
by Dr Fredric Coe | Sep 15, 2016 | CASES
This is a first for the site, and perhaps it should have been a feature long ago. After all the generalizations and reviews there is something wonderful about a single instance that contains all the elements of a topic in the kind of instructive detail we can get only in life itself. Pat – who has permitted me to use his name and data – forms calcium stones and has idiopathic hypercalciuria and a job that makes hydration a problem. For treatment I wanted to use low sodium diet to lower his urine calcium excretion and if possible avoid thiazide diuretics just because of his job which is outside and in summertime poses serious heat loads. MIchelle, his wife, created a reliable low sodium diet for him as proven by multiple follow up tests and that reduction of sodium lowered urine sodium and stone risk, as one might expect. I asked her to share her experience in doing this, and she responded with this wonderful article. It helps that she is a professional writer! I am indebted to Michelle and Pat for their story, and I hope you like it.

by Dr Fredric Coe | Sep 1, 2016 | For Doctors, For Patients, For Scientists
Here are all the trials for prevention of idiopathic calcium stones, and my personal approach to using their results in clinical stone prevention. The whole site thus far has been built to support this article, which is the capstone of the enterprise. To highlight its importance I have made it header type larger.
Beside the usual references, I provide spreadsheets that contain all of the trial stone data with links to the original articles and PDF images of the articles. I also provide spreadsheets of stone risk data from the trials that I use in my analysis of the physiological responses to treatment. So this is a definitive as I can make it. I have left the two preceding videos in red because they are the steps up to this article, and perhaps people might want to view them in preparation. The two prior articles on phenotypes that come before the videos are also preparatory to this final presentation.
I say final because with the full presentation of all of the trials we have more or less covered the entirety of idiopathic calcium stone disease and need to move on to other stone types and to the systemic diseases that cause stones.

by Dr Fredric Coe | Jul 28, 2016 | For Doctors, For Patients, For Scientists
The second in this series of stone forming phenotypes, the calcium phosphate stone formers are less numerous than the calcium oxalate stone formers, but perhaps more worrisome, and certainly more complex. There are two types, those whose stones contain any brushite – an unusual form of calcium phosphate in stones, and those whose phosphate is only hydroxyapatite – the mineral found in bones. This latter group is to a large extent composed of young women, for reasons we do not know. Phosphate stones are likely than the calcium oxalate variety to be numerous, and often produce nephrocalcinosis, a mixture of small stones and tissue calcium deposits. Nephrocalcinosis, in turn, is often labelled medullary sponge kidney simply on radiological grounds, even when the distinctive lesions of MSK are not necessarily present. Likewise, phosphate stone patients can appear to have renal tubular acidosis because of nephrocalcinosis and because RTA and phosphate stone patients both produce a more alkaline urine than do normals, or patients with calcium oxalate stones. All in all, this is a complex form of calcium stones, challenging for clinicians and often very trying and concerning for patients with it. The article is long and difficult, so you might want to watch this video by way of an introduction.

by Dr Fredric Coe and Elaine Worcester, MD | Feb 26, 2016 | For Doctors, For Patients, For Scientists
This is an article that can be written only by the readers of this site. We are not product testers nor do we do market surveys. But given how many fluid and diet apps one can find on the web and also given how many people come to this site every month we should be able to get a good idea about which ones seem of value. The benefit of accumulating your experience in comments to this very brief article accrues to all of you who come here. Whether you use an app or not crowd sourcing of a kind can tell us all which ones seem really good, and we can all use that knowledge. There are almost no words in the article, but as the results come in – in other words if you will share – we will count up by app in a table or so, ongoing. As for smart bottles, there are only a few on the market, but we should be able to get an idea about them if you will share. So, here it is: A blank slate for everyone to write on so everyone can benefit. Please share.
by Dr Fredric Coe and Hatim Hassan, MD PhD | Feb 22, 2016 | For Doctors, For Scientists
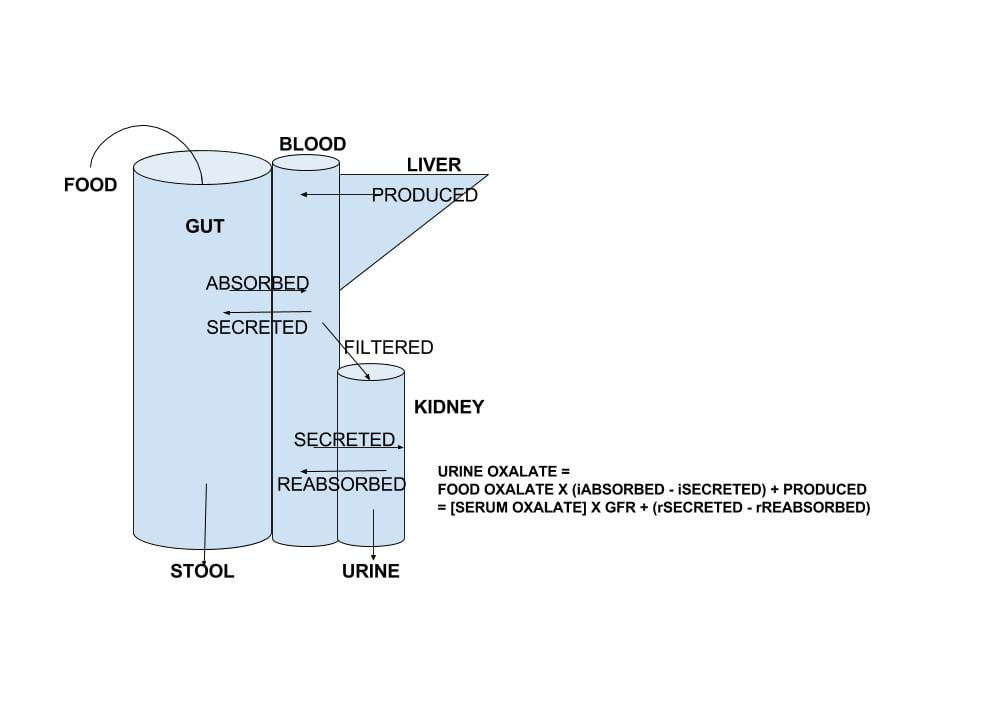
There is no doubt that urine oxalate excretion is an important factor in calcium oxalate kidney stone production, and that excretion is a very complex outcome of transport in the gut and kidney tubules and, of course, diet calcium intake. We have devoted a lot of energy to refining food oxalate lists and making a reasonable diet plan for oxalate. Here, we have taken on the harder task of reviewing the complex movements of oxalate from food into urine. The intestines not only absorb oxalate from food into the blood, they can secrete oxalate back out from blood into the gut lumen from which it is removed in the stool. The kidneys remove the net of diet oxalate absorbed minus that secreted by a process of filtration and subsequent renal cell reabsorption and secretion of that filtered oxalate. It is as though evolution has handled oxalate like a real hot potato: keep control of how much oxalate the kidneys need to remove and keep control of the blood oxalate concentration. This seems prudent – if one dares to speak this way about evolution – as oxalate can crystallize in blood as it does in urine and both processes can be dangerous. The new work on oxalate transport does not now directly translate into new tests or treatments for patients, but surely will. So I and my brilliant colleague Dr Hatim Hassan – who is the real expert here – have written about the future in medicine. Because the article is very complex and may not get a lot of readers – scared off – I have made a tiny movie to introduce it by way of encouragement.