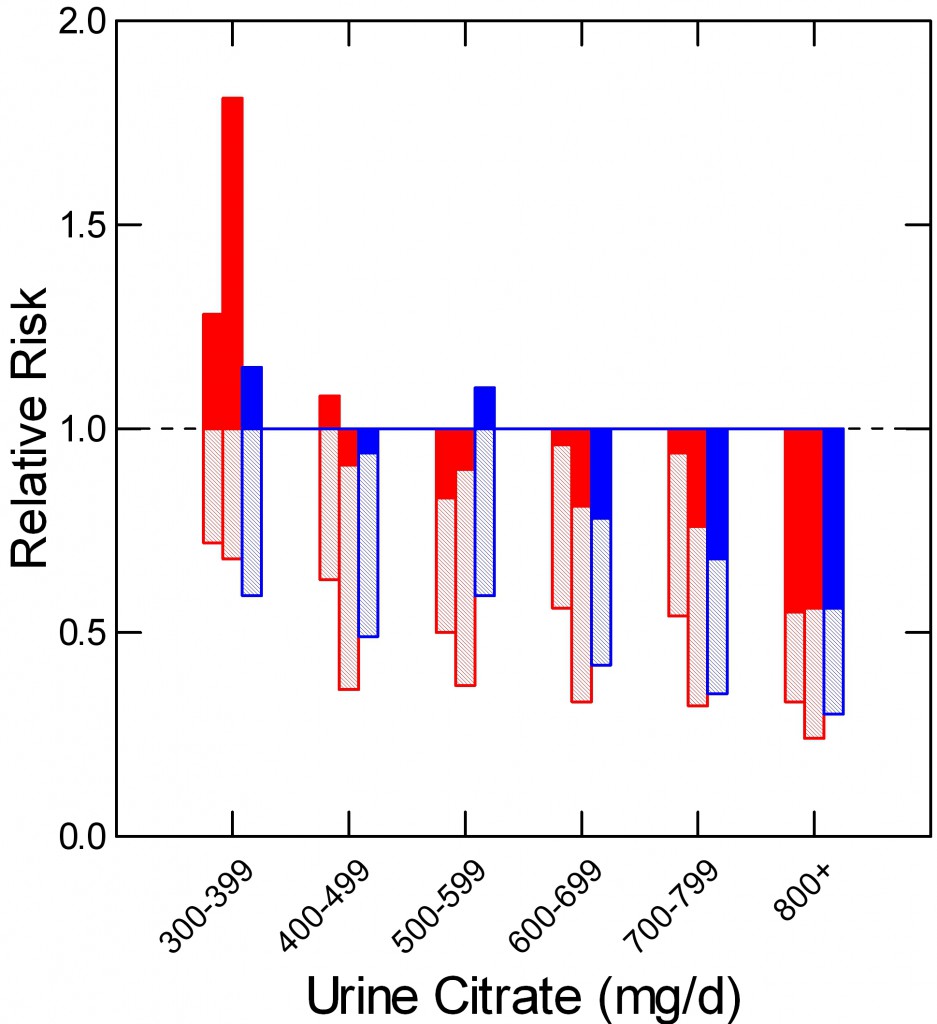
In a prospective study of two nurse (red) and one male physician cohort (blue) Curhan found that relative risk of kidney stone onset (vertical axis) rose as urine citrate excretion (shown in hexiles along the horizontal axis) fell. Below 400 mg/day of urine citrate risk was – compared to above 800 mg/day) increased by nearly 2 fold. Mean relative risk is at the ends of the shaded bars. The upper 95% of risk is at the tops of the filled bars. Even though the average risk (end of crosshatched bars) remained below 1.
CALCIUM STONES
TRIALS
Although I had quibbles with some of the comments it included, I believe the recent American College of Physicians (ACP) review of kidney stone prevention trials was done properly, and therefore have selected for review here those they felt were technically adequate.
Below is a detailed presentation of the five studies. Here is a link to my spreadsheet with all of the numbers. It also contains my references for thiazide treatment.
Ettinger et al (J Urol 158:2069-2073, 1997).
Sixty four patients with at least 2 stones in the past 5 years and at least 1 within the past year before the trial were given placebo (33 cases) or potassium magnesium citrate (63 mEq citrate, 42 mEq as potassium and 21 mEq as the magnesium salt in combination pills) – 31 cases. Each pill contained 21 mEq of citrate; 2 pills were taken 3 times a day. The trial was designed to last for 3 years. There were 5 and 9 women in the placebo and treatment arms. Urine citrate excretions were not different before treatment (549 and 587 mg/day, respectively, nor were urine volume, pH, calcium, oxalate, or any other stone forming risk. After a one month grace period in which new stones were not counted, any passage or radiographic appearance of new stones, or growth of previous stones was considered a treatment failure. During the trial, 15 subjects left the treatment arm, 8 the placebo arm.
New stones or growth of old stones occurred in 63.6% (16 cases) of the 25 placebo cases who finished the trial and in 12.9% (2 cases) of the 16 treated cases who finished the trial. If the 6 subjects who left the treatment arm because of drug adverse effects are added in as treatment failures the drug effect remained significant (8 of 22 or 33%).
Of note, this particular formulation is not available in the US. A version of the supplement is available OTC but the dose per pill is so low that it is impractical for anyone to use it. So the trial is part of a proof of principle, but not actually applicable to clinical practice in this country.
Lojanapiwat et al (International Braz J Urol 37:611-616, 2011)
Unlike the Ettinger study, which concerned spontaneous stone formation, this study concerned new stones or growth of residual fragments after shock wave lithotripsy (SWL) or percutaneous nephrolithotomy (PERC). Their subjects were 80 initial patients, all 8 weeks after either procedure, and either stone free or having no residual stone fragments >4mm diameter (Numbers are in the Table). Hypocitraturia (<325 mg/day) was present in 20/39 who received citrate and 15/37 who did not.
| SWL | PERC | Total | |
| STONE FREE | 24(8) | 15(5) | 39(13) |
| RESIDUAL STONES | 26(17) | 11(9) | 37(26) |
| Total | 50(25) | 26(14) | 76(39) |
They were randomized into 39 treated and 37 placebo treated groups and followed for one year which 76 of the original 80 completed. Numbers receiving citrate in each group are in parentheses. Sodium potassium citrate was given as 81 mEq/day in 3 divided doses).
Of the 13 cases who were stone free and received citrate, 12 remained so vs. 15 of the 26 given placebo. Of the 26 who had retained fragments and were given citrate, 8 were stone free vs. 1 of the 11 controls and 16 others given citrate showed no change (13) or reduction in size (3) vs. 2, no change and 2 decreased size among the 11 placebo. These differences were judged significant at the p<0.05 level by the authors.
Soygur et al (J Endourology 16:149, 2002)
This trial considered 90 patients after SWL for lower pole stones who had residual stones <5 mm or were stone free. They were randomly assigned to potassium citrate (50 mEq/day in 3 divided doses) or placebo (Table). The trial lasted one year. The end
| Citrate | Placebo | Total | |
| STONE FREE | 28(0) | 28(8) | 56(8) |
| RESIDUAL STONES | 18(0) | 16(6) | 34(6) |
| Total | 46(0) | 44(14) | 90(14) |
points were stone free or not and residual stone size increased or not.
New stones occurred (parentheses) in none of the citrate treated stone free patients and in 8 of the placebo treated patients. Among the residual stone group, the fragments disappeared in 8 treated cases and failed to grow or shrank in the others vs. growth or new stones in 6/16 placebo cases. The differences in growth or new appearance were all significant.
Of course, both of these post treatment trials are subject to the biases of a radiography study, but observers appeared to have been suitably blinded to the patient groups.
Hofbauer et al (British J Urol 73:362-365, 1994)
In this trial, an equimolal sodium / potassium citrate was given in doses that maintained urine pH in the range of 7 to 7.2 vs. placebo. Therefore, although patients were allocated randomly to active treatment or placebo, the trial could not be blinded. By the three year endpoint, 22/25 placebo and 16/25 active drug subjects remained. New stones occurred in 16/22 placebo and 10/16 active drug subjects. This difference was not significant. This study is the only one with a negative outcome. It is also the only study that was not double blinded.
Barcello et al (J Urol 150:1761, 1993)
Stone formers with urine citrate excretion rates below 643 mg/day (3.4 mmol/day) were allocated to potassium citrate 60 mEq/day in 3 divided doses. Their mean urine citrate excretion was 359 mg/day. At the end of three years of followup, 20/28 placebo treated and 18/27 citrate treated subjects remained. New stones occurred in 14/20 placebo and 5/18 treated cases, a significant departure from chance.
GRAND SUMMARY
| NEW STONES | |||
| YES | NO | TOTAL | |
| TREATED | 20 | 115 | 135 |
| NOT TREATED | 77 | 71 | 148 |
| TOTAL | 97 | 186 | 283 |
Despite the variability of design, one can, with nerve, simply ask about the beneficial effects of citrate salts across all the trials. In all five trials 283 people completed the desired treatment period. Of these, 97/283 (34%) formed new stones or, in the case of the post procedure trials showed growth of retained fragments. Among all patients who were given citrate salts, 20/135 (14.8%) formed new stones or showed growth of retained fragments vs. 77/148 (52%) of those given placebo.
I have not added back the 6 cases from the Ettinger trial who left because of drug side effects.
From this we can reconstruct a sense of the value of the treatment as applied to the mixed practice of post surgical management and overall medical prevention.
Let us assume these numbers will hold for the future.
For every 1000 cases like the ones in the trials, 520 untreated cases will form new stones or show stone growth after a procedure vs. 148 cases/1000 cases with citrate, a savings of 372/1000 cases overall.
I realize I am not calculating in the most satisfactory manner as a statistician, but I rather like the coarse grained, even vulgar nature of my count me up.
QUALITY OF EVIDENCE
A Personal View
The trial community exhibits the kind of methodological fussiness one expects and applauds in any scientific situation. Among their ilk the citrate effect is viewed as modest at best, the evidence, by their likes, fair.
I am sure they are right according to the mores and social instincts of this discipline, but I do not come from nor inhabit that discipline, and therefore have an altogether different way of counting – for that is all one does after the impatient and often indifferent subjects have played out their roles in the work.
How likely is it, I ask myself, that citrate salts do not prevent new stones or fragment growth?
Not at all likely.
Why assume anything but that blinding was performed when specified, that radiograph readers were competent and blinded to the groups patients were in, that stone events were counted fairly and compared to radiographs to estimate new stones? If we make these assumption of honesty and skill, the marked downward skew from alkali is just too large to be by chance.
My bet will be on the drug, and if I bet that way, I will always win.
Do We Need More Trials For Calcium Stone Formers?
For me, no. It would seem a waste of money.
Some trials treated patients with reduced urine citrate, others did not. Some trials looked at new stones over 3 years, others at residual fragment growth one year after urological procedures. Will another 50 or even 100 cases be likely to change the outcomes? If so, in what way, and why?
It is true that one trial showed no effect and that trial was not blinded. It is actually a drag on the results as I did not remove it.
We Do Need a Trial of Citrate for Calcium Phosphate Stone Formers?
I do not know how often this must be said. Calcium phosphate stone formers must lurk in each of the trials I have reviewed, but I do not know their outcomes. One trial insisted stones be at least >50% calcium oxalate. That means perhaps a few had considerable phosphate is stones.
Calcium phosphate crystal formation is sensitive to urine pH whereas calcium oxalate stone formation will not be. The reason is that calcium phosphate supersaturation requires divalent phosphate be present, and the pKa for the second proton is about 6.8. Citrate salts can raise urine pH, so they can raise supersaturation with respect to calcium phosphate salts. On the other hand, citrate is an inhibitor of crystallization both because it is calcium binding and because it directly affects calcium crystal growth.
ROLE OF TESTING
The very same ACP report from which I derived the studies shown here presented an annoying set of comments that infers we might as well just give a drug like potassium citrate without knowing stone composition, or doing serum or urine testing that concerns stone pathogenesis.
For this reason, I offer some remarks on that subject. This is in the special context of citrate treatment. I have made more general remarks of a negative sort about the APC comments.
Does Stone Analysis Matter?
How can it not? I have already mentioned the problem of phosphate stones. Do we not have to exclude struvite is stones? The odd patient with cystinuria who has slipped by? Drug stones? Conversion from calcium oxalate to calcium phosphate stones?
Do Serum and Urine Testing Matter?
How can they not?
SERUM
Do we want to give potassium loads to people with reduced renal function?
Having prescribed potassium, do we not want to monitor for serious increase in serum potassium; some patients are older, some diabetic, some take ACE or ARB medications, some age or change drugs over the years we treat them.
Do we not want to diagnose primary hyperparathyroidism? You cannot without serum testing and 24 hour urine testing to be sure calcium excretion is not low.
24 HOUR URINE TESTING
If we do not obtain and measure 24 hour urine samples, how can we know anything? Some patients may have very high urine citrate levels. Some may have very high urine pH values.
Here and there urine oxalate is very high, from primary hyperoxaluria, or occult malabsorption syndromes, or very odd food habits.
People change their habits and develop diseases.
Moreover, people do not always take their citrate. Fall in urine ammonia in relation to urine sulfate, and rise in urine potassium assure one they are taking the drug.
URIC ACID STONES
Do We Need a Trial for Uric Acid Stone Formers?
NO
No one really questions that alkali salts will raise urine pH, nor that raising urine pH will reduce uric acid supersaturation and prevent stones. It is common practice. I doubt anyone will pay for or perform an RCT to test this question.
That they will not is very important, because it raises an unexpected question.
WHY NOT?
We Know the Chemistry
Uric acid is a large flat mainly hydrophobic molecule with most of its charge on a single proton receptor site. The protonated from has a very low solubility in urine of around 90 mg/liter whereas 24 hour urine uric acid excretion ranges from 400 to over 1000 mg daily depending upon diet purine loads. The pKa of the proton receptor site is about 5.3 in urine.
Given these facts we can calculate uric acid supersaturation from the urine concentration of total uric acid and the pH, along with minor adjustments for the effects of ionic strength on the pKa. High supersaturation will lead to a snowstorm of uric acid crystals. Raising urine pH to above 6 will generally reduce supersaturation below 1 and end uric acid stone formation.
Everyone Knows Alkali Work
There is a lot of uric acid excreted every day, so uric acid stones can grow rapidly. Uric acid gravel has an orange red color and is often seen. When alkali are given, the gravel goes away only to come back if patients miss doses. The absence of new stones is obvious.
No One Treats Without Stone Analyses
Who can be sure of stone composition without stone analysis? Even during treatment of someone who has produced uric acid stones, calcium oxalate or calcium phosphate stones may begin. So people know the stone type, and proceed by custom.
No One Treats Without Testing Serum and Urine
Uric acid stones are common in diabetics and people with reduced renal function; potassium loads are potentially dangerous. Perhaps this is more obvious among uric acid stone formers than calcium stone formers, although given wide spread use of ACE and ARB drugs and NSAIDS, potential risk is everywhere.
The amounts of alkali needed can be variable, and the only reliable way to ascertain is 24 hour urine testing. Likewise for compliance.
Therefore routine practice monitors before and during potassium citrate treatment of uric acid stones.
TRIALS ARE UNNECESSARY
IN this situation, no one has and probably no one will propose a trial of alkali for uric acid stones. But, there is an almost exact parallel situation for calcium phosphate stones, yet such certainty as pertains to uric acid stones certainly does not exist.
CALCIUM PHOSPHATE (CaP) STONES
Do We Need a Trial for CaP Stone Formers?
YES
WHY?
We Know the Chemistry
Calcium cannot combine with mono-valent phosphate but only with the divalent form. The pKa for dissociation of the second proton of phosphoric acid is about 6.8 in urine, although the precise value varies with ionic strength. Given the molarities of total phosphate, calcium, citrate – which binds calcium – and other ligands that have modest effects, the supersaturation of brushite – the usual initial urine CaP phase – can be calculated as well as we can calculate the supersaturation for uric acid.
Like uric acid, phosphate and calcium are abundant in urine, so the amount of crystal that can be produced in a day is similar to that of uric acid. Therefore stones can, and do, form rapidly and become large.
As in the case of uric acid, high urine CaP supersaturation can produce snows storms of crystallization; though certainly not common, patients can recognize this as white urine.
On physical chemical grounds, to lower CaP supersaturation below one and keep it there is to prevent CaP stones as surely as one prevents uric acid stones by raising urine pH and lowering supersaturation below one. Why, then, is not this treatment as self evident as alkali for uric acid stones?
Everyone Does Not ‘Know’ Treatment Works
We have no drug corresponding to alkali.
We can raise urine pH safely but cannot lower it.
Acid loads raise urine calcium losses and can be detrimental to bone mineral balance. Higher protein intake is a possible way to lower pH, but not all kidneys respond to acid with a prompt fall in pH. In some cases urine ammonium ion excretion will rise. In others, acid retention may occur. Urine calcium will tend to rise.
So treatment is not as transparent as for uric acid.
But Treatment Must Work Exactly the Same Way
We can lower CaP below 1 with fluids and measures – reduced diet sodium and thiazide – that reduce urine calcium, and we can monitor supersaturation as we monitor urine pH and uric acid supersaturation.
Furthermore, patients can tell if white urine has ceased.
Moreover, because stones are often actively forming, effective treatment is reasonably obvious.
However, these measures may be difficult to achieve. Thiazide is not always tolerated, reduced salt diet not always maintained.
Citrate is a powerful inhibitor of crystals, and it would be good to know if it were beneficial for the CaP stone former.
Dear Dr. Patel, Thanks for a great question, and very pertinent to the article on citrate.
For CaP stones, the idea is to get as much citrate as possible without raising the CaP SS. Some patients tend to respond with a lot of citrate and not so much bicarbonate excretion, so their urine pH does not rise overly. Others are remarkably poor in citrate response and excrete lots of bicarbonate, so urine pH goes up, CaP SS goes up, and citrate, what you want, is not impressively increased. So, what I do is give about 2/3 of the ammonia (main acid excretion) daily, and measure. If citrate has risen, I look at CaP SS. If it is above 1 – 1.2, I use whatever combination of higher fluids, reduced Na intake, or even thiazide to bring it down.
For uric acid, things are easier. The ‘guideline’ is to bring the pH to above 5.5; I pay no attention to that but usually give alkali equal to the daily ammonia excretion and measure. My goal is to bring uric acid SS below 1, and I like the 24 hour urine SS – an average, after all – to be <0.7 to have some room for variation during the 24 hours of the day and night. I watch the CaP SS, which means I do not let the pH get much above 6. I think the last dose of K citrate is best given before bedtime – as GI tolerance permits.
Regards, Fred Coe
Sir,
I’m a 40-year-old man who has passed three calcium oxalate stones in his life so far. Needless to say, I’d do just about anything to prevent the recurrence of stones. If taking a potassium-magnesium citrate supplement helps with this, I’m ready to take it. However, I would need some guidance re dosage. I’m based in Europe and the only supplement I have been able to locate is this: http://www.pureencapsulations.com/potassium-magnesium-citrate.html
One capsule contains 140mg of potassium citrate and 70mg of magnesium citrate.
Question is, how many capsules should I take each day in the hope of preventing stone recurrence?
Thank you very much for your reply.
Do you have any comments or advice on the use of sodium citrate?
The advantages of sodium citrate is the lack of potassium with all its problems. The problem is the sodium load. If the agent is being used to raise pH or citrate and urine calcium is normal, and blood pressure is not a problem, sodium alkali should be fine. But the sodium can raise urine calcium excretion and thereby raise stone risk. I use it for uric acid stones when potassium loading is inadvisable because of diabetes or concurrent medications which alter potassium handling by the kidney. Otherwise I use the potassium salts. Regards, Fred Coe
Thanks!
Potassium bicarbonate and citric acid are cheap at Amazon, 100/190 weight ratio is equimolar, has anyone tried to make a solution that is palatable and tried BID or TID dosing?
Hi, We have an issue about measurement in ordinary household situations. Potassium is always a worry if the amount should be way off for someone. I agree bulk material – which is what I presume you refer to – is inexpensive. Can you provide a link to the product you are speaking about? If bulk can you think of a way to safeguard against overdose of potassium in a home measurement environment? Thank you for the effort, Regards, Fred Coe
potassium bicarbonate: amazon.com/gp/product/B0064GZPU4?psc=1&redirect=true&ref_=oh_aui_detailpage_o01_s01
citric acid: http://www.amazon.com/Spicy-World-Citric-Acid-5-Pound/dp/B000OZFECU/ref=sr_1_6?ie=UTF8&qid=1434900344&sr=8-6&keywords=citric+acid&pebp=1434900367299&perid=088Z51KJGNGB780XN4YT
I agree that adequate measurement of the potassium dose is of the utmost importance, making a solution will not be the right approach for everybody, but it can be done.
In my area the lowest cost for 90 tablets of 10 meq of potassium citrate is $81.89.
Getting an accurate scale and careful measurement could result in significant savings. Gunpowder scales are fairly accurate and one could be dedicated for food use.
http://www.amazon.com/GUARANTEED-Precision-Gunsmithing-Gunpowder-Ammunition/dp/B004HN0YL6/ref=sr_1_4?s=sports-and-fitness&ie=UTF8&qid=1434902724&sr=1-4&keywords=gunpowder+scale&pebp=1434902757404&perid=1FY5DJE0B5ZP102H7TC9
Some entrepreneurial pharmacist could make the solution, Cytra-2 from Cypress Pharmaceuticals is labeled “Medical Food for Urinary Health” even though it is Rx.
Since we advise patients to drink plenty of water, one approach could be to make a 1-2 liter solution of potassium citrate-citric acid, non-caloric sweetener and flavoring to taste to make it the oral hydrating solution for daily use. The question is how much potassium bicarbonate/citric acid per liter, how often an electrolyte panel needs to be measured while titrating the dose and for maintenance surveillance. Adding HCTZ, if tolerated could also help manage the calcium and potassium balance.
My confession: I’ve had to undergo 2 ESWL and one laser lithotripsy procedures, I am looking for ways to prevent another stone, I live in Ohio, in the border of the “stone belt”. I am a patient and a Family Medicine Physician.
Hi, Dr Ballester. In your case, being a physician, I am sure a solution process is safe – you are fully trained and understand the issues. For most people, who lack such training and expertise, I am hesitant, as I suspect you are, too. A reasonable concentration is about 20 mEq/liter, which is about what one gets from Crystal Light – an inexpensive beverage fully approved for people and on sale everywhere. It has an artificial sweetener, I have been told, and some do not want to use it. But whatever you do by way of making your own potassium citrate solutions, I cannot recommend it for non physicians, nor would you, unless there were extremely effective safeguards. Potassium is potentially dangerous, as you well know, if taken in excess. Warm Regards, Fred Coe
Thanks!
I am a mass producer of uric acid stones. Just had them removed and have had a nephrostomy tube for several weeks. This is the second time I have had to have this done – the first time being 6 years ago. It is not something I want to repeat. Each time they have removed approximately 100 stones – with lithrotripsy being done 7 times in between. What would your suggestions be to bring a halt to the mass production?
Hi Phyllis, I am a bit puzzled. If the stones are really uric acid then raising the urine pH to above 6 with potassium citrate will make their formation impossible: Physically impossible. I cannot imagine you have not been given that medication already and so assume you continue to make ‘uric acid’ stones despite a urine pH at which they cannot form. So: Firstly, be sure you are on potassium citrate or other alkali and your 24 hour urine pH is above 6; secondly, if you are on such treatment, be sure the doses are spaced out over the 24 hour day so there are no dead spots – long intervals between doses in which pH could fall, especially overnight; thirdly be sure you see the stone analyses and that the stones are uric acid not some salt of uric like ammonium acid urate which is an entirely different matter. Have many stones analysed as labs can be faulty – there are 2 8 dihydroxy adenine stones, there are other odd stones. But overall be sure of this: Real uric acid cannot form and will even dissolve at a pH above 6. Let me know. Regards, Fred Coe
Thinking of kidney stones in terms of inorganic crystal growth, the problem is not the formation of crystals per se, but the formation of large crystals. Of course, the surest way of preventing crystal formation is to keep supersaturation continuously below 1.0. But with supersaturation >1.0, crystal size decreases and crystal number increases with increasing saturation, because high saturation favors spontaneous nucleation and competition between crystals. Given that, it seems like reducing the concentration of stone-forming ions might not always be the best approach if the concentration of at least one of the ions cannot be reduced to below supersaturation, and that increasing saturation actually might be better, by working to prevent the formation of large stones even as if favors the formation of small ones.
Dear Joseph, Your remark is, of course, correct and it is clear you are professionally knowledgeable in this area. The kidney stone development is complicated massively by the urine proteins and proteoglycans which modify nucleation, growth and aggregation of crystals and ‘glue’ them together into what amounts to a crystal/protein composite material. By last count of our proteomics colleagues urine contains about 1,800 individual proteins and peptides, many of which are anionic and therefore prone to attach to nascent crystals. Stones themselves, when crystals are dissolved out, have a ‘matrix’ we have found contains about 800 – 1000 proteins, many of which are probably random adsorbents others highly active in the production of the stones. Under these circumstances, the effects of supersaturation on crystal size are not critical – crystals that form immediately engage with urine proteins and begin the complex process of making the composite – and in fact many small crystals are a fine way to gather in a lot of ‘matrix’ and make stones. That is the reason lowering supersaturations is so favored as a treatment. Thank you for putting up so useful a comment. Regards, Fred Coe
Thank you. You’re site is wonderful. I’ve been reading through it for hours now. It’s rare to find such critical discussions of basic science applied to medicine.
I am a vertebrate paleontologist turned isotope chemist specializing in medical applications, especially of Ca isotopes. On the paleontology side I’ve done some work on very early mineralization of buried animals, and struvie is one of the first minerals to appear. So all of that primed me for an interest in kidney stones. On top of that I passed a stone, for the first time, last week, and so have been looking for good information.
Which leads me to another question. My physician wasn’t interested in analyzing the stone fragments I collected, but I thought that I should at least rule out struvite, so I took a ca 1mm fragment and heated it to around 400°C on my stove, smelling it the whole time. It released water vapor and later some smoke, but never any ammonia that I could smell. From that can I conclude that it was not struvite (which should release ammonia at around 155°). It also did not darken appreciably, which should exclude apatite, which leaves plain old oxalate. The sample I have left is just enough for Ca isotope analysis, so I’d rather keep if for that.
Hi Joseph, Struvite would have been an uncommon crystal for a male – it is formed in human urine only by urea splitting bacteria which are not at all expected in an otherwise normal urinary tract. In soil they abound, of course. I would have the stone analysed via FTIR which is reliable enough. LIkewise I would have proper studies done of blood and urine to find out why you made the stone and so as to insure against more of them. The calcium isotope studies of stones are indeed interesting, and offer a kind of time – geology view. Let us know. Best, Fred
Thanks you. I will do that.
I was looking through your article and wanted to know if there was something you could recommend as an ‘over the counter’ pill on the market I can take in lieu of consuming straight pure lemon juice. That is the program my current urologist has me on for my kidney stones. 1 cup of fresh squeezed lemon juice a day. So far it has worked but it’s so expensive and time consuming to squeeze the lemons daily for this. I also travel a lot for work which makes it especially difficult to keep up the regimen. If there was a pill form of Uric acid on the market that was as effective that would be a lifesaver. Any suggestions? Thanks for your help!!
Hi Tad, I think lemon juice is indeed burdensome and also not an ideal approach. The amount of citrate available will vary with the acidity of the juice, and it is indeed not inexpensive. If indeed you do need potassium citrate as a treatment for your stones, then there are a lot of alternatives. One is simply prescription potassium citrate pills to be used for convenience while traveling. Then, there are a lot of less expensive workarounds people are finding to get the dose of potassium citrate needed. Beverages have potassium citrate – same link. Crystal Light lemonade, one liter is equivalent to two 10 mEq potassium citrate pills. Here is my problem with your question, however. Using lemon juice I cannot tell how much potassium citrate your physician wants you to have. I think a cup of fresh squeezed lemon juice is good for no more than the equivalent of 2 potassium citrate pills, but this may vary with the ripeness of the lemons. Another problem is what are we treating? IF it is uric acid stones, then pills are the only safe way to go; such stones can grow rapidly and potassium citrate in the proper dose is an absolute prevention – always works. If it is to prevent calcium stones, I presume you have a low urine citrate level, and then the needed dose of citrate will depend on your urine results. Perhaps you should check on these two points and then reconsider how your treatment needs to proceed. Regards, Fred Coe
Dr. Coe , I’ve been searching for a solution for quite some time and there’s so much misinformation on the internet so it was wonderful to find your site.
My situation, three years ago I passed a small fragment of are very large kidney stone. I had it analyzed and it was 80% uric acid 20% calcium. I had a SWL but when I woke up from the procedure the Dr. said he was only able to reduce it not get rid of it because it was too soft. I asked him what we can do about it and the answer was that I could try taking potassium magnesium citrate but he doubted it would do anything. I started taking the prescription and he scheduled to come back in several months to review everything with him. No discussion of diet or constant PH tracking. At my next checkup it showed that my kidney stone was back to its full size and there were some additional smaller stones. This time we scheduled a procedure using a laser to blast the stone into small fragments and pull out the smaller pieces. I woke up from this procedure and my urologist had that same puzzled funny look on his face and then said to me that once again he was unable to completely remove the stone. He said it was bouncing around a lot and the fluid got too cloudy to see so he had to stop after 45 minutes. Frustrating!
Up to this point my diet was terrible, it consisted of a very high percentage of red meats, sugar products, refined flour products and diet coke. After some discussion with a friend who eats healthy and doing some internet searching I decided to change to a plant based diet. However my PH was still under 6 with occasional peaks above 6. Now I am once again facing having another SWL with a different urologist. The CT scan and ultrasound show I have a 2 cm stone and several smaller ones. I did ask my new urologist about diet and PH and was told by him it would not make a difference. He’s very nice and a personable doctor but he just seems too eager to get me into the operating room. I’m a big believer in modern medicine but I just don’t understand why my doctors are so quick suggest invasive medical procedures rather than discussing a natural treatment.
In the last two months I’ve started a juicing campaign with a majority of my meals consisting of juices made from 80% vegetables and 20% fruits – Lemons Limes mostly – I’m following one of Joe Cross’ reboot programs – Look up Fat, Sick and Nearly Dead, and I exercise vigorously on a regular basis. Yes I have lost weight and feel better but the big stones are still there causing moderate pain. But I see that what you have said above how important it is to consistently keep one’s PH at six or higher which is the first time I’ve heard this so I’m hopeful this holds true for me so as of today, I’m putting it in place.
Since starting my juice diet I have found it interesting that some combinations of veggies and or fruits still produce a PH under six for me and some combos higher. Even though I have my last meal the night before of leafy green vegetables including kale apple and lemon juice my morning PH before breakfast was 5.5. It could be lower as my testing paper scale is 5.5 – 8.0. I have tested lower than 5.0 at my doctor’s office in the past. I just discovered in the last few days that Ceylon cinnamon seems to be the best at raising my PH closer to 7.0 than anything else. Celery, almond and of course the green leafy veggie raise it but not as well as the cinnamon. I just started tracking my types of food intake and their PH results on a 24/7 basis about three days ago.
Which leads me to my questions:
Does it matter what you use to raise your PH? Medicine VS food? Vegies and spices are my preference.
Should I ask my doctor for a specific blood & urine test and how often should I do it?
If I keep my PH 6 or higher 24/7 how long might it take to get rid of a 1.1 cm non-shadowing stone and multiple smaller stones ranging from 3-mm? I know everyone is different and you haven’t seen my medical history I’m just trying to gauge how to proceed with healing myself and how to get my doctor on board with me.
Thanks
Tim
Hi Tim, The 80% uric acid part of your stone will respond to an increase of urine pH. Uric acid stones do grow rapidly and can become very large. I would not try to use potentially confusing and variable food treatments for this but take potassium citrate at a dose sufficient to raise your urine pH above 6 but not much higher than 6.5. Your physician needs to do proper 24 hour urine testing to gauge the dose, and do follow up testing to assure a proper result. The other 20%, which is no doubt calcium oxalate – although I have been surprised here and there – requires some care as well. The same 24 hour testing will disclose any primary disorders that might be causing the calcium stones and these need to be treated. As for all of the rest, your diet needs to accord with your calcium stone risks, and leave the uric acid problem to raising the pH with potassium citrate. Fred Coe
Thank You
Thank you for the article. If one simply had to raise the pH of urine then bicarbonate would work. Do bicarbonate salts not inhibit crystal formation? Is a citrate blend better for a pregnant patient? i.e. magnesium/calcium/potassium citrate.
What is the toxic dose of potassium citrate or rather at what dose may it cause arrhythmias in the mother or fetus?
Hi Jason, When you take in any alkali the response of the kidney is normally to reduce reabsorption of filtered citrate so it can enter the urine. Citrate specifically binds calcium in a soluble salt and also reduces formation and growth of stone forming crystals. So, any alkali, including bicarbonate, will have the same effect on urine citrate. But, sodium increases urine calcium losses and many stone formers have genetic hypercalciuria, so potassium salts are far more preferable. WIth normal kidney function potassium loads commonly used are harmless. Regards, Fred
Thanks for the reply and the links. With normal kidney function harmless in pregnant women or harmless to non-pregnant people? Do you have experience treating pregnant women with kidney stones? Magnesium citrate and Potassium citrate are both listed as category C so some physicians are hesitant to recommend it. If calcium citrate is taken with food containing oxalates I wonder if calcium will bind to the oxalates and citrate will be absorbed in the small intestine – I don’t know the affinity chemistry or which has a stronger bond. I think Oxalobacter forminges may be deficient in frequent stone formers, especially having frequent UTI’s and antibiotic therapy. Do you link there is also an underlying liver issue? The liver produces excessive amounts of oxalates?
Hi Jason, In the US we do not have the magnesium potassium citrate preparation. Potassium citrate would be of no concern during pregnancy unless the woman had a form of renal disease. As for calcium citrate, calcium will bind oxalate in the intestine and reduce its absorption; the affinity of oxalate for calcium exceeds that of citrate. As for oxalobacter deficiency as a cause of kidney stones in humans, the issue is as yet not resolved. As for abnormal liver oxalate production in stone formers, there is little evidence to support the idea apart from the established 3 primary hyperoxaluric states. Regards, Fred Coe
You can get the magnesium/potassium preparation from pure encapsulations. I gather, since oxalates have a higher affinity than citrate for calcium then that means citrate is only used to raise urine pH levels and discourage oxalate stone formation AND citrate does not slowly break down calcium oxalate crystals in the kidney. As far as I know there is not, unfortunately, a drug or substance that slowly breaks down stones in the kidney, correct?
Hi Jason, Although oxalate binds calcium more strongly than citrate, citrate does compete and lower the available calcium so that supersaturations with respect to the calcium crystals are reduced. See the article on calcium binding by citrate. Citrate disorganizes the surface growth patterns of calcium oxalate and apatite crystals so growth is reduced but because of almost invariable urine calcium oxalate supersaturations citrate does not dissolve calcium oxalate crystals in kidneys. There is no way to dissolve the calcium stones. Uric acid, cystine, and possibly struvite stones can dissolve. Regards, Fred Coe
Why did you think this preparation was not available in the U.S.?
(magnesium citrate) 70mg
(potassium citrate) 140mg https://www.pureformulas.com/potassium-magnesium-citrate-180-vegetable-capsules-by-pure-encapsulations.html#sthash.8Z4hUfk1.dpuf
Hi Jason, The product of potassium magnesium citrate sold OTC in the US is at a small dose compared to common usage – at minimum 20 mEq of the citrate moiety – so a large number of tablets would be needed every day. Regards, Fred Coe
Hello, Just stumbled upon your website, ( I’m a 53 year old female)
I was offered what was referred to as a ” Lemonade” pill and have been drinking water with lemon instead. I first made stones over 22 years ago – all calcium phosphate. Then, 2 years ago new stones were discovered. They have all been clearing out this year, some required Lithotripsy help. As I had changed to a healthier diet a few years back …. these stones were mixed – Calcium Oxalate/ Calcium Phosphate. It was also discovered that I have a caylceal diverticulum with some or a stone inside. Am I stuck on a Stone merry go round due to these factors?
Hi EB, I do not know what a lemonade pill is but I suspect it is potassium citrate. In the right patients it is ideal, for calcium phosphate stones is may not be. You have not so far had what I would call organized prevention, and should have it; in particular, part of your program might be a thiazide diuretic. The diverticulum is a blockage of a small part of a kidney leading to a focus of crystals; it can be left as is unless it is painful or becomes infected. Surgery for it is never shock waves. Get prevention organized as I have presented it, and lets hope there are no more stones. Regards, Fred Coe
Hi Dr. Coe,
For a couple of years, I took calcium containing antacids several times per day for reflux. Suddenly at the age of 40+, I had my first kidney stone (calcium oxalate). Could the stone be related to the antacids? Since the stone, I’ve switched to H2 blockers instead. Thank you.
Hi Richard, Indeed there is a literature, albeit descriptive, linking calcium based antacids to calcium stones. The switch is a good thing. Be careful, though. Get a proper evaluation to be sure there is not another reason, one that can be treated to prevent more stones. Regards, Fred Coe
Thank you so much!
I miss Divya Anil Popat 19 yrs studying bpharm.I am suffering from uric acid stones and i have it in both the kidneys.2 years back i had lithotropsy done.but now from my recent reports the stones have been formed again in both the kidneys..kindly provide me with some solution to prevent it from forming again
Hi Divya, Uric acid stones all can be prevented by taking alkali in sufficient doses to make the urine less acidic. Potassium citrate will do this, and you should be on it. In fact any alkali is better than none. You should have 24 hour urine testing if you can obtain it. The link tells you how to read the report so you can work with your physician to prevent more. It also shows how these stones form. There is no reason to ever have another uric acid stone. Be sure and take some form of alkali. Regards, Fred Coe
thank you for your valuable guidance
Dear Divya, I am glad. Good luck with prevention. Come back some time and say what happened. Regards, Fred Coe
I just got back the results from a 24 hour urine test. Calcium oxalate supersaturation was 1.53 and Ph is 5.6. Specimen volume is 2.66 L. My oxalate rate is 48 (norm shows <45).
Is the Crystal Light flavor the pink or yellow lemonade? I'm drinking 100 ounces of water a day (mostly). I'm on a low oxalate diet but I'm also eating a lower carb diet. I don't eat dairy because it causes bad joint pain. Is this a diet that will increase the risk of stones? I never had stones before I started eating lower carb. Thank you for your time.
Hi Georgene, what about your other urine findings? Calcium, for example. Your oxalate is high and a common reason is a low calcium diet. Check the low oxalate diet article. Unless you are taking in 1000 mg of calcium daily, raise your intake and recheck the urine. The calcium may cure the oxalate problem. The article gives a lot of alternatives for oxalate as well. Crystal light would matter if your citrate was low – was it?? Regards, Fred Coe
I have a patient with joint pains who took too much vitamin D by mistake, causing his level to rise to 300 ng/dl. A couple of months later, he gets his first kidney stone, calcium phosphate. Is there a connection? My patients tend to have more alkaline urine because I recommend a plant-based diet. In his case, I will recommend what I read online, increasing urine volume, restricting sodium, avoiding citrus, soda and keeping animal protein below 6 oz/day. But I love your rigorous analysis of the situation and would much appreciate your thoughts on this. If his stones recur, I will recommend thiazide diuretics but otherwise I tend towards diet and lifestyle and not medications (due to plethora of unanticipated long-term side effects). Some have also recommended thiazide diuretics paired with citrate supplements. Thank you!!
Hi Dr Ashe, I do agree that the vitamin D excess is a likely cause of hypercalciuria and stones. The phosphate no doubt reflects higher pH from diet as you mentioned. I would be guided by the urine calcium; if it is still high reduced Na diet and high fluids would be good; thiazide is also good unless the vitamin D excess is still important which would produce hypercalcemia with thiazide. I woud shun citrate supplements because of the phosphate stone. I would do a CT if not done already because nephrocalcinosis may be present. Regards, Fred Coe
I am an otherwise extremely healthy and active 55 year old woman. I had my first kidney stone (calcium oxalate) 7 years ago. Luckily it passed within 8 hours. Just had my second and was in so much pain wound up in the ER. Luckily it passed the next day. Also calcium oxalate. While I was in the ER they did a CAT scan which said ” There are bilateral renal calculi. The largest on the right measures approximately 5mm and the largest on the left measures approximately 4mm. ” I followed up with a urologist who didn’t conduct any further tests but gave me a list of foods high in oxalate to avoid. I was still concerned so I followed up with my Primary physician. He tested my parathyroid – normal and did a 24 hour Urine Test. The results were everything in the normal range except for: Calcium 164, Citric Acid (Citrate) 242 and Phosphorus 523. My oxalates were 16. PH was 6.7. So do I really have to stick to a low oxalate diet? I am really afraid to take Urocit. Not because of the cost but because of the side effects. I don’t want to feel sick to my stomach every day because of a medication that I’m taking for an issue that happened twice over 7 years. I have researched this to death and there is so much conflicting information. I would appreciate any suggestions you have. Thank you so much.
Dear Lauri, Your urine oxalate is very low and I do not think a low oxalate diet is useful or worthwhile given that fact. Your urine citrate is low and perhaps your physicians might want to consider potassium citrate or an alternative alkali. if you are afraid of potassium citrate consider beverage alternatives – see the article on the price of potassium citrate. High fluids would always help. Regards, Fred Coe
Thank you for your response. Is the only alternative alkali Crystal Light Lemonade?
Hi Lauri, It is but one of many. Try the article on pricing of potassium citrate and read through the comments. Regards Fred Coe
Dear Dr Coe,
Great website! Is there any way to predict how much oral citrate is needed to raise the urine citrate to certain levels? in my case my urine citrate was 151 ( calcium 174, oxalate 23, na 104, uric acid 468, vol 2600) and my stone in the past was calcium oxalate (I had a calcium oxalate stone in 1981 when I was an intern in Milwaukee and saw Dr Leman , the workup was all normal so idiopathic, but no urine citrate then. No recurrances till this year when 5 mm stone seen on ultrasound, asymptomatic) I also have idiopathic osteoporosis, on Forteo. Urine calcium was 160 pre Forteo so I’m not too concerned that the Forteo is a big risk factor for stones.
Thanks
Hi Chris, Jack was a close friend; you saw a great physician. You seem to have the low urine citrate condition without other abnormalities and calcium oxalate stones. As such potassium citrate is ideal as trial data support it as a treatment for prevention. Although one tends to think of idiopathic hypercalciuria in a stone formers with bone disease I guess you do not have that condition. Be sure your diet calcium intake is ample. The dose of oral citrate is hard to calculate. I would start with 10 meq BID and re measure; if you need more double the dose. But, not everyone responds with increased citrate only higher pH; in that event stone using it and consider other means. Regards, Fred Coe
Dr Coe
If I wanted to moderately limit my patient’s overall potassium intake but still needed to treat low urinary citrate, could they take a combination of potassium citrate and magnesium citrate? Not the liquid mag citrate for the GI cleanout, but mag citrate powder. I have heard that Sodium bicarb and sodium citrate may also be useful, but I worry about the sodium levels too.
In line with the referenced Ettinger et al trial above, If aiming for 40meq of Kcit per day, would 20meq of Kcit and 20meq MgCit accomplish the same thing? They are both alkali, right?
Thank you for your wonderful and informative website.
Hi, I am not sure if the magnesium citrate will be well absorbed or tolerated. I would guess your patient has uric acid stones and type 4 RTA with some potassium handling difficulties. My approach is to use sodium bicarbonate – the bicarbonate fosters sodium loss so volume retention is not so marked or I use potassium citrate with a thiazide like chlorthalidone 25 mg daily which prevents a rise in serum K, or I use sodium bicarbonate with the same thiazide. In all cases I get the urine pH up and avoid a rise in blood pressure. Let me know your thoughts, Regards, Fred
Thanks for answering so quickly.
I was basically trying to mirror the Ettinger article you cited above (J Urol 158:2069-2073, 1997).
It looks like they used a combination of potassium citrate (~40meq/day) and magnesium citrate (unsure of the amount but to a lesser degree) and had statistically significant decreases in urine citrate and increases in urine pH.
I know that plain old potassium citrate is much more common these days but thought that trying to bring back potassium/magnesium citrate might be a different strategy. But then again I’m no Charlie Pak or Fred Coe!
regards – Frank
Hi Frank, I see your point; the preparation Ettinger used is not available here in the US. It would be good if it were. Sorry I did not get your exact meaning. You are right, it would be a valuable alternative for this patient. Regards, Fred
Any insight as to how or why potassium citrate won out over potassium magnesium citrate as the most common med for low urine citrate?
Dr. Pak’s early data from the late eighties and early nineties seems to indicate that the K Mg Cit provided a more robust citraturic response when compared to K Cit alone.
Hi Frank, I think Mission either decided to go with Urocit or perhaps the patents on the Mg formulation were not their own. I agree with you we could use the Mg preparation but alas! Regards, Fred
Thank you for this article. I have CKD4 and hypoparathyroidism after acute renal failure caused by kidney infection. I develop large (10+ mm) stones after UTIs – calculi that were not there at the time of the first UTI. (I was told to take extra Vitamin C to help fight the recurring UTIs, which I now think was bad advice.) Analysis shows the stones are at least partly calcium oxalate, but there was a suspicion that was the outside, not the inside (although no one told me what the inside might be).
I would be concerned about potassium citrate on a daily basis because of CKD4, but magnesium citrate could help. I take magnesium to help prevent migraines. I could switch to a low potassium diet to allow room for potassium citrate, but would being able to add potassium be sufficiently better than only magnesium citrate?
Dear Linda, CKD 4 puts you into a different world from that of ordinary stone formers. You are right- do not take potassium salts of any kind without nephrology supervision. Do not take magnesium salts either without direct supervision. This site is for your information but you are so special a case that nothing I say here can be done without direct medical review by a nephrologist. I do not say this to protect me or my university, I say it to protect you. CKD4 is serious kidney failure, and the kidney failure dominates all discussions for your care. I am afraid the stones may be struvite – be sure about this. The acute renal failure must have followed not only infection but either infection with sepsis or obstruction with infection. Warm Regards, Fred Coe
I have had a calcium oxalate stone. I was just diagnosed with osteoporosis and have to take calcium. My urologist said calcium citrate is ok for me. Do you agree? I have a duplicated ureter on one side, so a 3 mm stone would not pass as the ureters are very narrow.
Hi Susan, I imagine you have idiopathic hypercalciuria which can cause bone mineral loss as well as stones. A 1000 mg calcium intake is ideal, from foods if possible. If not, then supplements are used to add what food cannot provide. Take the supplements with a main meal, never alone. Any calcium supplement will work, so shop for price. A very low sodium diet will help reduce bone mineral loss, and lower urine calcium loss and stone risk. Be sure your urine volume stays about 2.5 liter/day despite the low sodium. Regards, Fred Coe
Would Magnesium Citrate help in reducing the occurrence of Calcium oxalate stones?
Hi Pascal, We did review the magnesium potassium citrate product in this article. Magnesium citrate itself has not been tried and might have GI side effects. Regards, Fred Coe
I just had a ureteroscopy (and stent) to remove a 6mm uric acid stone. I am now taking a 1080 mg Potassium Cirtate tab once daily and drinking 100 ounces of water per day. Is this sufficient to prevent another stone or is other diet alteration needed? Could other types of stones be formed instead without diet changes?
Hi James, You need enough potassium citrate to raise the pH of your urine above 6. That will prevent any uric acid from forming. As for other types of stones, one would have to know that other abnormalities you have. If the urine pH is brought to 6 there are no diet changes needed for uric acid stones. Regards, Fred Coe
Can bringing up pH w/ ascorbic acid instead an option? How about diets that do this?
Hi Joan, Ascorbic acid can raise urine oxalate and will not make urine pH go up. I would not pursue it as a treatment. Regards, Fred Coe
I have just had my 5th ureteroscopy in the last 5 years my doctors cannot seem to prevent them Please Help
Hi Chris, Prevention needs a complete program. Here is a place to start. Let me know, Regards, Fred Coe
Hi Dr. Coe:
I have been reading over your site and have found it very interesting. I have battled with kidney stones for well over twenty-eight years now….my first stone was in my teens. For many years the stones were made of uric acid and a physician finally placed me on 300mg of allopurinol once a day. I have been through countless cystoscopic stone retrievals in the 90’s, and a right nephrectomy when I was twenty-eight due to hydronephrosis due to ureter damage from stent placements and stones. I did well for ten years or so after the nephrectomy, and then I started producing calcium stones. I have had several SWLs, and ureteroscopes over the past few years. I’ve completed 24 hour urine tests over the past several years and found to be hypercalciuria. My medication regime consists of allopurinol 300mg (for over 26 years now), HCTZ (over 10 years), and estradiol 1.5mg (surgical menopause one year after nephrectomy). When my physician put me on the HCTZ he stated I needed to be sure to eat alot of bananas due to the thiazide lowering the potassium levels.
I’m battling yet another stone as I write this. I have added flomax temporarily to help relax the muscle and ureter in hopes it will soon pass; however passing stones has never much worked in my favor. I can certainly produce stones….just can’t eliminate them!
It has now come to the point when I go into my physician’s office he doesn’t even question when I say to him I have another stone (this after having a SWL to fragment a stone only to return two weeks later due to another ….which was removed through a ureteroscope). I have been given the whole lists of foods to avoid, what not to drink, eat, etc….and none of it makes a difference.
Water is my main beverage throughout the day/evening and even when dining out. I carry it wherever I go. I stay clear of sodas, but will have an occasional clear soda or lemonade just to mix things up a little. Tea and Coffee are never even a choice, and I don’t drink alcoholic beverages. I consume very little red meat, and dairy products.
I’m just in my early forties, and having a solitary kidney I am always concerned! I am concerned about the many CTs, along with the many other radiation treatments I’ve received. Aside from being a frequent stone producer I consider myself to be in great health. I’m desperately searching for ways to manage this uncomfortable, painful condition I’ve dealt with for so many years. I have to wonder if my body has possibly become immune to the medication I’m on.
Thank you, I look forward to your suggestions.
Hi Elizabeth, This is a very serious problem and I am sure your physicians are very concerned to prevent stones. If calcium, what kind?? Calcium phosphate, brushite, calcium oxalate? Are they mixed, and in what proportions. How well is your hypercalciuria controlled? Take a look at an approach to prevention and be sure everything is as it should be. If you have active stones, you need to lower the supersaturation(s) relevant to the crystals in your stones. There is no reason for continued stone formation. Regards, Fred Coe
Dr. Coe,
I’m almost embarrassed to say I don’t really know. I’ve only completed two 24 hour urine studies over the last ten years with the latest being done in 2011. Each time these studies were done through Litholink. My annual visit usually consists of just checking a urinalysis. The only time a CT or ultrasound is done is if I go in with problems, and blood tests are not completed unless I’m hospitalized. Despite the medications, I seem to always be actively making stones. My last CT was this time last year when I was in for a stone, and at that time I had three more higher in the kidney which are always left alone. I am so glad I have discovered this site. The information has been so insightful. I will be seeing my physician in a couple weeks, and will be requesting a 24 hour urine as well as blood work. I have to find a way to get to the bottom of this.
Hello Dr. Coe,
I would assume this information is also beneficial for gout sufferers?
I do not suffer from kidney stones (yet) but I do suffer from gout – uric acid crystals that settle for the most part in and around my fingers and more so during winter and cold.
Would citrate therapy help?
Thanks,
Best regards,
Kristof
Hi Krisof, It is not. Gout involves crystallization of sodium hydrogen urate in joint fluid, stones in involve crystallization of uric acid – dihydrogen urate – in urine. Potassium citrate will not make a known measurable change in joint fluid, but will in urine. For gout one proceeds in an entirely different manner. Regards, Fred Coe
Dr, Coe,
I am a 47 yrear old female with 1 solitary kidney. (1 was removed at 10yrs of age) I was diagnosed with cystinuria. Most of my life was stone free until 2015. I had 2 Uteroscopy laser procedures to break up the stones. 1 cystine stone was 18 x 9 mm. I passed literaly hundreds of stones after the surgery. I thought i was doing good. However after a blockage of passing a very large stone. A CT scan showed that my kidney was once again full of stones in less than 1 year. This summer 2016 I had a Percutaneous Nephrolithotomy. It was not a pleasant experience to say the least. I am petrified of getting the stones back again. I am on Hydrochlorothizide 25 mg to produce even more urine flow . Drinking 101 oz of water a day and lowering to the bare minimum of protein. However, I will be seeing a dietician soon. However, I have not been put on Potassium citrate yet. I just dont want to go on Thiola before trying a less radical treatmet.
Hi Lisa, You have a really major problem, and I like some of what you are doing. Massive fluids evenly spaced out over the day is a huge benefit for you. The OHCTZ will not raise urine volume; only water intake can do that. I presume your physician found a high urine calcium level and is trying to reduce it to stave off calcium overgrowth on the cystine stones. Low protein diet can help as can potassium citrate to raise urine pH above 7. But with one kidney and many stones perhaps your physicians would want to add the Thiola sooner than later – if you can take the drug without side effects. Regards, Fred Coe
I submitted a comment earlier this morning but haven’t heard from you.
Hi, Sorry to take so long – Regards, Fred Coe
Would taking Calcium Citrate 200mg with lunch and dinner accomplish the same results as taking potassium citrate?
My last stone analysis showed 70% uric acid and 30% Calcium citrate. That’s something that my doctor recommended but I hesitated taking a Calcium supplement.
Thank you for your great website
Hi James, No. Your stones are mainly uric acid and you need to get the urine pH up above 6 to stop them. WHen you are there get another 24 hour urine and figure out the reasons for the calcium part of your stones. Regards, Fred Coe
Does Magnesium Citrate work for calcium oxalate stone formers?
Hi toolate, There is no known role for it. But the question makes me wonder if you really know what is the best way to prevent your stones. Take a look here and be sure you have checked things out fully. In general, stones are a technical thing – crystal formation follows physical laws – so treatment is very particular. Regards, Fred Coe
well in my case, stones are 90% Calcium Oxalate, 10% phosphate. 24 hour urine showed nothing remarkable.
Adequate intake of water has been a problem!
I like to take Magnesium citrate anyway is why I asked, and I have heard lots of anecdotes from stone formers that Magnesium helped them.
And there are of course studies in the distant past that suggested a role for magnesium
Hi Toolate, There were indeed, but they were of poor quality and generally negative. Regards, Fred Coe
Hi toolate, I guess my only response is to be sure that the urine tests are really normal – were they representative of everyday life, for example. Just check out this small plan for evaluation and be sure. Regards, Fred Coe
I should add: I do not seem to be forming new stones over a 4 year period BUT i do have one remaining stone of 10 mm which i would prefer not to remove surgically and was wondering if shrinking calcium oxalate stones by means of fluids, diet and medications is a possibility?
Hi Toolate, I think dissolving calcium oxalate stones is very unlikely – too insoluble. Regards, Fred Coe
Thank you. Any sense of whether stones that are not causing any symptoms and are relatively stable need intervention? Any trials about this?
Hi, No trials. Stones need to be removed if they cause obstruction, infection, severe pain, or bleeding. Otherwise the problems of surgery are not justified. Regards, Fred Coe
Thank you for that opinion! But isnt the risk of the various procedures increased if one waits for infection or obstruction?
Hi toolate, It is not an opinion but a generalization. If the stone is not obstructing, and pain, infection, and bleeding are not present – your physician needs to assure this – removal is not known to benefit patients in the long term. Your physician may offer surgery because of the details of the stone position or your kidney anatomy. Regards, Fred Coe
Once again thank you for your kind and thoughtful reply!
As a long time patient of your clinic at University of Chicago, I have spent much time researching this disease. I’m so greatful for the advances made in treating this disease. I have calcium phosphate stones. I also suffer with Lupus and Primary Immune Deficiency. I wonder if either of those diseases have caused my gravel pits known as kidneys. I’ve had at least 10 lithotripsies (I lost count), and currently have 5 and 6mm stones along with many 2mm stones in each kidney. I take 25mg of Chlorthalidone daily. This drug has greatly reduced my stone formation, but also my potassium levels. It was impossible with potassium cholride alone to get it in the normal range. I take Amiloride 10 mg 2x a day and 60 meq Potassium Chloride. This keeps my level around 3.5. I strive for a low phosphate – low sodium diet, along with at least 2.5 liters fluid a day. Thanks to Dr. John Asplin and then Dr. Anna Zisman for their great care and guidance – I’m doing well. I’m fortunate to live within 2 hours of the clinic. I have not been there in several years as I see a local Urologist, Dr. Brian Keuer and a Nephrologist, Dr. Donald Cronin, for my care. Both my fine doctors have stressed increasing citrates as you have in your published articles. My urine ph level is quite high, Dr. Zisman believes the reason is too many lithotripsies. My question is: what ph level should be strived for with calcium phosphate stones?
p.s. I’d be happy to be included in a study as you stated not many have been done for my type of stones.
Hi Laurel, Dr Zisman is my partner, and she should answer this. I am sure she mentioned that immune disorders can cause renal tubular acidosis with high urine pH and calcium phosphate stones. I am sure your local physicians are excellent. If there are any problems, we are here to help. Presently we are not doing a study related to your stone type but thank you for the offer. Regards, Fred Coe
My diagnoses of Lupus and Primary Immune Deficiency came after my last appointment with Dr. Zisman, although my symptoms all existed. This is the first I have heard of renal tubular acidosis, it sure answers my question – why am I a stone former. I will make an appointment with Dr. Zisman to follow-up on this important issue. Thank you very much!
Hi, Laurel, I only made a suggestion. But Dr Zisman is very skilled and if your immune disorders have caused RTA she will certainly be able to help. Regards, Fred Coe
Dear Dr. Coe – How much of your advice applies to bladder calcium oxalate stone formers? I have had three procedures in the last four years to remove them. I have BPH but very low residual after voiding. This had led my current urologist to think the cause is metabolic rather than BPH-caused obstruction. I’ve had a 24 hour test which showed 1.8 liters and high oxalate. Treatment now consists of increasing my water intake to eight 8 oz. glasses of water daily and eliminating high oxalate foods. Does this seem reasonable to you? Many thanks in advance for your advice and work.
Hi Jim, Your doctor may be right. The way to proceed is not to add fluids and fool around with oxalate. Get things evaluated the right way and treat what is abnormal. Try this plan and see if it works for you. Regards, Fred Coe
“The way to proceed is not to add fluids and fool around with oxalate.” Is this correct? Did you mean now instead of not?
Hi Jim, Thanks. I cannot find this phrase in the citrate article. Can you point to it? I read the article through 3 times and seem to have missed it. Regards, Fred
It’s your second sentence in your initial response to my question.
Hi Jim, Yes I meant ‘not’ because of what follows – you need to get a complete evaluation to determine what to do and not try things that have been proposed for stones. Empirical treatment without chemistries is not efficient and will not in the long run work well. I pointed you to a good article with a decent sequence to follow. Regards, Fred Coe
The treatment plan to increase fluid and decrease oxalate was based on a 24 hour collection and analysis with the following results: volume 1.8; SS CaOx 6.19; calcium 111; oxalate 49; citrate 714; SS CaP .43; ph 5.809; SS Uric Acid .92; and Uric Acid (g/day) .578. The volume, SS CaOx and oxalate measurements stood out. Is there another test I should be taking? My urologist’s plan is to have an ultrasound test in March to see if bladder stones have formed. I greatly appreciate your willingness to respond to questions from the great expanse of the internet. Jim
Hi Jim, A reasonable plan. Be sure you are getting the full 1,000 to 1,200 mg of diet calcium; taken with main meals high calcium foods block oxalate absorption and make the diet issues a lot easier. The calcium also protects your bones.
In 2013 I was diagnosed with a renal oncocytoma and 1.7 centimeter stone. A blockage, a stent and a lithotripsy followed. After a 2nd lithotripsy, another blockage and then a 3rd lithotripsy, I was found to have just a few very small stones. I followed a low oxalate diet for nearly a year and asked my urologist about Theralith. I passed the fragments and have been stone free since March of 2014. I also have gout, but haven’t had a flare till this summer. My urologist told me to add foods back into my diet and drink at
least a gallon of fluid daily and make part of that lemonade. Just wanted your opinion. Thanks for your time!
Charlene
Hi Charlene, Thanks for sharing your experience. Theralith is a low dose formulation of magnesium potassium citrate. This agent was tried on one trial but with higher amounts than I suspect you used with this product. Of importance, you did not say what your stones were made of. Given gout, perhaps they are uric acid. Regards, Fred Coe
Hello again.
Since beginning of Septeber, I am measuring my urine pH each time. What makes me curious is the fact that in the morning pH is very low – and despite citrate load (10 mEq + 0.5 dm3 of water and 6 am and 8 am ) it stays below 6.0. After first meal (~12am) it rises to ~6.5. Previously, when I was eating a small breakfast (+ 10 mEq Kcit) at 6am, it was always about 6.5. However, if I don’t eat much protein meals, then pH falls @ 5-6pm (another doses of Kcit @ 2,4 and 6pm) to 5.8-6.0…
If I eat a high protein meal ~5 pm , then pH skyrockets to 7.2-7.4 about 2-3 hours after (even if I stop citrate) and stays there for a few hours , to my last visit in WC before sleep. If I eat heavy meal before sleep (bad idea, I know) – then even in the morning pH is above 7…
So, for now, since I cant consult my doctor…I am trying to go for low amount of food distributed through all day and that works… but I never suspected our meals influence urinary pH so heavily.
Regards
Luke
Hi Luke, you are a good scientist. Yes, meals raise urine pH – well known, and you have accurately observed it. For uric acid stones I would not be too fussy, it is the 24 hour urine pH average that counts, so just use enough potassium citrate or other alkali sources to get it above 6. Regards, Fred Coe
Many thanks for reassuring me that the increased water/increased calcium/low oxalate regimen I’m on makes sense. It means a lot to know that it is likely doing some good since I’ve had to significantly change drinking and eating habits Thanks again for generously sharing your knowledge and time.
Dr. Coe,
Thank you for your continuing efforts to help with identifying the causes of renal calculi and minimize kidney stone formation. I began following your recommendations last summer and finally saw a reduction in my stones! Now? I am struggling with a compromised medication that caused my stones to return. Long story I won’t bore you with, but, I am at least sure the regiment you recommend is effective. It is difficult for me as I had been on a diabetic diet and so many of the foods I had learned to love are high in oxalate. I’m adjusting my diet, again, as the stones are a much greater risk to my health than a slightly elevated A1C. I will see my nephrologist soon and ask about a Rx for Urocit K. I’m hoping that will further reduce my stones.
Dear Dr. Coe, many thanks for a wealth of information. Potassium citrate is mentioned frequently, would magnesium citrate also suffice?
Hi Rasmus, I do not think so. It is poorly absorbed and can cause diarrhea. Regards, Fred Coe
I have suffered from calcium oxalate stones since 2002. Today, my kidneys have 20+ stones each, as shown on an ultrasound performed twice/year by my urologist.
I drink 10 glasses of water/day and watch my diet, but for some reason am not preventing the formation of new stones. Every few months, I suffer from a UTI and have stone-like symptoms.
Do you suggest I take potassium citrate to prevent the formation of future calcium oxalate stones? Thank you.
Natalie
Hi Natalie, A lot of confusion and trouble can occur with so many stones in the kidneys. This article sums up a lot of what I know. This one helps be sure everything has been done right. It is not so much any one medication as it is the ensemble of proper diet and meds as needed. Regards, Fred Coe
Hi Dr. Coe,
Once I’m on a balanced diet and medication regiment, about how soon might I finally see a reduction in the frequency and duration of my kidney stones? I’m getting so very discouraged. It limits my life so much! My endocrinologist and nephrologist and I tweak medication and their dosing, but it just never seems to get better. Thank yoU!
Hi Lisa, I guess the question is the most important one. Do you know the crystals in the stones you are forming? If so, find out the urine supersaturations for those crystals- your physicians know all this. What was the supersaturation for those stone crystals before diet and medications were instituted? What is it now? If it really fell a lot, are you sure there are new stones or passage of old stones – your physicians know this. If there are really more new stones, be sure you know their crystals. If the same ones as in the past, the supersaturations may have fallen but are not low enough: Lower them more. Be sure the 24 hour urines you give your physicians represent your real life, work and leisure. Supersaturation is all crystals can know about, so low enough and stones must stop. Regards, Fred Coe
Sir i had a stone analysis of stone i think it is a uric acid stone but base on the stone analysis their a presence of oxalate. and i thought it might be uric acid oxalate stone and just to make the record all clear this is the stone analysis : texture=hard oxalate=positive, ammonium=positive magnesium=positive and uric acid=positive. It would be a big help if for me.
Hi Juvanniel, It sounds like a mixed stone with both calcium oxalate and uric acid in it. This is not rare. The presence of ammonium suggests that struvite might be present. However, chemical analysis of stones is not a very reliable method. I would aim at the calcium oxalate and uric acid. Here is an approach you might find useful. Regards, Fred Coe
god day doc fred
Actually im only a highschooler conducting a study about kidney stone. As you said to me the stone might be a combination of uric acid stone and calcium oxalate stone. But in the stone analysis their is a absence of calcium. but base on the teacher that gave me the kidney stone it is a calcium oxalate stone his doctor said but the certification was missing. And so i conducted the stone analysis. And in my shock calcium is negative on the stone analysis.
Hi, As I said, chemical testing of stones is a poor method with variable and medically useless results. There is no doubt calcium as measurable oxalate without crystals would be impossible for you to detect. The most reliable technique is infrared spectroscopy, which would not be usable for a classroom. If your school had a polarizing microscope you could polish an end of the stone and get the polarization angles of the crystals which would help identify the crystals. Uric acid in stones is usually crystalline dihydrogen urate; calcium is either present as calcium oxalate mono or dihydrate, or calcium phosphate – you did not appear to find phosphate. Oxalate will always be in calcium oxalate crystals. Urine has oxalate to only about 0.1 mmol/liter, but in calcium oxalate stones it is locally concentrated so you can detect it. As for the calcium, you missed it – try again. It is a very good lab exercise, good for your teacher, and you. Best wishes, Fred Coe
God day Doc fred
To be true Im not the one that conducted the stone analysis it was conducted at cebu doctors hospital. And the result shows their is a absence of calcium thats the mean reason why im worried. And so i can up with this question. Can i name the stone uric acid oxalate stone. or uric acid stone? Your replies is much appreciated and im so soory for the inconvenients.
Hi If there was oxalate there is calcium. Chemical analysis is just too poor for real use. If this is just a school experiment you need to name the stone for what it is – has uric acid in it and is unsatisfactory in analysis having oxalate without calcium. If this is about a real person, the results cannot be used at all. Regards, Fred Coe
Sir,
I have been having uric stones on my left kidney repeatedly (I was an ulcerative colitis patient for 25 years). A few passed (up to 6,5mm) but then in 2012 I was operated to remove by incision and laser two stones (1,5cm and 2 cm each). One a an half year later, two more uric acid stones were formed (1,9cm & 1,7 cm). I started therapy with sodium bicarbonate (1,5 g per day) and a pH meter. Three years later my two stones were reduced to 1,7 & 0,7cm respectively (always measured with the same ultrasound machine and the same radiologist), so I was optimist about dissolving them completely. However, 6 months ago I had a permanent ileostomy. Following this I had difficulty maintaining urine pH around 7 as before with 1,5g of sod. bicarb per day. Now I require 8grams of sodium bicarbonate per day to keep urine pH around 6 to 6,5. A week ago I measured the stones again by ultrasound and to my dismay they grew by 2mm each. Should I switch to potassium citrate to have better results and try to stop stone growth and achieve further shrinkage (I do not want to further increase the dosage of sod bicarb and I would like to avoid another operation) ?
Best regards
Kostas Phytas
Quebec City, Canada
Hi Kostas, You have a real problem in that ileostomy fluid is high in alkali, essentially a loss of sodium bicarbonate. Usually sodium alkali is ideal because ileostomy fluid is sodium rich whereas potassium alkali is irritating to the bowel and often not absorbed well. You have little risk of sodium excess. I would be sure to spread out the sodium bicarbonate during the day and even night especially to match ileostomy flow as periods of low urine pH can produce marked growth. You could add 20 or 30 mEq of potassium citrate to the sodium bicarbonate if you wish, of course, especially if your serum potassium falls, but that rarely occurs. With time ileostomy flows tend to moderate. But aside from pH, sodium and water depletion will tend to lower urine volume and that is a very common reason for stone growth. If you cannot maintain urine volume with plain fluids, use beverages with sugar because sugar absorption will promote water absorption in the jejunum. The sugar should be glucose. Regards, Fred Coe
Thank you very much Fredrik for your helpful comments. I really appreciate your help.
Sometimes, I am wondering if I should aim at a urine pH of 7 or even higher (7,8). I found out that on internet (http://emedicine.medscape.com/article/983759-treatment) that …Sodium urate is 15 times more soluble than uric acid. At a urine pH level of 6.8, 10 times as much sodium urate as uric acid is present. At a urine pH level of 7.8, 100 times as much urate as uric acid is present….do you agree?
Thanks a million
Kostas
Hi Kostas, For uric acid stones, one wants a pH around 6 – 6.5 because the pKa for dihydrogen urate – the uric acid that crystallized into stones – is 5.35. Higher pH levels can promote crystallization of calcium phosphate salts, and lead to mixed stones. At pH 6 to 6.5 the concentrations of dihydrogen urate are so low higher pH will be essentially useless. Regards, Fred Coe
Thank you very much Fredrik, I appreciate a lot your advice
Best regards, Kostas
Hello Fredrik, I keep my uric acid stones under control by taking 8-9g of sodium bicarbonate daily and monitoring urine pH around 6,5. I observe through regular ultrasound a slow dissolution of my stones (a couple mm per year) and I am quite happy although my permanent ileostomy is a challenge. Do you have any idea of how to avoid stomach irritation with so much sodium bicarbonate (I take in pills of 0,5g)
I did notice that sometimes my stomach gets irritated especially if I get sod. bic. diluted in a glass of water. Thank you very much Kostas Phytas
Hi Kostas, Sodium alkali is ideal for ileostomy, and you have chosen well. Be sure your blood pressure is not high – sodium loads can worsen that. I would use the pills with food to reduce gastric irritation. Regards, Fred Coe
Thank you so much, Fredrik. Your advice is precious to me. You are the only one who can understand my approach and I see slow results (stone dissolution). Classic approach by urologists is operation by laser which I did once but one year after I ended up with exactly the same stones in my left kidney (which is a mystery to me why only in the left one). Then another urologist told me that each laser destruction and stone removal results in a 5% decrease in kidney’s function. Best regards Kostas
I had lithotripsy in August 2016 for a large (2cm) stone and still passed gravel in October. On November 22, I had an ultrasound and my urologist said that I was not actively trying to pass stones and my kidneys looked clear (although she said ultrasound is not reliable for that). She prescribed potassium citrate since my stone was 80% uric acid and my 24 hour urine showed low volume and low pH. I also started drinking Crystal Light after reading your articles. On December 2 I started having symptoms similar to when I had a stent – constant urge to urinate with urgency. No UTI. Could I have developed new stones that quickly? Also, on December 4, I started having diarrhea and I am afraid I might not be able to tolerate the potassium citrate. Will water alone dissolve uric acid stones? Is there any other remedy for the OAB like symptoms that are maddening?
Hi Peggy, It is possible that you made a new tiny uric acid stone or passed a fragment from an old one. Get your urologist to check as it could be at the junction of the ureter and bladder – there is always the possibility of kidney obstruction, and that cannot be left alone. Water is not enough. If potassium citrate is hard to use Crystal light can be your main treatment and perhaps a smaller amount of what you need from the k citrate pills. WHat you need is enough alkali to raise urine pH above 6, and 24 hour testing the most reliable guide. Regards, Fred Coe
Thank you for such a quick reply. What test is best to check if a small stone is at the junction of the ureter and bladder? My physician mentioned a Ct scan but I had 4 of them while hospitalized three times in the last 2 months. Should I worry about exposure?
Hi Peggy, Here is a problem. It all depends on the details of your immediate symptoms and those are hard to evaluate – medicine is a lot like auto repair: You need to hear the motor running, or listen to the squeaky sound itself. So leave this to your urologist. Low dose modern CT scanners are much lower in radiation hazard. Ultrasound could rule out obstruction – good at that – and if there is no obstruction one can wait if you can stand the symptom. Use your physician here. Regards, Fred Coe
Hi, My stone analysis show that i am positive for Calcium carbonate, 33% calicum Oxalate and 40% Calcium Phosphate, with such, what is your best recommended treatment? Thanks
regards,
Chris
Hi Christopher, Given 33% CaOx and 40$ CaP the calcium carbonate would have been 27% making your stone predominantly CaP/CaCO3. I doubt the calcium carbonate part of the analysis and suspect is is highly carbonated apatite, but that is speculation. So, from the one stone, you appear to be a calcium phosphate stone former. You should pursue a complete evaluation to exclude systemic diseases as a cause and get 24 hour urine testing. Assuming no systemic diseases you would be like other calcium phosphate stone formers. Overall treatment would look like this. Regards, Fred Coe
Dr. Coe
Which type/form of calcium supplement is recommended to prevent future calcium oxilate stones?
Thank you
Hi David, For everyone diet calcium should be 1000 to 1200 mg, preferably from foods. Supplements are merely a workaround when foods will not do. If needed they must be taken with larger meals. Warm Regards, Fred Coe
Dr. Coe
I’ve had 3 trips to the ER in the last 15 yrs for calcium oxilate stones. I’m 67 yrs old and really don’t want another stone. I’m hoping you can recommend which type of calcium supplement and dosage to take (calcium citrate or calcium carbonate, or? )
Thank you
Hi David, Three stones is 3 too many. I can indeed recommend for you, but it is to get a full evaluation of causes. You cannot prevent stones without knowing what is wrong. As a general fact, a 1,200 mg calcium diet is ideal for more or less everyone, but for stone formers it is generally important to also lower diet sodium to about 1500 to keep urine calcium low. But I would get proper testing before making such changes. Regards, Fred Coe
Hello Doctor,
Firstly Thank you for this Awesome informations..
I had two 3 mm stone nearly 5 years ago – unfortunately I had not done the Stone analysis then.
– (It was very hard – dark brown stone passed via Urine) – not sure what type of Stone is this..
But now I have a 8mm stone.. and in Plain CT nothing was shown, so I had to do a IV contrast
– It is just above the VUJ. – causing mild ureterohydronephrosis.
– No Plain – Never had a plain till now..
– Urine smells likes ammonia often
– Ecoli was found with UTI issue
Even after taking Norflox drug, i keep getting UTI regularly..
– My Doctors are surprised to hear that I never had pain (not even a bit)
– Is there is a way to tell what type of stone it is?
– Could this be a Uric Stone? because it was not shown in plain CT scan..
– I’m Also worry that my kidney might get damaged because of this
(I’m mean I am having no pain)
– nearly two months now on heavy fluid intake
or is there is a way to know the type of stone
Kindly assist..
Sam
Hi Sam, the strong ammonia smell suggest infection with bacteria that can hydrolyse urea to ammonia. They can actually produce stone crystals – struvite. After 2 months of obstruction is it not time to have the stone removed?? It may be uric acid, it may be struvite, whatever have it analysed when it is removed. Regards, Fred Coe
Thank you Very much Doctor for your reply…
– I rely can’t explain why there is no Plain..
– Will these stone grow in Ureter?
– Since I had a hard stone (looked like a Calcium stone) earlier – Doctor thinks it could Oxalate..
But Since uric acid is soft, I thought I’d wait for it pass
But In heavy Dilamma
I mean
– I rely can’t explain why there is no Pain..
Hi Sam, Uric acid is not soft. Discuss with your physician about when to remove the thing. Regards, Fred Coe
I was searching through your article Associate in Nursingd wished to understand if there was one thing you may advocate as an ‘over the counter’ pill on the market I will soak up role of overwhelming straight pure juice. that’s the program my current medical specialist has American state on for my urinary organ stones. one cup of contemporary squeezed juice daily. to this point it’s worked however it’s therefore expensive and long to squeeze the lemons daily for this. I conjointly travel plenty for work that makes it particularly tough to stay up the plan. If there was a pill type of acid on the market that was as effective that may be a lifesaver. Any suggestions? Thanks for your help!!
Hi, I do not have your name as you seem to come from the above website which depicts treatments and remedies. I gather your issue is whether a pill can substitute for squeezing lemons. Yes, if you have kidney stones and need potassium citrate one can get it from lemons, and yes that is cumbersome and not even that cheap. The pills that will substitute easily require medical prescription. My problem with answering you more fully is that you give no real information, and therefore I cannot very well give you a real answer. Regards, Fred coe
I suffer from calcium oxalate stones, and when I’m in pain from them I look up various science breakthroughs related to kidney stones, because it’s hard to believe a medical condition that happens to so many people only has prevention, palliatives, and removal as options. With that said:
There’s a nanomedicine approach published in Biochim Biophys Acta that is theoretical, researchers analyzed the nanostructure of stones and came up with a potential gold-nanoparticle that may show promise in fracturing the stone at nanoscale. I realize that this isn’t a feasible short term solution.
Also, I’ve heard about the new HCA breakthrough published in Nature by materials engineer Jeffrey Rimer, et al. Hydroxycitrate apparently can dissolve the stones in real time in lab settings.
My question is I was wondering if you were aware of this research and had any recommendations regarding it? HCA is easily available online, for instance.
Hi Matt, The gold nanoparticles are indeed far from medical practice. The HCA breakthrough authors include my colleague John Asplin so I certainly know all about it. A trial is important and not done. The material is in health foods sans prescription needs. Stone prevention is odd in that crystals obey physical laws to reduction of supersaturations must lead to prevention; the problems are all practical issues in lowering said supersaturation. So prevention can be had at varying degrees of personal annoyance and practical difficulty. I hope some day for more efficient means – perhaps crystal doping agents like HCA. REgards, Fred Coe
Thanks for your swift response and all the information your website provides,
“A trial is important and not done.” – Does this mean there is a trial, but it is not complete, or that there is currently no trial for HCA being attempted at this time? If so what are the barriers for attempting an in vivo study (money, safety, lack of interest, etc)?
Hi Matt, I really do not know; probably the matter is being discussed with the interested parties. Since the material is available widely, safety is not a main issue. Sorry I have no more to offer. Regards, Fred Coe
Update: After a year of searching I’ve finally found a clinical trial of HCA in humans to study urine chemistry in control subjects vs. calcium oxalate stone formers; set to begin on Dec 2017 and set to conclude on Dec 2018. The aforementioned study is NCT03348228 and being done by the University of New York. The enrollment period is over, but I look forward to the results.
Dr. Coe – I found this article and the comments and replies very interesting. I had kidney stones as a teenager in 1967. I did not have them again until March of 2015. I had laser lithotripsy and the stone was analyzed as 80% uric acid and 20% calcium Oxalate. I had blood work and a 24-hour urine test and was told my calcium and uric acid levels were normal but I was slightly dehydrated and was low in cituric acid. I left with orders to drink more water and drink lemonade. I have done that since then.
I saw the doctor for a regular check-up in last month. The doctor was happy that I had lost 50 pounds in the past year and had given up drinking all soda replacing it with water and lemonade. The doctor ordered an ultrasound because of routine blood work that indicated my kidney function was a little off. On the drive home after the ultrasound I had another kidney stone attack. I passed a small cluster of stones but I again had laser lithotripsy to remove a 1.8cm stone. The doctor said he found hundreds of tiny stones in my kidney. The stone again tested as a combination of uric acid and calcium oxalate. He said he cannot prescribe medication or diet until I have an ultrasound to make sure the kidney has healed from the surgery and then blood work and another 24-hour urine test.
I am concern is that my levels will be normal again and that I will be told to drink more water and lemonade and sent on my way again. Knowing I still have a large number of tiny stone in me, what can I do to keep them from clustering and forming larger stones? I am fearful that another attack can happen at any time. We have two major trips planned, one of them out of the country, and I am so afraid of having an attack while away. The doctor said that I can plan the trips but I am anxious about this. Any suggestions you can give will be appreciated.
Hi Kate, Your stones are predominantly uric acid and that phase arises when urine is too acidic – pH is below 5.3. Low urine pH occurs in obesity, metabolic syndrome – high blood pressure, abnormal blood lipids etc – and diabetes or the precursor to diabetes: Insulin dependence. I suspect your early life stones were calcium from genetic hypercalciuria and your later stones from what I said. Soda is a risk factor if containing sugar or high fructose corn syrup. Dehydration is always an issue. For the uric acid you need potassium citrate in a full dose and your physician can easily provide it. Of course he/she knows that total urine uric acid has nothing whatever to do with uric acid stones. Take a look at your own lab report. Smaller uric acid stones may dissolve, larger ones will probably not. Urological management is obviously in the hands of your surgeon. Prevention of uric acid stones is invariably perfect as all it takes is potassium citrate in adequate dose – the uric acid crystals cannot survive in urine of average pH above 6.3. Regards, Fred Coe
Thank you so much for your reply.
I am hoping that the doctor will prescribe potassium citrate this time. He said he will not prescribe anything until all of the testing is complete which will not be until mid to late March. I am anxious to start doing something to help keep the tiny stones I still have from getting larger or clustering together. I appreciate your comments. Thank you so much.
Dear Dr. Coe,
We are based in the Netherlands. We have a 14 year old daughter, diagnosed hyperoxaluria after stone removal (55% calcium-oxalate-monohydrate, 45% calcium-oxalate-dihydrate). Attention was focused to existence of primary hyperoxaluria Type I and investigation was carried out on DNA analysis for confirmation. DNA analysis concluded no marker and subsequently it could be somewhere in the DNA but not known to scientists at this moment. Primary focus was to increase alkalinity by administering potassium citrate 6000 mg. Dosis was initially far too high: due to severe muscle fatigue. Dosis lowered to 3000 mg/day. Urine pH levels average: 6. Which is sufficient to prevent stone formation. She has been on the pills for four months and the nephrologist advised (after finding out that no DNA markers present) to stop all medication and get her back to a ‘zero level’. In other words she will form new stones and they want to see if this does happen. They told us not to be worried and not to measure her urine pH levels, as this would upset too much. Of course we are very concerned with this approach and have also noticed, that our daughter has a low saturation (sometimes below 85; should be round 99%). (This is the reason for contacting you for some alternative advice.)
Blood investigation, after recently stopping potassium citrate, showed after three weeks that the potassium citrate levels: 5.5 mmol/l potassium. After four weeks: 4.5 mmol/l. So potassium is gradually being cleared. We have also read, that too much potassium could affect the heart and are worried, that if we would want to continue on the potassium citrate, that too much potassium would not be good for her. Muscle fatigue, saturation problems?
We have been reading about magnesium citrate or a combination of magnesium/potassium citrate could be beneficial. We would rather not have her on potassium citrate but an alternative for potassium like magnesium would help. What are your experiences? What about sodium bicarbonate? I read that this would help alkalinize, but am concerned it would also higher the pH in the stomach and thus prevent the beneficial working of the pH there for killing bacteria etc.
What about the pico-ionic magnesium(gets absorbed better by the intestine and does not have an GI effect associated with normal magnesium pills taken?
Thank you for your time and answer in advance.
Kind regards,
Philip
one more concern: her PH level in her urine is currently below 4!
Hi Philip, You do not say but I infer the levels of oxalate in the urine connote a primary form of hyperoxaluria. That is a dangerous disease that can produce kidney failure. Drugs like potassium citrate are not a problem but also a weak defense against kidney damage. I presume you are at a university center that has expertise in this condition; if not such expertise is an absolute necessity. That her blood potassium varied with the dose of potassium citrate probably means the bloods were taken after the drug because normal kidneys will clear potassium promptly enough serum potassium hardly changes. My sole advice is to get her care from physicians – these will always be at research centers – expert in this condition. The best world resource is the rare disease consortium at Mayo Clinic. The director is Dr John Liese who was once my protege and now world famous for his work on these rare conditions. Probably the center or Dr Lieske can be sure about the right physician for your daughter. Regards, Fred Coe
Dear Dr. Coe,
I am desperately seeking advice to help my son, Ian.
Ian forms 3-6 kidney stones each month. That is not a typo, each month.
He is in constant irretractable agony 24/7. The doctors dismiss him as dramatic and one accused him of picking his finger to put blood in his urine. This accusation was made even as he had the CT results in his hands. How do you fake a CT scan. After that encounter,
I found that my son has researched suicide online.
My son has been in constant pain for over a year and the doctors, petrified by the DEA, refuse to use proper pain medicine. Until a cure is found what can I do to help him?
Hi Eva, The issue here is stone prevention. Three stones monthly is over 30 in a year, which is very active. You do not say what they are composed of, but begin there by having many analyzed. Here is a good plan for prevention, and what you can do for him is get him through this plan to a final prevention plan. Pain medication is nothing but a brief stopgap, prevention is the key. If your son has researched suicide on the web there is possible danger; his physicians need to know that and you need to consult with proper professionals about how best to keep him safe. Regards, Fred Coe
Eva,
I know this is going to sound crazy as it is a folk remedy but has he tried apple cider vinegar? It seems to work for me. It does contain citric acid and helps increase PH in blood and urine. There are lots of recipes online for a drink with the vinegar but I just fill a shot glass in the morning and at night with the vinegar and then drink a big glass of water after. I can see the gravel in my urine so I know they are dissolving. I know many people here will disagree because folk remedies and old wives tales are not science but I know for myself it works. It is worth a try at least to alleviate some of his pain if it can at least shrink the stones a little. It can’t hurt to try it. I hope he feels better soon and it is hard to find a doctor that will listen these days but I hope you find one.
i will be 60 in a month, have recently since july of 2016 gotten kidney stones, it woke me up 1 night but got progressively worse throughout the day, and 13 hours later i was in a lot of pain and thought it was my appendix, i went to the hospital, they scanned my told me i had kidney stones, my creatnin levels are high, i dont know if that has anything to do with it, but recently had them anylized, and found out today they are uric acid hidrate stones, how can i prevent these from forming, i was using real lemon juice and water to ‘shrink’ them to pass easier but is this a remedy whatsoever, i do not want to get them again, if possible, and any info in prevention, like my diet of daily eats,and natural remedies instead of drugs is a huge help to me, thank you
Hi Tom, Uric acid stones occur only because urine is too acidic and are cured by raising the urine pH with alkali. THe lemon juice is nonsense – probably too little alkali, variable effects. You need reliable alkalinization and that is usually 20 mEq of potassium citrate 2 – 3 times a day. Your physician needs to make appropriate precautions about the potassium loading. You need proper 24 hour urine testing and followup testing after going on treatment. Diet will not reliably work and the stones can form rapidly and become large, so just stop them. Regards, Fred Coe
Dr. Coe, I had an attack of kidney stones last November in the early morning. Only time this has ever happened, actually thought I may be dieing . Trip to ER revealed mulitple stones in both kidneys all <4mm. To my knowledge I never passed a stone. I strained urine for three weeks and never saw any sign of a stone. Followup with Dr. gave little advice except to drink lots of water, some "flowmax", and bring in stone if i catch it. No problems since but situation is scary. Have given up tea and trying to cut out salt. Any other advice would be appreciated. Thanks.
Hi Ricky, Prevention is very important for you given so many stones in the kidneys. Here is a good summary about a plan you can follow. There is no sense in diet changes, these have to be made in the light of a proper evaluation. Take a look. Regards, Fred Coe