
by Dr Fredric Coe and Elaine Worcester, MD | Feb 26, 2016 | For Doctors, For Patients, For Scientists
This is an article that can be written only by the readers of this site. We are not product testers nor do we do market surveys. But given how many fluid and diet apps one can find on the web and also given how many people come to this site every month we should be able to get a good idea about which ones seem of value. The benefit of accumulating your experience in comments to this very brief article accrues to all of you who come here. Whether you use an app or not crowd sourcing of a kind can tell us all which ones seem really good, and we can all use that knowledge. There are almost no words in the article, but as the results come in – in other words if you will share – we will count up by app in a table or so, ongoing. As for smart bottles, there are only a few on the market, but we should be able to get an idea about them if you will share. So, here it is: A blank slate for everyone to write on so everyone can benefit. Please share.
by Dr Fredric Coe and Hatim Hassan, MD PhD | Feb 22, 2016 | For Doctors, For Scientists
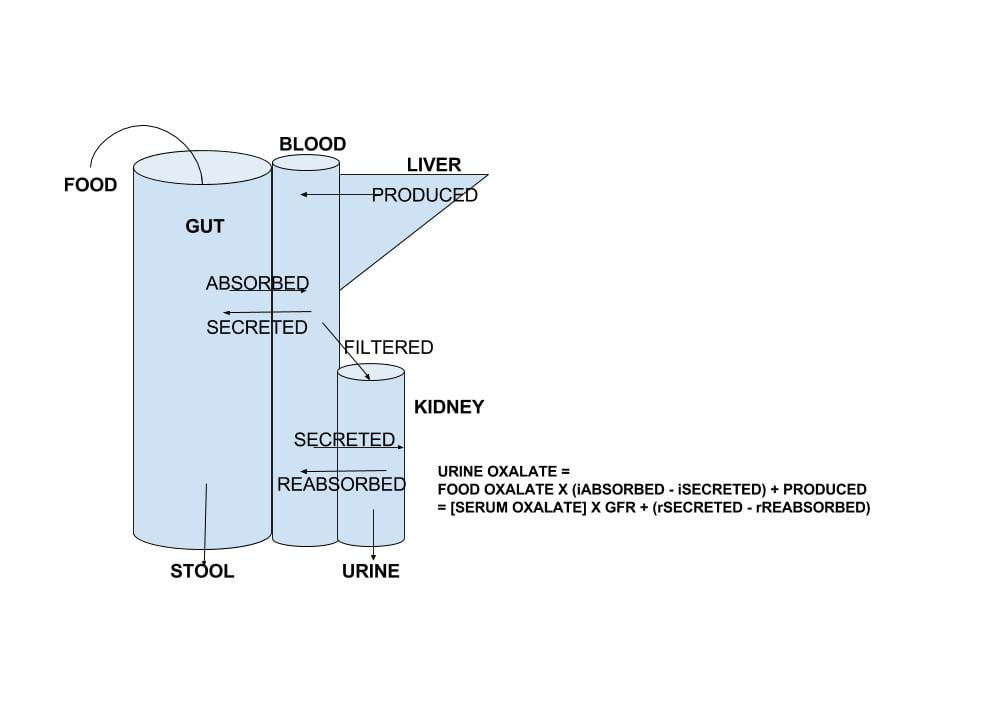
There is no doubt that urine oxalate excretion is an important factor in calcium oxalate kidney stone production, and that excretion is a very complex outcome of transport in the gut and kidney tubules and, of course, diet calcium intake. We have devoted a lot of energy to refining food oxalate lists and making a reasonable diet plan for oxalate. Here, we have taken on the harder task of reviewing the complex movements of oxalate from food into urine. The intestines not only absorb oxalate from food into the blood, they can secrete oxalate back out from blood into the gut lumen from which it is removed in the stool. The kidneys remove the net of diet oxalate absorbed minus that secreted by a process of filtration and subsequent renal cell reabsorption and secretion of that filtered oxalate. It is as though evolution has handled oxalate like a real hot potato: keep control of how much oxalate the kidneys need to remove and keep control of the blood oxalate concentration. This seems prudent – if one dares to speak this way about evolution – as oxalate can crystallize in blood as it does in urine and both processes can be dangerous. The new work on oxalate transport does not now directly translate into new tests or treatments for patients, but surely will. So I and my brilliant colleague Dr Hatim Hassan – who is the real expert here – have written about the future in medicine. Because the article is very complex and may not get a lot of readers – scared off – I have made a tiny movie to introduce it by way of encouragement.
by Dr Fredric Coe | Feb 16, 2016 | For Doctors, For Patients, For Scientists
This little goodie started with my partner Dr Anna Zisman who to wanted us to have a simpler format for patients to follow in looking at their 24 hour urine lab reports. Answer five easy questions and get back a list of what you have to do with fluids and diet. Try it. Let me know if it works. If not, can you help make it better?

by Dr Fredric Coe | Feb 14, 2016 | For Doctors, For Patients, For Scientists
Well, here it is, the last pillar in the foundation. My goal is to enable patients to achieve successful stone prevention and I believe this requires a partnership with their physicians, a partnership in which they play a very active individual role. Patients after all are the ones who can manage diet, fluid intake, and life demands, only they can assure that 24 hour urine collections are representative of normal life, and, frankly, only they can decide on a life of long term prevention. Stones being rarely fatal and usually not a cause of progressive kidney disease, patients can elect prevention or not, and their physicians are in a role more like attorneys and accountants than authoritarian directors of events. But as in Eden, one can expect proper choices only if one has provided full knowledge, which I have set out to accomplish. By proper I mean most suitable to patients given full knowledge, for some may not care to exercise themselves so much as I think they must to be successful, whereas others may consider the work of prevention slight indeed compared to the consequences of continued stones. In any event, this article is the end of that cycle of enablement I can manage, and I put it here, as in all writings, as the chef puts out her best effort – to face the indifferent judgement of the gourmet.
by Michael Borofsky, M.D. | Jan 24, 2016 | For Doctors, For Patients, For Scientists
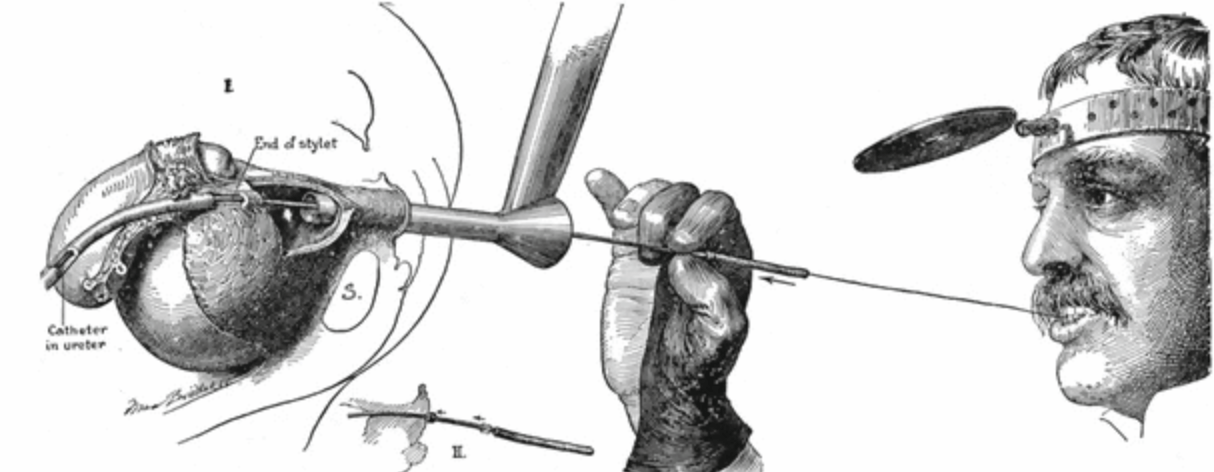
Dr. Mike Borofsky authored a favorite article on this site – Pain from Kidney Stones. Now, he has authored our first article on stone urology, meaning the urological surgeries used for treatment of stones in the kidneys and urinary tract. Ureteroscopy is fast becoming the preferred approach, outstripping shock wave lithotripsy and percutaneous lithotripsy. This is because the instruments for ureteroscopy offer superior optics and are flexible and small enough to get from the urethra up into the kidneys and into all of the crevices of the kidneys where stones form and lodge. Armed with tiny but powerful laser fibers, the new ureteroscopes permit surgeons to fracture stones in the kidneys and turn them into mostly harmless dust that passes silently for days or weeks thereafter, or into small fragments they take out during the procedure leaving not a speck behind. It is a brilliant time to be a young urologist and use these marvelous instruments to do what would otherwise require a far more complex and risky procedure (percutaneous nephrolithotomy) or depend upon an indirect and often incompletely effective one (shock wave lithotripsy).
by Dr Fredric Coe | Jan 11, 2016 | For Doctors, For Patients, For Scientists
These two articles cover the main stone types, and this new one on uric acid parallels the prior one on calcium stones. Like the calcium stone article it is meant for patients, although physicians might like some of the nuances. The purpose is not to make patients into their own physicians but to enable them to understand their own stone forming abnormalities. My ruling hypothesis is that patients want prevention, and will embrace and implement the changes needed with more enthusiasm and endurance if they fully understand the goals. LIkewise if they can themselves follow the effects of their efforts on stone risk factors they will believe that what they are doing has real meaning. I know that hypotheses are for disproving, and I know someone may well do a prospective double blind randomized trial, some day, to test mine. Right now, I believe in the idea because of Eden whose resident twosome were not just told about the tree but exactly why they should not eat of its fruit. I know it is an unfortunate comparison, given the outcome, but much effort was expended on education. My source for the details, apart from the Hebrew Bible, is Milton, J: Paradise Lost; Books V – Viii.