 A new video about how science works
A new video about how science works
What is it About?
All we know about kidney stones arose at one time or another from scientific research. The same for everything on this site. Beyond the borders of stone disease, one might say this for all of physical modernity.
No surprises here.
Do the incomparable successes of science not cause at least some of us, sometimes, to wonder about how science works? I do not mean pictures of remarkable instruments, or the gorgeous star scapes from NASA. I mean the mundane if productive lives of normal scientists doing their work – how much of what we have came to be; my own life in science, surely.
Apart from stone disease, my other life has been as a teacher of science. This site has a whole section with my thoughts about the matter going back years now. Teaching has a way about it. Your thoughts have to evolve as you encounter successive students and produce successive lectures. This past few years mine have, to the point where I decided to gather them into a video for this site.
The video contains my current views about how science, especially clinical science works.
The video is not easy, and it is long. People will decide if it is worth their time and energy.
It was for me.
What is Specially Interesting in the Video?
The purpose of a research – its objective.
For example an ongoing trial seeks to improve water intake in stone formers as a means to prevention.
Fluids are Obviously of Value
Fluids dilute the urine and dilution will reduce crystal formation, so fluids are certainly part of stone prevention. Few patients doubt this, but not all drink enough.
By ‘enough’, what does one mean? In our one trial of water alone, about 100 patients with very low urine volumes (mean about 1 liter/d) were randomized into nurse prompted high fluids (urine volume about 2.6 l/d of urine) or told to stay hydrated (mean volume around 1 l/d of urine). After five years, new stones occurred in 12% of the high fluid group and 27% of the low fluid group.
In our best risk factor style study, Curhan found that risk of new stone onset rose mainly below 1.25 l/d of urine volume, consistent with the trial.
So ‘enough’ must mean somewhere between 1.25 and 2.6 l/d of urine volume, certainly closer to the latter than the former. Since 12% of even the high fluid group formed another stone, and the population of the trial was exclusively first time stone formers, very high fluids alone is not an ideal treatment. But it did lower new stone formation, so it is of some worth.
Does this mean that ‘enough’ must indeed be 2.6 l/d?
That is a burdensome amount.
Is that goal also true if one uses all we know about diet and even medications to prevent stones? In other stone prevention trials (in the linked article) of medications and diet, urine volumes were about 2.2 l/d, a lot less burdensome.
What Does the New Trial Seek as its Objective?
“Rationale & objective: Although maintaining high fluid intake is an effective low-risk intervention for the secondary prevention of urinary stone disease, many patients with stones do not increase their fluid intake.” (copied from the trial)
The objective – what is desired as new knowledge: What is it? One must presume it is something to get patients to increase fluid intake more uniformly than they presently appear to do.
If the objective of a research program is a ‘thing’, some thing that will benefit patients, then this is some kind of thing to raise fluid intake more than just advice from physicians.
I have no quarrel with this public facing form of the objective. One can simply say one seeks a ‘thing’ (method, machine, medication) to increase fluid intake in stone forming people. This is in the form of invention, which my video clarifies logically and realistically as an imagined solution to an evident need. An imagined ‘thing’ which can be produced or extracted from the real world and tested the way one might test an improved refrigerator, or rocket ship, or antibiotic made by an exotic soil fungus.
What Is the Imagined Thing?
“Interventions: All participants receive usual care and a smart water bottle with smartphone application. Participants in the intervention arm receive a fluid intake prescription and an adaptive program of behavioral interventions, including financial incentives, structured problem solving, and other automated adherence interventions. Control arm participants receive guideline-based fluid instructions.”
The group that does not get the new ‘thing’ gets 1) “a smart water bottle with smartphone application” and 2) “guideline-based fluid instructions”.
The ones that get the ‘thing’ get 1) “a smart water bottle with smartphone application” and 2) “a fluid intake prescription”, and 3) “an adaptive program of behavioral interventions, including financial incentives, structured problem solving, and other automated adherence interventions.”
Given the ‘thing’ is the difference between the groups, the ‘thing’ is ” behavioral interventions, including financial incentives, structured problem solving, and other automated adherence interventions”. That is the objective of the trial, testing the value of the thing against not having the thing.
The Two Sides of an Objective
This trial illustrates one of the most important issues in clinical research. The significance of an objective arises from its utility: its benefits to certain people, in certain ways, and to a certain extent. Surely a thing that will maintain fluids would be a significant objective.
The problem is imagining a version of the ‘thing’ that can be tested. One form of testing, if it is not something we will make to use, is if the imagined ‘thing’ makes predictions one can test in an experiment. This is how we make progress concerning how nature does things – like cause some people to produce kidney stones. The other is if the ‘thing’ is something we can use. We make the ‘thing’ and try it our (do a trial) to see how well it works.
The illustration I have chosen is an invention, a mix of financial incentives, structured problem solving, and automated adherence interventions.
Imagination works precisely between the public facing objective (a way to enhance fluid intake) and the imagined form of the thing (“behavioral interventions, including financial incentives, structured problem solving, and other automated adherence interventions”.) Presumably, if the thing is better than no thing a way will be found to use financial incentives, structured problem solving and automated adherence interventions in a mass market and practical manner without the financial support of an NIH grant.
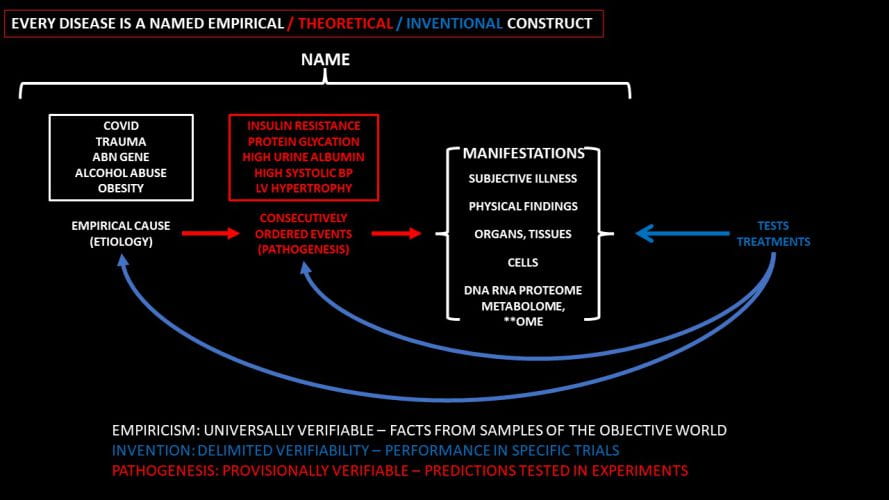
The Video Presents the Entire Logic of Clinical Research
The video shows the entire structure of a research program of which my example is a limited instance. There are multiple ways to progress from the public facing to the experimental face of an objective. The hypothesis, an often poorly understood combine of the experimental objective and the actions needed to achieve it, is much clarified. The logical connections between imagination and measurement, which I illustrated in the trial, is a far more interesting topic that the video speaks to. Finally, we have in my illustration here only one kind of objective – an invention. But there are two others – empirical research, and theoretical research the video presents in detail.
Who Would Want to Know?
I would think everybody.
The engine of science creates the whole of clinical medicine – tests and treatments, and understanding of diseases. Patients have a huge stake, and physicians likewise. The video gives one intellectual tools to extract out of the wordy rubble of research proposals, science articles, and medical news the real objectives, hypotheses, logic, and measurements – how they fit together (or not) and how sound a conclusion is possible given what is there.
I am not a lawyer, but want to know enough to understand the significance of supreme court rulings. Same with science – we all want to evaluate medical advances on our own, to some extent, do we not?
Why Would I be a Reliable Vendor of Such Information?
An army of physician scientists roams the halls of academe. Why have I singled myself out to write about science as a critic and presumed teacher?
It is because I have busied myself for over 20 years teaching science at my university. Pupils have been science hopefuls, young people with a desire, seasoned faculty who want to hone their skills. Responsible teachers learn what to teach, usually from greater persons, as in my case. Nothing in my video is original with me except perhaps the idea of the Janus face, the two sides of an objective. My polestars are Karl Popper and Thomas Kuhn, who have small roles in the video but played for years on the great stage of world science.
What is My Objective?
“…Not for ambition or bread / Or the strut and trade of charms/ On the ivory stages..“, surely not.
For the pleasures of intellect, perhaps – those rarified amusements which lure people of a certain temperament into professorship.
Certainly for love of teaching, a most selfish act. When else can one learn at so high a rate?
In response to my passionate belief that understanding enlightens everyone, patients and physicians – to their mutual benefit.
Admirable effort, Dr. Coe. Yes, everyone SHOULD want to know. It seems that lately, however, “knowing” has become an almost impossible task for the average patient, given that, (1) some “research” is being performed with the goal of “proving” a predetermined outcome, for various reasons, not the least of which are financial and other monetary incentives coming from government, big pharma and other medical industries, (2) the recent proliferation of mandated “settled science” conclusions coming from academe and the “public health” arenas, which is antithetical to the basic premise of research (i. e. to re-“search” the scientific conclusions, and (3) apparent corruption in the “peer review” process which appears all too often. Academe and the “public health” arenas appear to be shockingly uninterested in addressing these barriers to the public “knowing”.
Thank you, Glenn, for your thoughtful remarks. In fact, Karl Popper – my intellectual superhero – says all we can do is falsify, and if that is not possible accept what we have until someone else falsifies it. A dour but effecting antidote to ‘settled science’. Fred