

Diagnosis of MSK is Increasing
Urologists and nephrologists specializing in the treatment of kidney stones seem to encounter patients with medullary sponge kidney (MSK) far more often than one would predict given the fact that this disease affects less than 0.5-1% of the general population.
One potential explanation is the high frequency of stones in such patients, nearly 70%. Stones call attention to themselves. Even so, referrals for MSK seem to be occurring at ever increasing rates, out of proportion to the prevalence of the disease.
Another explanation is that we can see more because of dramatic improvements in CT scanners and endoscopic equipment we use for stone removal.
Latest generation, thin slice CT scans can isolate tiny stones as small as a millimeter in size. Meanwhile, modern flexible endoscopes not only visualize every crevice of the renal collecting system but are able to do so in high definition. Consequently we can identify previously unrecognized variations in the appearance of stone forming kidneys, of particular interest here nephrocalcinosis on CT and tubular plugging on endoscopy.
But diagnostic capabilities may be progressing faster than our ability to comprehend the significance of what we see. As a result, one can misclassify patients as having MSK when the correct diagnosis is another more common finding such as nephrocalcinosis or tubule plugging.
For example, a urological surgeon performing ureteroscopy with a modern high resolution digital instrument notices “hundreds of tiny stones,”, “abnormal papillary architecture” or “stones located under the urothelium” and proceeds to label the patient with MSK. Or, a patient with urologic symptoms such as renal colic, recurrent urinary tract infections, or microhematuria has a CT scan showing ‘nephrocalcinosis’ and is labeled as having MSK.
In both instances, the true likelihood of actually having MSK is, by a recent small study, only 4/15 (25%), but physicians are not generally aware of the differences between MSK, nephrocalcinosis, and tubule plugging because these are new areas of knowledge which have not been proliferated widely.
This article is one way we hope to make the diagnosis of MSK, a unique and complex disorder of renal development, clearer for physicians and their patients.
What Is MSK?
Our collective understanding regarding the development and pathophysiology of MSK is rather sparse even though G. Lenarduzzi first described it in 1939.
The Cause of MSK
The exact mechanisms that produce MSK are unknown. It is believed to be a result of abnormal renal development in utero. More specifically, scientists believe the ureteric bud – which will give rise to the ureters – interacts abnormally with the metanephric blastema tissue in the embryo which will produce much of the kidney substance.
There appears to be a genetic component to the disease. Recent evidence is that about half of patients diagnosed with MSK will have at least one relative with some degree of similar affliction. This kind of familial clustering can suggest an autosomal dominant gene expression or the actions of multiple genes giving that impression. The review of the above link is an excellent recent treatment of the matter of development and genetics which we highly recommend.
The Anatomy of MSK
MSK, as its name implies, is characterized by sponge like, cavitary regions within one or both kidneys (Figure 1).
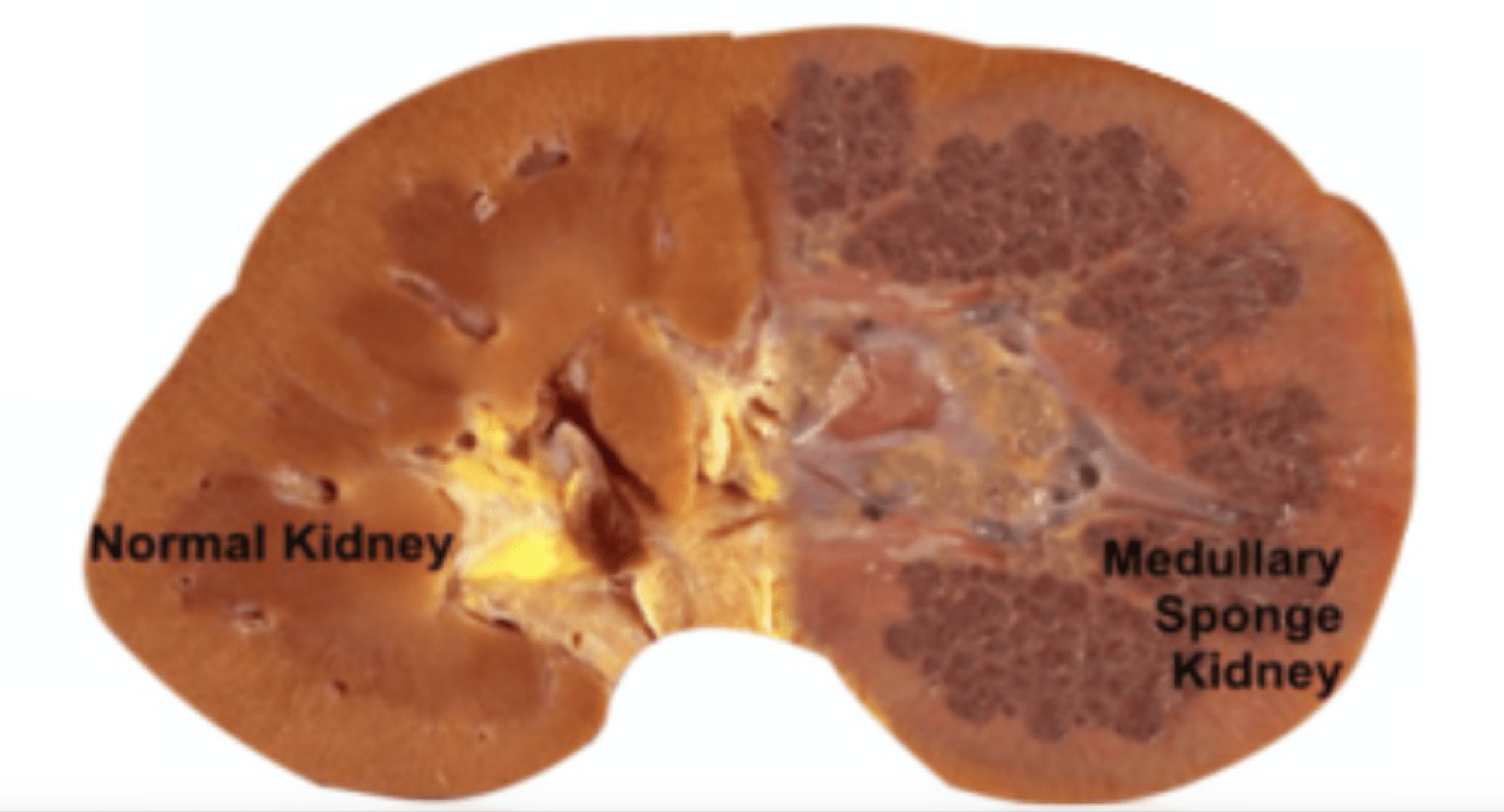
Figure 1 – A normal appearing kidney (left) compared to MSK kidney (right).
More specifically, the dilations occur in the inner medullary (precalyceal) collecting ducts. These collecting ducts are the terminal region of the nephrons, the individual functional units of the kidney.The inner medullary collecting ducts (IMCD) have the job of delivering urine to progressively larger ducts (ducts of Bellini) that deliver the final urine out of the renal papilla into the minor calyces (Figure 2) which connect into the renal pelvis and thence into the ureter to the bladder.
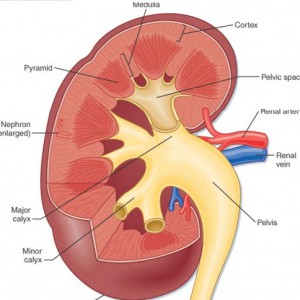
One way to think of the IMCD is as a collection of streams merging and forming a river (duct of Bellini) which leads to a delta (minor calyx) and then a lake (major calyx) and ultimately an ocean (renal pelvis) (Figure 2).
Figure 2 – Anatomic depiction of kidney and collecting system
The IMCDs are not visualized in Figure 2 but if you scan down to Figure 3 just below several human nephrons which were microdissected from an MSK kidney show what is really wrong with them.
In MSK, some IMCD are dilated markedly and have outpouchings (cysts): blind sacs which begin at the IMCD lumen but go nowhere – like a hallway someone walled off at one end. It is at the ends of these hallways one finds the stones, free floating and probably trouble. Other IMCD are not dilated and do not have cystic outpouchings.
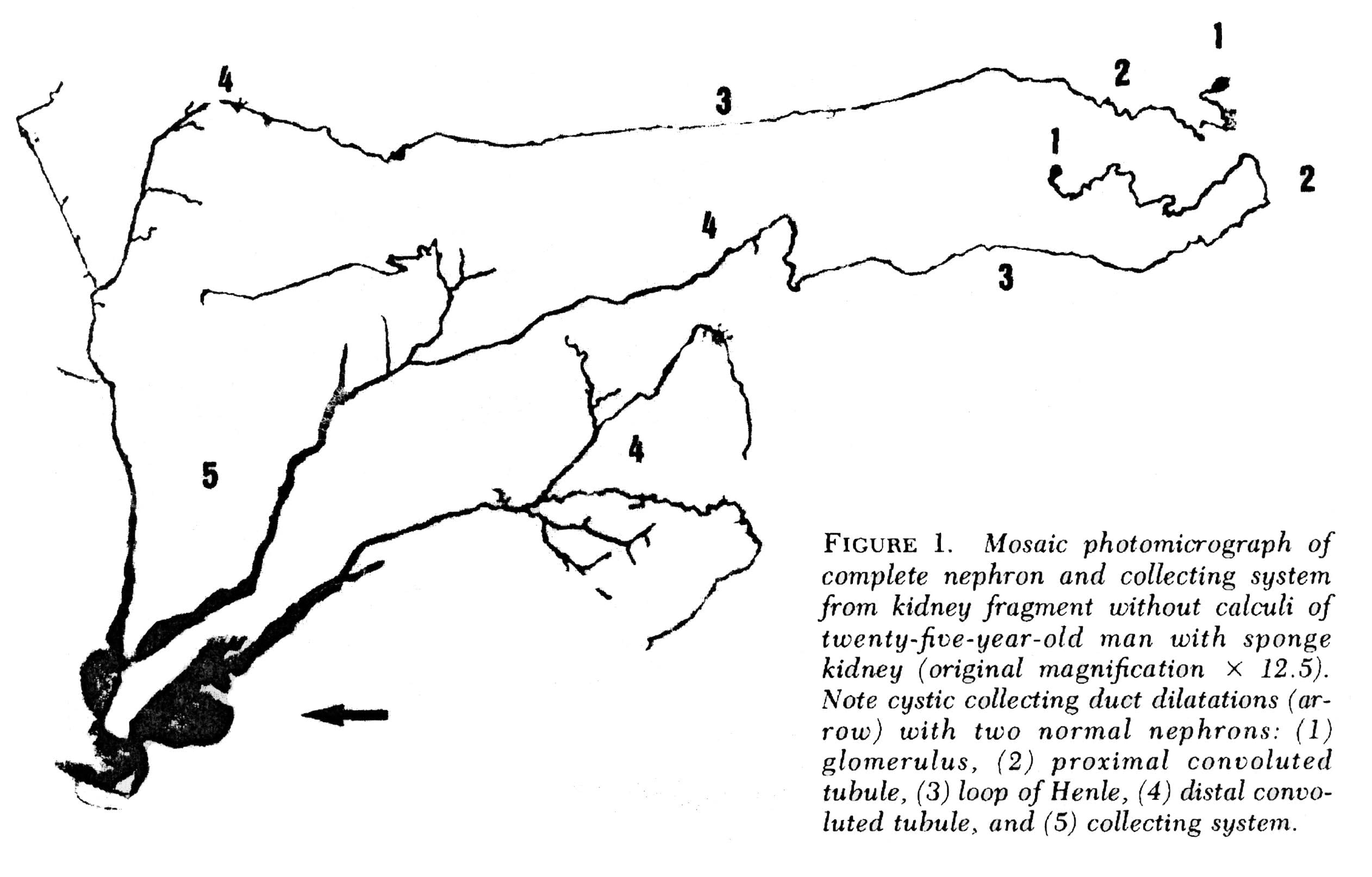 Figure 3 – Microdissection of complete nephrons from MSK. Irregular dilation of the IMCD is present. Cystic outpouchings are present, of varying sizes. The blind ends are obvious. It is in these cysts that tiny stones are found.
Figure 3 – Microdissection of complete nephrons from MSK. Irregular dilation of the IMCD is present. Cystic outpouchings are present, of varying sizes. The blind ends are obvious. It is in these cysts that tiny stones are found.
Quite apart from the IMCD dilatation and cysts, the kidneys of MSK have two other abnormalities which mark it as a specific disease. Those IMCD which are not dilated nor cystic have a multilayered epithelial lining, whereas a normal undilated IMCD lining is one cell layer thick. The interstitial cells of the renal papillum – the cells between the tubules and vessels – are more numerous than in normal kidneys, and have an immature appearance much like is seen in fetal kidneys.
Why Stones Form in MSK
Elsewhere on this site we have pointed out that supersaturation is a force, a source of energy directed at forming solid phases such as stone crystals. The kinetic retardants in urine, which include citrate, stave off crystallization but can never prevent it: A supersaturated solution will eventually collapse into two phases, crystals and a residual solution precisely at the solubility point, devoid of extra free energy.
The stagnant flow as a result of the dilated MSK IMCD, and particularly the static conditions in the fluid filled blind ended cysts, are the probable reason those innumerable tiny stones form which end up packing the ‘sponges’ with masses of crystals. How MSK patients produce larger stones, big enough to block the ureter is unknown. It is not true that MSK patients have remarkably high urine supersaturations or other physiologic abnormalities such as hypercalciuria and hypocitraturia. Possibly the tiny stones somehow leave their cysts and enter the urine where they act as nucleation centers.
Other Associations
Other common associations with MSK include urinary tract infection, microscopic and gross hematuria, and impaired renal function. Perhaps the stagnant flow in dilated IMCD and particularly in cysts, predisposes to infection. But since the papillae are abnormal in other ways it seems likely that these intrinsic abnormalities themselves must be clinically important, and more work needs to be done on the problem.
Making the Diagnosis of MSK
Of course, when we speak of what is wrong in the MSK kidneys, and how it affects people, we base everything on knowing that a given patient has MSK. If you have a kidney from such a patient and can show the dilated IMCD, the cysts, the tri-layered IMCD epithelium, and abnormal interstitial cells, diagnosis is certain. But what can we do when we are dealing with a patient?
Radiological Studies
Intravenous Urography
Historically, the diagnosis of MSK has been made on intravenous urography (IVU). Radiographic contrast is administered and x-rays of the kidneys, ureter, and bladder are taken periodically as the contrast is absorbed and later excreted by the kidneys through the urinary tract.
The delayed phase image is essential for diagnosis. This is when contrast material fills the masses of dilated IMCD and cysts which make up the sponge.
The masses of dilated IMCD filled with contrast material produce a characteristic ‘papillary blush’ which appears like flames on the outer edges of the papillae. When particularly large it can mimic a bouquet of flowers peripheral to the collecting system.
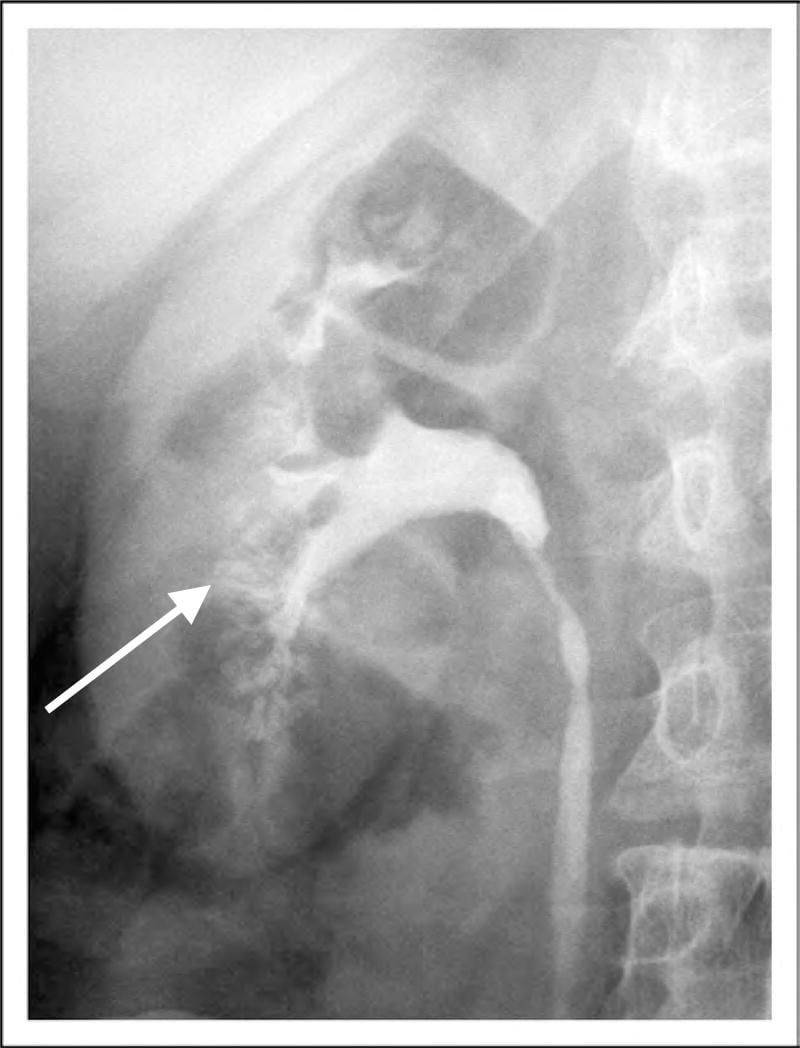
Figure 4 – IVU image of medullary sponge kidney. The arrow designates the papillary blush in the mass of dilated IMCD space.
CT Scans and Other Imaging
Over the past 10-15 years, noncontrast CT scans have replaced IVU as the imaging method of choice for stone formers. While these scans are more sensitive in detecting small stones, the lack of contrast limits the ability to accurately diagnose MSK and has raised concerns regarding the potential for under-diagnosis of this disease.
CT does have the capability of making this diagnosis when contrast is given and CT urography is performed; though this is not used as a first line choice for stone imaging and is generally reserved for specific indications such as hematuria and concern for urinary tract injuries.

Figure 5 – Demonstration of papillary blush (small arrows) on CT urography for patient with medullary sponge kidney.
Use of other imaging modalities have been investigated as well though they have proven suboptimal in their diagnostic capabilities. Ultrasound has poor sensitivity to detect dilation of the collecting ducts and MRI has the potential to delineate detailed renal anatomy but can not detect stones or calcification.
High Definition Endoscopy
State of the art high definition endoscopes have allowed investigators to make observations at the time of renal endoscopy correlating the appearance of the renal papillae and collecting system to specific types of diseases and metabolic derangements associated with stone formation. Because endoscopy is now being performed as a common and often preferred way to manage stones, this kind of detailed imaging of kidneys will be available more and more in the course of regular patient care and permit physicians to diagnose the exact kinds of disorders in the kidneys of stone formers.
Medullary sponge kidney in particular has an entirely unique appearance unlike any other type of stone related disease, making endoscopy a particularly exacting diagnostic procedure. Detailed anatomic descriptions from twelve such patients each with evidence of MSK on biopsy were recently described by Evan et al.
The Papillary Malformations Seen Via Endoscopy
In stone formers the papillae often appear abnormal, a concept that merits its own post and which we can only briefly summarize here.
Plaque
The renal 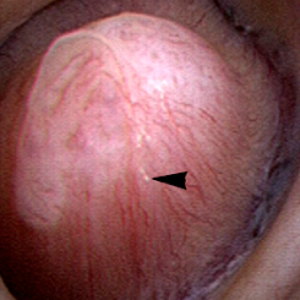 papilla is the anatomic subunit of the kidney where the IMCD merge together into the terminal Bellini ducts which empty into the minor calyx. Normally, it should have the appearance of a smooth walled mound or mountain without much if any calcification (plaque) along its surface. The link is to a detailed post about plaque by Dr Andrew Evan.
papilla is the anatomic subunit of the kidney where the IMCD merge together into the terminal Bellini ducts which empty into the minor calyx. Normally, it should have the appearance of a smooth walled mound or mountain without much if any calcification (plaque) along its surface. The link is to a detailed post about plaque by Dr Andrew Evan.
Figure 6 – Healthy appearing renal papilla with a minimal amount of Randall’s plaque (arrowhead).
Ductal Plugging
Another common abnormality identified in many papillae at the time of endoscopy are plugged ducts. The physiologic mechanisms for this process are currently unclear; 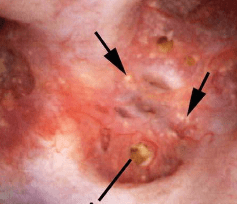 however, we believe it is a reflection of injury that begins a potentially disastrous chain of events for stone formers.
however, we believe it is a reflection of injury that begins a potentially disastrous chain of events for stone formers.
Figure 7 – Abnormal papilla in a patient with severe ductal plugging. Yellow mineral deposits (arrows) can be seen protruding from dilated ducts of Bellini.
Our present assumptions are that once crystals begin to form within a duct, they damage the lining cells and the duct loses its ability to make acidic urine. This in turn raises the local pH level and leads to the growth of more calcium phosphate mineral deposits which are favored by high pH.
Unclear is what begins this process. Since these ducts contain fluid which is very close in composition to the final urine, we suspect it is high supersaturation with respect to calcium phosphate. This occurs in those patients with both high urine calcium excretions (hypercalciuria) and higher urine pH levels – above 6.2. Such patients often form stones high in calcium phosphate composition and plugging is strongly associated with formation of such stones.
The mineral deposits subsequently grow and we believe can even act as a nidus for stone formation. The corresponding papillae can look markedly abnormal and the dilated ducts are easily evident. Remnant dilated ducts left behind after the mineral is spit out or surgically removed (Figure 8) show dilation without the mineral plug.
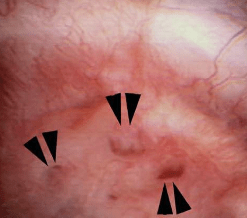 Figure 8 – Evidence of abnormally dilated ducts (arrowheads) at the surface of a papilla.
Figure 8 – Evidence of abnormally dilated ducts (arrowheads) at the surface of a papilla.
MSK
The findings in MSK are comparable in some ways to ductal plugging; however, rather than the papillae having one or several abnormally dilated ducts, the entirety of the papillum is markedly abnormal.
Therefore MSK and plugging type papillae look remarkably different.
The MSK papillae are excessively round, enlarged, and billowy (Figure 9).
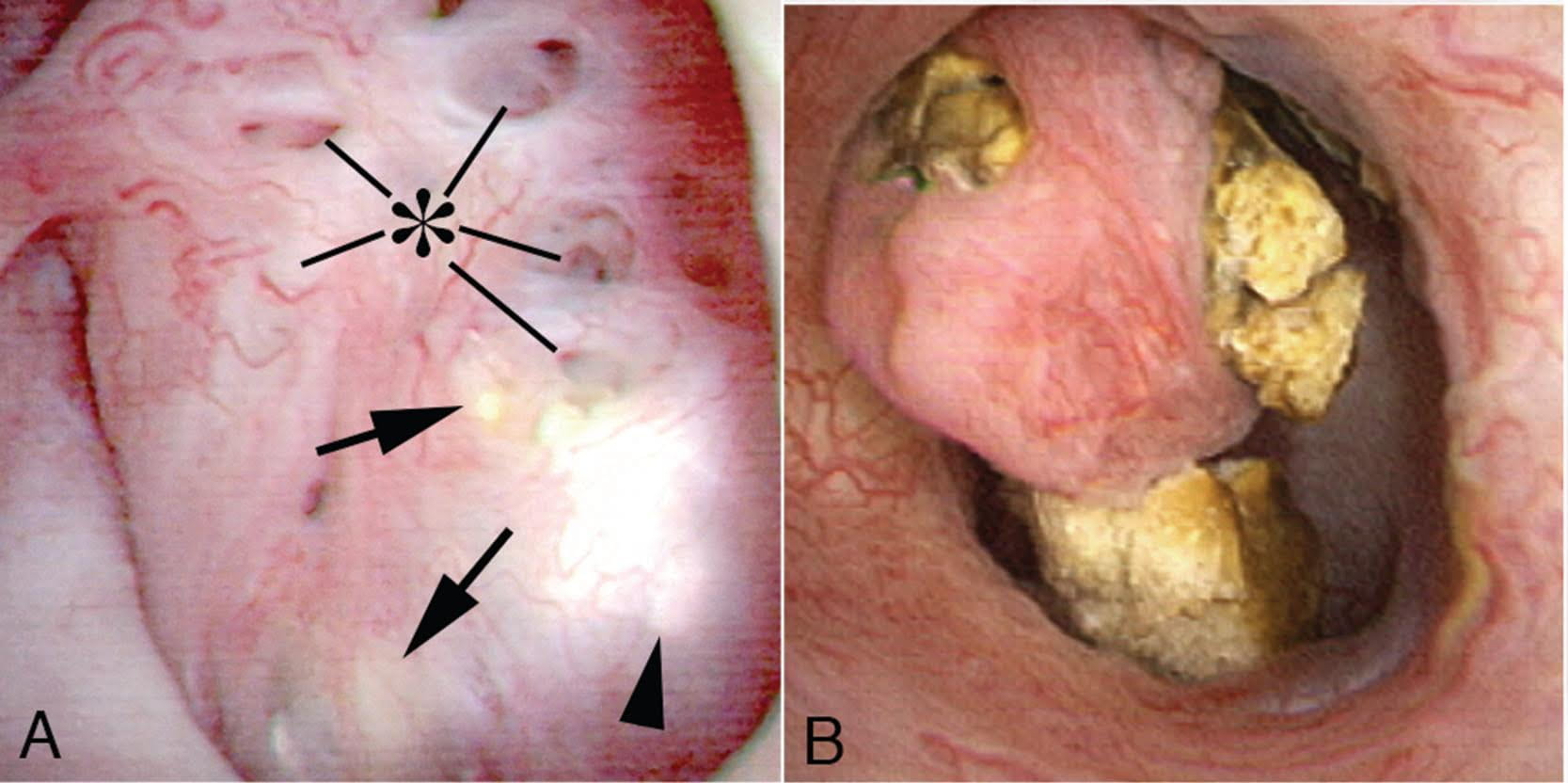 Figure 9 – A papillum in a patient with medullary sponge kidney. The papillae are rounded and enlarged with a billowy appearance. The papillary tips are blunted. No other kind of papillary disease is known to present this appearance which is therefore pathognomonic of MSK. Panel a shows dilated Bellini duct openings at asterisk; the arrows show yellow plaque – plugging of IMCD completely separate from the stones which fill dilated IMCD, the arrowheads show traces of white plaque. Panel b shows the billowy papillum with a blunted tip surrounded by calyceal stones.
Figure 9 – A papillum in a patient with medullary sponge kidney. The papillae are rounded and enlarged with a billowy appearance. The papillary tips are blunted. No other kind of papillary disease is known to present this appearance which is therefore pathognomonic of MSK. Panel a shows dilated Bellini duct openings at asterisk; the arrows show yellow plaque – plugging of IMCD completely separate from the stones which fill dilated IMCD, the arrowheads show traces of white plaque. Panel b shows the billowy papillum with a blunted tip surrounded by calyceal stones.
In the majority of such cases, these changes are seen diffusely throughout each kidney, though segmental sponge findings are present in a minority of patients.
The differences in appearance are well demonstrated in the post by Dr. Evan and the following video. With ductal plugging the bulk architecture of the papilla is intact though many ductal plugs are seen. Note the way the ductal plugs are adherent to the lumen.
In MSK on the other hand, the papillary architecture has and unique, billowy appearance with massively dilated ducts and freely mobile stones within them. The following video is from a patient with MSK. A duct of Bellini is massively dilated and numerous tiny stones which are free floating pass out of it during the visualization as the opening is enlarged with a laser. You can see stones bouncing within the duct because of movement of the irrigation fluid.
Clearly neither papillum is “normal” and one can imagine the tendency to misdiagnose a plugging patient as a MSK patient unless the two patterns are clearly in one’s mind.
The ductal deposits themselves are an important clue. In all plugging diseases but cystinuria ductal mineral plugs are fixed within the ducts because the crystals adhere to the lining cells and often destroy them. As the lining cells are destroyed crystals fix themselves to the basement membranes, the collagen shell on which the lining cells once grew. Inflammation follows such injury with scarring and loss of the tubule segments. Deposits therefore never float free from a dilated duct except in cystinuria and in MSK. Cystinuria is usually diagnosed directly from stone analysis and urine cystine screening.
Perhaps because the tiny stones in MSK do not attach to the epithelium of IMCD there is no evidence of cell injury or inflammation, in marked contrast to all of the plugging diseases. Even in cystinuria injury occurs, not from the free floating distal cystine plugs but from calcium phosphate plugs which form in the IMCD.
Stones may cause pain in MSK despite the lack of ureteral obstruction and inflammation and cell injury. Possibly distention of the dilated ducts by masses of tiny stones could be a factor. Consequently, laser unroofing has been postulated as a potential treatment option in both disease states: those with plugging and MSK.
The video may not make it easy for everyone to visualize the stones and cavities of MSK. The 4 still pictures below show much the same thing for clarity.
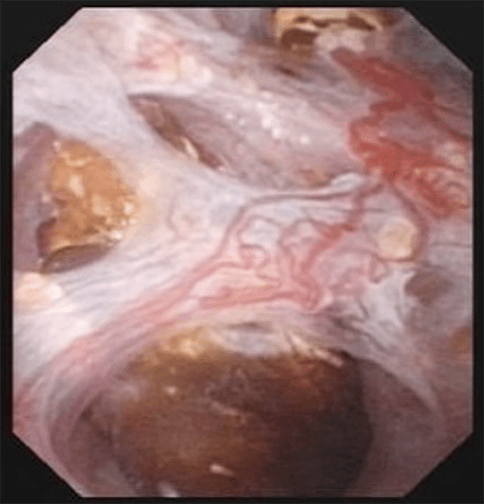
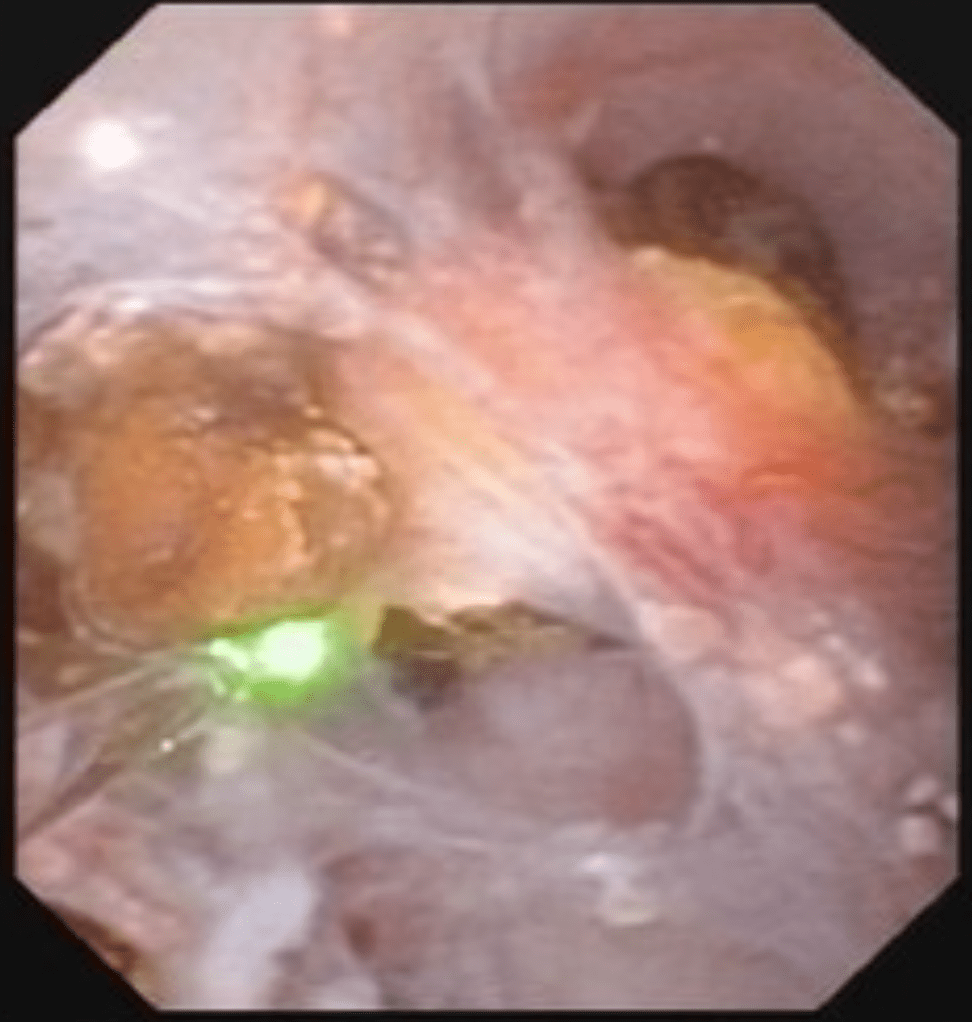
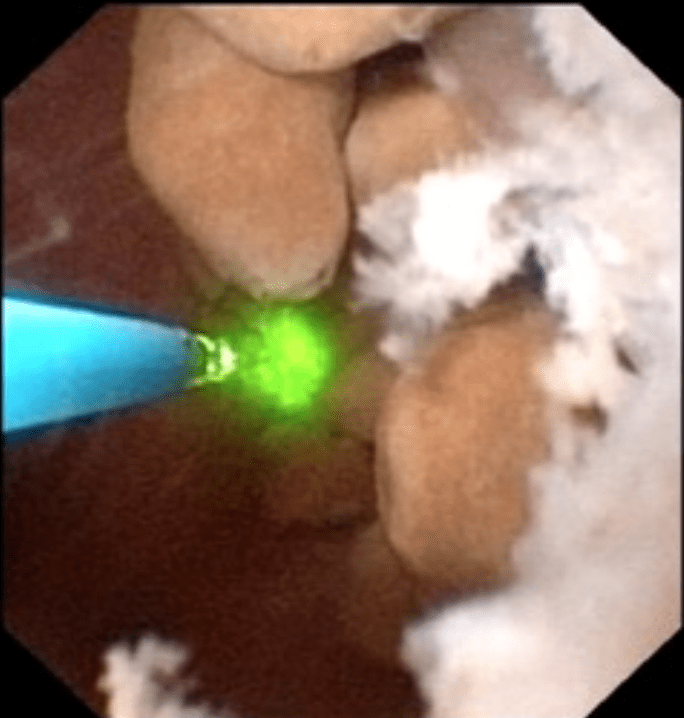
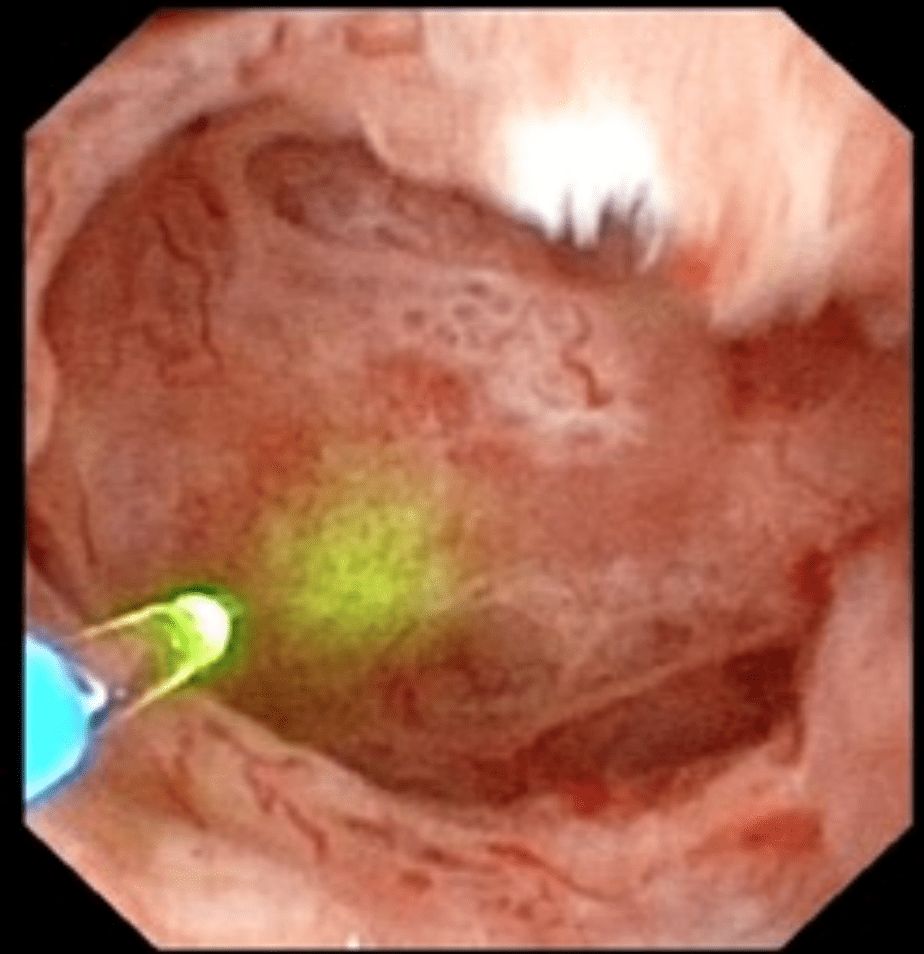
Figure 10 (a-d) – Example of laser unroofing of sponge cavity full of freely floating stones. The massively dilated MSK bellini ducts are seen in Panel a; the white speckles at 9 o’clock are tiny stones in dilated IMCD or cysts. Panel b shows a holmium laser fiber being used to open dilated IMCD or cysts. Panel c shows masses of tiny stones free in dilated IMCD or cysts which float out as the surface is incised with the laser. In panel d, the remnant sponge cavity can be seen now free of stones.
Nephrocalcinosis and MSK
Strictly speaking, nephrocalcinosis refers to the presence of calcium deposits in the kidney tissue. Of course, this includes ductal plugging and the masses of tiny micro – stones inside cavities produced by numerous dilated IMCD in MSK. However, the word ‘nephrocalcinosis’ is also used as a radiological diagnosis which is far less specific.
Limitations of Radiology
When radiologists speak of nephrocalcinosis they can mean large numbers of calcifications within the collecting system or kidney tissue, because they cannot differentiate reliably between tissue calcifications and stones. When urologists speak of nephrocalcinosis seen during high resolution endoscopy they can specify if it refers to tissue calcifications, stones, or both, and will reserve the term for that component arising from tissue calcifications.
MSK is one of several disease states that is commonly associated with extensive nephrocalcinosis observed by radiologists. Other common conditions are stones caused by renal tubular acidosis and primary hyperparathyroidism. Calcium phosphate stone formers without any systemic disease can also produce sufficient combinations of ductal plugging and stones that nephrocalcinosis is diagnosed radiologically.
In a recent study of 67 idiopathic calcium stone forming patients undergoing percutaneous nephrolithotomy, rates of nephrocalcinosis ranged from 18-71% depending on the type of associated stone.
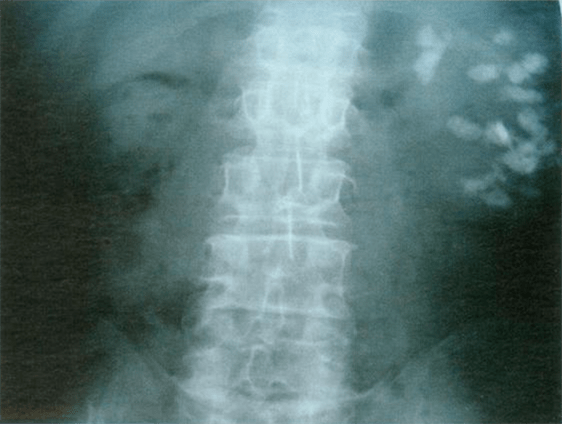
Figure 11- X-ray example of patient with MSK affecting the left kidney. Extensive nephrocalcinosis is seen.
Because radiographs cannot reliably distinguish tissue calcifications from stones adjacent to tissues, the very word ‘nephrocalcinosis’ needs to be re-defined.
In particular, the situation with respect to diagnosis of MSK has worsened as radiological techniques have changes. When IVU was the first line imaging modality for stones, contrast enhanced urographic phase imaging gave additional clues to MSK – the papillary blush illustrated in a prior section.
Nowadays since a single non-contrast CT series is all that is typically performed, the papillary blush effect cannot be seen, and diagnosis of MSK must rely more on the presence and pattern of nephrocalcinosis itself, which is not very specific to MSK. This means that the diagnosis of MSK by radiology has become unreliable.
The Power of Endoscopy
Differentiation of Nephrocalcinosis from Stones
During endoscopic procedures, stones and tissue calcifications can be directly identified and told apart. For example, in the images below, some of the calcifications were identified as stones. Others were tissue calcium deposits such as plugging or extensive plaque.
This has led to the notion that kidneys should only be labeled as having nephrocalcinosis once confirmed visually on endoscopy.

Figure 12 (A-C) – Evidence of increasing degrees of nephrocalcinosis confirmed visually at the time of percutaneous nephrolithotomy. In each image a nephrostomy tube (not calcification) is depicted by an arrow. The remainder of the images have increasing degrees of calcification (bright white) within the kidney. Ignoring the nephrostomy tube, one can clearly appreciate a minimal but very present degree of accessory brightness (calcification) in panel A, a moderate amount in panel B and a severe amount in panel C.
Diagnosis of MSK
Of course, all of the problems of nephrocalcinosis are compounded when it comes to MSK. Stones and tissue mineral are easily mistaken for one another in CT scans, and ‘MSK’ affixed as a label to patients who do not have it. Endoscopy will easily identify the remarkably abnormal papillary shapes and dilated sponges, so MSK patients are properly diagnosed.
Tips for diagnosing MSK
1) Confirmation with flexible renal endoscopy can make a definitive diagnosis in patients suspected to have MSK and can be diagnostic as well as potentially therapeutic in terms of stone removal.
2) Consider urographic phase imaging either with IVU or CTU to confirm MSK suspicion in cases where renal endoscopy is not clinically indicated.
3) MSK should not be confused with ductal plugging as these are distinct clinical entities.
4) Nephrocalcinosis is more common than previously appreciated and does not necessarily indicate systemic disease or the specific developmental disorder of MSK.
A Final Word on Treatment
MSK is a true disease and deserves more attention and research efforts to help clarify its etiology and optimize treatment strategies. Because diagnosis by CT scanning is unreliable, the condition is easily overdiagnosed, a problem which leads to many kinds of confusion, clinical and research.
Alternative diagnoses to MSK, such as severe ductal plugging, are not benign and require their own treatment in order to prevent progression. Very often patients with plugging have multiple and severe abnormalities of urine chemistry which can be treated with diet and medications. Proper classification of patients is therefore especially important as different disease states may require unique treatment strategies.
In the event that an accurate MSK diagnosis is made, the tendency to give up on treatment and surrender to the inherent challenges of the disease should be avoided. In fact, these are the patients where metabolic evaluations and attempts at stone prevention are most critical.
Moreover, just because many of these patients tend to have extensive nephrocalcinosis on imaging does not mean they can’t form symptomatic stones in the collecting system as well. In fact, for such patients the clinical history is especially important as visualizing new stones in the setting of extensive nephrocalcinosis can be quite challenging.
Oftentimes when there is a high index of suspicion based on clinical factors, the optimal approach is ureteroscopy as this can be both diagnostic and therapeutic.
That being said, realistic surgical goals should be established. Clearing all stones from such kidneys is rarely feasible, though unroofing those pockets closest to the collecting system or largest on CT imaging offers a good place to start.
MSK is a complex and poorly understood disease that can manifest uniquely from patient to patient. In that respect what works for one person may not be appropriate for another and treatment strategies should thus be organized on a patient to patient basis.
Thank you so much for your work here. I was recently diagnosed with MSK based on the the results of a CT scan. I’m skeptical, however. I am 39 and have had three children. I have had no kidney stones and only the very rare UTI throughout my life. My chief complaint over the past few months has been urinary frequency that has now developed into what is the CONSTANT sensation of having a very full bladder and needing to urinate. This has become very disruptive and is keeping me from sleeping, concentrating and functioning normally throughout the day. I feel bladder pressure and what I would describe as irritation (discomfort and with a slight burning sensation, but not what I would consider pain). This feeling never goes away. Is it at all possible that this a rare presentation of symptoms that really are due to MSK? Or does it seem more likely to you that something else must be underlying this problem? Or course I realize the limitations of weighing in on such complex issues from a distance, but any of your brief insights would be appreciated. Thanks for your time and expertise!
Hi Erin, The most likely possibility is that a tiny stone or mass of crystals is lodged at the junction of the ureter and bladder. I imaging your physicians have already looked but it is easy to miss – not their reading but just hard to visualize. This is not rare. MSK was diagnosed perhaps because of multiple calcified sites in the kidneys so you should be evaluated to find out why they formed and take steps to halt the process. Take a look here. Regards, Fred Coe
I was diagnosed with MSK by my 1st urologist in 2006 when he removed 10 stones, calcium stones, from both of my kidneys. As far as I know I had not ever had a kidney stone before. It took over 3 years to get the diagnosis due to I have atypical symptoms.. , extreme dizziness, feel like I will pass out, nausea, vomiting, mainly. No pain when passing a stone, except when I had a 1.4 CM, yes CM, stone trying to pass in left ureter in 8/28/2015. I had already been set for surgery again on 9/2 by ureteroscope for these to be removed.. IT did not wait. It had been in lower pole of left kidney. the dr LEFT, another 1.2 CM and a 7mm and 9mm stone in that same kidney that day. I have just had a ct scan again on 7/14/2016 due to having the symptoms above, and it only shows a 5 mm mid pole and a m in 1 cm in lower pole. I have went to an extremely acidic diet, only distilled water and no calcium intake at all. I have not given up cheese entirely, but it is less than 1/8 – 1/4 cup in a day and only occasionally at that. My urine and blood calcium are still high, I know you mentioned parathyroidism above, have likely is it for this to coincide with MSK? I am very sick and tired of being sick and dizzy and having subsequent panic attacks associated with the pass out feelings and the fear of that huge stone passing again…. It was a nightmare. I am allergic to all morphine derivatives. I want to mitigate this as much as possible with diet and that. I consume min 1 gallon distilled water a day, usually closer to 2 gallons. Nephrologist wants me to go on UrocitK and bind the CA in my blood, I am truly afraid of this as well due to I do want to increase my already elevated risk of heart attack and stroke by doing that. Could parathyroid issues be making my calcium levels off badly and be exacerbating the MSK? I have asked and asked for endocrinologist referral over the years several and the answer is always.. you have MSK it is what it is… I am tired of living with this “lame” answer. Please any feedback you can give me would be beyond appreciated. I literally drink apple cider vinegar, about 1/4 cup a day, and then drink OJ, the real stuff, eat tomatoes- in all forms everyday and many other dietary changes to mitigate this. Please feel free to email me as well if need be. What would be the correct CA level blood and urine wise for a person with MSK? I know it is a million questions. I am tired of being this sick all the time.
Hi TaLona, You do seem to have a complicated problem. If your blood calcium is high then you have some primary systemic disorder, perhaps primary hyperparathyroidism that requires specific treatment. A very low calcium diet is not a seemingly good treatment for any kind of stone disease I know of, and I do not imagine your physicians would want it. MSK, or perhaps simply multiple renal calcium deposits, certainly can coexist and even be caused by primary hyperparathyroidism, or many other disorders. Given all the complexity, feel free to email me – address is on the site – and I will try to be more specifically helpful. Regards, Fred Coe
I was diagnosed with MSK in March. I’ve had kidney stones, kidney infections and UTI’s for several years. I had one 5 mm stone removed in April ir had completly blocked off my left kidney, after I passed a 4 and 3 mm. I still pass small ones on a regular basis. My question here is about pain. Its like my kidneys and tubes hurt all the time. Why is this? My doctor tells me he sees no reason for pain. However other MSK people complain with pain too. I really just want to find a doctor close to me that can give me some insight into MSK other than just saying I have it
Hi, I was diagnosed with MSK last year. I do not have problems with stones passing, but used to have a lot of problems with UTIs. When I found my new urologist, he kept asking me how long I had my kidney stones and I had no idea what he was talking about. Apparently they were noticed when I had an ultrasound completed for something else. I have been taking Urocit for almost a year now and was told they are doing better. My question is, do I really need to see both the Urologist and Nephrologist three times a year or can one suffice?
Hi MIsty, So your stones were noticed in the course of other studies and therefore incidental though important. No one has evaluated you to see why you formed them? If not, here is a plan to follow, because there is, or was a cause and you do not want more. Potassium citrate can be an excellent medication for stones, but it is not always the right one, depending on your results. Get the proper evaluation, and have treatment fitted to the outcome. Regards, Fred Coe
Thank you for your quick reply. The stones are from high uric acid. I did read your attached link and it was very helpful. Thank you.
Hi Misty, were the stone themselves uric acid? Or was the urine high in uric acid? Regards, Fred Coe
It is from high uric acid
Hi Misty, Thanks for the information. Be sure to ask if the stones are made of uric acid or are caused by uric acid. Warm regards, Fred Coe
Can you or anyone on here please tell me how to keep your teeth from breaking my cousin has msk and because she cannot intake too much calcium her teeth are constantly breaking even though she brushes them regularly, does anyone else have this problem or any tips?
Hi Rudi, Perhaps the problem is a low calcium diet. People with calcium stones need precisely the opposite – a high calcium diet albeit one with minimal sodium. This sounds paradoxical but is not. Here is a good link for you to consider. Bone and dental mineral are not remarkably different although the usual symptom of low calcium diet is loose teeth as the jaw bones weaken. Regards, Fred Coe
Hello Doctor Coe! Very nice to see you are still investigating those pesky stones. I hope you are well and hope you remember me. Did we ever make a decision on if I had true MSK or is it a ? ? I recently had a kidney clean out on my left kidney at Presbyterian in NY. It took 9 hours but really helped me out. My kidneys hurt everyday the older I get the worse the pain gets lol. Best.. Carol. H.
Hi Carol, Your recent surgery should have told us in that your urologist would have been able to see if you have MSK or not. Ask him and let us know – I especially! We now understand that CT scans cannot differentiate one kind of nephrocalcinosis from another, but surgical observation is now very accurate. Thanks for writing, Best, Fred Coe
Wow Doctor Coe this site is awesome! I’m so happy to have found it and so happy you are helping other MSKers. My new PCP yelled at me and told me there is no way I can have pain that the only pain with stones is when they travel down the ureter. Ugh please do not tell me that I have been dealing with this for 35 – 40 years now. Time for a new PCP.. the insurance is such a mess right now but I definitely should get back to Chicago with all my tests. Best
Dear Carol, I think everyone is beginning to understand that small stones can and do cause pain, sometimes a lot of it. The issue is what to do. Surgery is the obvious answer and a trial is needed. Warm Regards, Fred Coe
Agreed… especially depending on the shape of stone. Even the smallest of stones can impede in ureter and require surgery.
In 2000 I found out I had 3 9mm stones in my left kidney due to 2 weeks of bleeding and some pain. I had surgery a couple days later and then again 2 weeks after that due to a hole the dr. put in my ureter. I have been in and out of the dr.’s office over the years for bad back pain. I’ve had injections 3 times which never seemed to help with pain. I asked if my back pain could be caused from having kidney stones in the past and the dr. said no. In 2009 after coming home from vacation on a plane i thought I was going to die of pain. I went to the back specialist again and said in tears, someone needs to help me. They did a bone spec test which came back red flagging my kidneys. I went to the nephrologist and was told I had medullary nephrocalcinosis and both kidneys were about 75% calcified with about 60,000 stones in them. Surgery was out of the question, as it would destroy my kidneys. I’m used to passing stones and have a high threshold for pain but I seem to always be in pain. Sometimes it feels like my back has been thrown against a wall. Just stanling and talking to someone for 10 min. makes me have to bend over in a ball and release pain. Even when i bend down to empty the litter box it feels as though I’ve been gardening for hours. One of the dr.s said i had an even rarer muscle problem that some msk patiants have, although I list the paper and have no idea what it said. I was also told that there isn’t a way to get rid of the stones and that taking potassium citrate 540 mg 3 times a day would help not develop anymore stones. Are there any other people that are in tons of pain like me? I use to be a clean freak and now just folding clothes exausts me. I have a very hard time just doing daily activities. I am in great health otherwise and love working out and doing outdoor activities. Now I can’t do those things without pain medicine first. I don’t like pain meds because they make me hyper. Do you have any suggestions for me?
Dear Susan, Medullary nephrocalcinosis can be MSK or simply calcium phosphate stones with plugging of tubules. Either way your pain sounds horrible. From this distance I cannot second guess your physicians as all depends on the details of your images and the results of your blood and 24 hour testing and stone analyses. Since your physicians have clearly done all they can and you remain disabled by pain, I am sure they would be pleased to help you find a second opinion or alternative source of care to supplement what they themselves can do for you. As for potassium citrate I cannot be sure if it will help as I do not know your lab findings. So my suggestion, perhaps too obvious, is seek additional skilled help. Sometimes medical centers at universities will have people who are specially skilled in what you need. Regards, Fred Coe
Thank You, SO VERY MUCH!! Amazing not one doctor face to face has explained and set my fears at ease like you and the information above! Sincerely grateful….M.Martinez.
Hello again Doctor Coe… that was a big YES from urologist. If you need a good referral for the NY area let me know. I have sent 4 people I know to this urologist and they all love him.. he’s fantastic. Be well… Best… Carol
I was just diagnosed with MSK last Friday. I have had a bout with stones in 2010 that was a month long of in and out of surgeries. The urologist NEVER mentioned MSK. I have not been feeling well and was diagnosed last week on Tuesday with a UTI. they gave me antibiotics and I progressively got worse wiht my abdomen pain increasing . Went to the ER and after a catscan without contrast the doctor asked if anyone has ever talked to me about my kidneys and the fact that I have MSK. Then he sent me for an ultrasound. they stated I have systs on my kidneys, but they should not be causing me pain. they sent me home stating I must be fighting a virus and gave my tylenol with codine. The prescription has not helped with my pain factor. I am still feeling bouts of pain. I have a follow up with my pcp whom i sent all the results from my er visit. She had to look up MSK as she is not familiar with it. Is it possible I have stones again, but they cannot see them with the tests they have administered? Just for the record I have no apendix as that was removed in 1998
Hi Loretta, MSK is hard to diagnose, but with or without it you must have multiple stones in your kidneys and that is a problem that should be treated so more to not form. Pain from small stones is definitely a real thing and a current research focus. The problem is whether surgery to remove the stones makes things better or not. If your PCP does not know about these matters perhaps she can refer you to someone who does because prevention is really not so simple. So, given what you have written you do have stones, and they are multiple – thence the diagnosis. Here is a good plan for prevention. Take a look and see if your physicians can help you with it. Regards, Fred Coe
Thank you for calling MSK what it really is, a disease….
Hi.
I was diagnosed With MSK this monday With CT after serveral UVI’s the last years. As far as I know, I’ve never had kidney stones (the doctor Also Told me so). I’ve had flank pain, but after starting drinking 2L wather each day, the pain is gone. This disease is unknown for me, and Im really scared about this. Im only 22, is IT possible that the pain will be worse when i Get older or start having kidney stones? And is it dangerous going trough a pregnancy With this disease? Can I Get a kidney failure? I going to the hospital in November to Get some more information about this, but IT feels like a very long time..
Hi CB, MSK is often diagnosed by CT scan findings of many crystal deposits in the kidneys – nephrocalcinosis. But that is a very unspecific finding and usually not MSK but the more common calcium phosphate stone disease that is specially common in young women and due to high urine calcium – hypercalciuria. Treatment is important and very straightforward. Blood and 24 hour urine testing are paramount. Given the nature of the CT findings you do have calcifications in the kidneys even if you have not passed stones so treatment is much the same as if you did pass them. If MSK is present, it still is a disease with crystals, so treatment is important – and also much the same. Kidney failure is rare, and pregnancy is not a major issue at all if you have normal kidney function and blood pressure. Regards, Fred Coe
Hi CB!
I’ve had MSK for approx. 14 years. I’ve had 3 vaginal births. I love my kids! Before I had my 1st baby, I passed a kidney stone at 9 weeks pregnant. If you begin shaking for no apparent reason and have the chills, don’t fret because those are the symptoms I had before I passed my one and only kidney stone. Do call your doctor right away!
I still have kidney stones, but I make sure I drink plenty of water.
Hope this puts your mind at ease, CB!
Your read was full of good information. I had my first kidney stone 21 years ago which caused my first daughter to be premature. I have had them every since. I was diagnosed in May of this year with having MSK. I produce 6 mm + stones on a regular basis. I have lithotripsy at least 3 times a year. My Urologist is amazed at the rate I produce kidney stones and not just a kidney stone but large ones at that. I am in the hospital when the pain gets too bad for me to take. I have fever and vomiting most of the time. This has effected my life through finances, emotionally, and physically. I am very tired of the Dr. not knowing what to do other then waiting for the next one to come. I don’t want to be put to sleep so I don’t have another blockage. I have insurance but of course they don’t pay 100% and when your in the hospital as much as me then bills add up. I wish there was more that could be done to help me. I not only don’t like going through this but hate what it does to my family. Any suggestions would be greatly appreciated.
Hi Debrah, I am never amazed at stone production rates having seen hundreds or more produced and having published about it over the years. The problem of prevention is the same for one or one hundred stones. Here is my favorite guide to how to get it done in an orderly way. It is usually very effective in people with a lot of stones, and easy to be sure about because of the many stones. Regards, Fred Coe
Debrah,
When i read your comment my jaw dropped since you are the first person that i have come across that has the same story as me other than i havent been officially diagnosed with msk yet. Its a sad but happy feeling hearing someone knows exactly what i have to ho through ALL the time. Thank you for sharing!!!!
I have passed several kidney stones, had lithotripsy x 2, ureterscopyx1 with stents. My ct scans show several stones bilaterally at any given time, and last few years with medullary calcium deposits, probable medullary nephrocalcitosis and possible MSK, but then nobody ever looks further . I also have been having left flank and lower abdomen pain last 6 months when I’m not passing a stone. My question is … is this new pain from the calsitosis?
Hi Debbi, Of course the pain could be from crystals passing or stones in the kidney. The problem is treatment. It is unclear if surgery to remove small stones or medullary calcium deposits will improve pain, because there are no trials as yet. So surgery should be only if pain is very disturbing. Prevention of more stones is crucial, and if you are not already getting it here is a good guide. Regards, Fred Coe
Very informative! Thank you! None of my doctors knows much about this disease. My first kidney stone was diagnosed and removed (before litho) when I was 16, but I was not diagnosed with MSK until I was pregnant with my first child. My stone burden increased dramatically throughout both of my pregnancies (appx 21 stones passed during each), and I had blockages and sepsis several times. Potassium citrate helped reduce stones for years, then my bladder got involved….and I was diagnosed with IC in 2012, with an “end stage” bladder at this point. I am s/p bilateral nephrostomies, partly because of obstructing stones, but also due to bil, hydro from my kidneys storing urine for my diseased bladder. My EGFR has risen from 33 to 57 with the nephrostomies (x 2 years) and I have my life back for the most part. I now am relatively pain free, yet over the past few months IR has been noticing “crusty” tubes even noting that one tube was stuck to the side of my kidney (crystals). This was NOT a problem previously and I do not know how to resolve the problem. Citra-K helped for years, but I was told to D/C it due to bladder issues. I drink copious amounts of water. I do have a problem with oxalates, and have been told to avoid fruit due to IC. Both ureters are scarred and damaged, and I have a significant stricture on the right side. My left kidney only operates at 30% capacity now, due to repeated infections. The many urologists I have seen have been unable to help me given the complexity of my two conditions. Nobody seems to want my case, although I have a great attitude, practice alternative healing and come across as healthy. Bladder removal has been recommended by several, but as of yet, I have refused. A bit frustrated at this point, but trying to stay optimistic. Any guidance would be appreciated. Meredith Easton Mendes
Dear Meredith, these are serious issues. The crystallizations on the tubes means that urine saturations are very high and need to come down. The tubes create lodgment for crystals and drainage of urine is not normal. Citrate is helpful in stopping crystals on tubes and I do not see why you should not use it. I know of no data linking potassium citrate to interstitial cystitis. As for obtaining needed care, you would pose a tremendous challenge to any urological group. If you are indeed having difficulties finding care, please email me personally so I can try to help you identify physicians who might be of help. My public email associated with the site is flcoe@uchicago,edu. Regards, Fred Coe
I was diagnosed with MSK in February in one kidney. I was just diagnosed today with both Kidney’s having MSK. I have chronic pain from both. I have found that vitamin water helps with the pain and flushing the kidney stones. I am not sure what the proper course of treatment is. I have regular painkillers and anti-nausient medication. I was also advised to not drink alcohol (which i don’t already, so go me) and to not have any caffeine (I have acid reflux so I gave this up). I don’t know what else can be done for me. I am being referred to a specialist and also to get a ct scan. What does treatment look like? The pain and nausea is awful. I have a history of multiple bladder, kidney, tract infections each year, also stones in the last two years.
Hi Stephanie, If indeed you have MSK there is anecdotal evidence that unroofing the large cavitary cysts may be helpful – as was done in this case. There are no trials. All aspects of stone prevention that reduce supersaturation should be helpful – the stones appear to form because of stagnant flow in the cysts. Regards, Fred Coe
Hi Stephanie I seriously could’ve written this. I was diagnosed as well in February with MSK in my right Kidney. It is now confirmed in both my left and right. I am on pain medical and anti nausient medication as well. I have had a lengthy history of tract, bladder and kidney infections since I was three. I also was advised no alcohol (go me I don’t drink) and no caffeine (already gave up due to heart burn, this was tough though as I was a caffeine junky). I also have hypothyroidism and PCOS. I am in constant pain.
Hi Stephanie, Thanks for writing. I hope that you are pursuing as much protection as possible against more stones. Take a look and be sure. Regards, Fred Coe
Thank you very much for this excellent article. Would it be ok if I printed it to discuss with my urologist ?
Once again thank you. Very well written and informative
Take care
Hi Tasha, The site is free to the world, and people are free to print what they will. Regards, Fred Coe
Thank you very much for the great information. I was diagnosed with MSK over 20 years ago and have many stones combined in both kidneys. I also have a double collecting system bilaterally. Are you aware of any correlation with the two or any further complications ahead I should be ready for?
Hi CD, There is a modest association of MSK and anomalies of the urinary collecting system. But more or less what you have is what you will have in that the abnormalities were present during development. The big issue of MSK is prevention of more stones, and I have alluded to how to think about the matter in the case report. Regards, Fred Coe
I’ve had lithotripsy twice in the past 10 years for 6+mm stones. I’m passing smaller stones on a regular basis tho. After much research, I’m just now learning of MSK. My urologist has never mentioned it. I’ve passed at least 9 stones in the last year (either from visibly seeing them myself or by CT scans/x rays showing them one month then gone by the next). I’ve had monthly horrible pain over the past 2 years in my lower right back and lower pelvic area. It hurts after I urinate daily. No STDS, no infections, no urgency to pee. I have blood in my urine at my exams. I’ve had a 24 hour urinalysis recently and was wondering if there any “tell tell signs” of that test for MSK.
My stones have analyzed as calcium oxalate by the way.
Hi Shana, The 24 hour testing has no role in diagnosis of MSK which is a disorder of kidney structure. Take a look at how to read your 24 hour test. Also take a look at how to get prevention for yourself. It is a process and testing is just one part. It will work. Regards, Fred Coe
I was just told that I have calcifications throughout my entire kidney. I have pretty severe constant flank pain, constant blood in the urine, and nausea. My kidney function is still on the acceptable end, but everything else, symptom wise, is pretty horrible. I don’t feel that I got very much information on what this entails. Is there anyway you could inform me a bit more?
Thank you.
Hi Shay, Given multiple calcifications in your kidney(s)? and pain, you may have any of a number of diseases. So what you are asking for is a way of thinking about the causes and prevention of the stones. Here is a good entry point, and it points to a number of articles that may help. As for the pain and nausea you may be producing and passing crystals, tiny stones, some combination of these, and your physician needs to figure out if that is happening. If so, then the article I pointed you to is ideal because all about the path to prevention of more stones and crystals. Regards, Fred Coe
Thank you so much for your response! Basically, what I was told, was that my kidney tissue density was abnormal, and that there is calcifications everywhere throughout my kidney, and that that was more of a “kidney disease thing”, and I was referred to a nephrologist.
I can’t get into him for a few weeks, and with that being all of the info that I got, I still feel very in the dark.
He also said there were no stones.
What does that mean in your opinion? I feel so confused! The pain, and general malaise is disheartening to say the least, and feeling confused about the little that I was told is frustrating!
Thank you so very much for your time.
Shay
Hi Shay, The combination of multiple calcifications and increased kidney tissue density on ultrasound – I would imagine that was the test method – points to one of a few alternatives I am sure your physician is considering. This is not rare with primary hyperoxaluria, renal tubular acidosis, and Dent disease, to name the more obvious alternatives. Your nephrologist will no doubt be expert in all of these and help sort things out. It is very important to do so in order to stave off further kidney function loss as best is possible. My site is not as yet fully done so the main systemic diseases are yet to be written up. Let me know, Regards, Fred Coe
I have been diagnosed with MSK and a nephrologist told me that it won’t kill me, so don’t worry about it. My urologist says, “just drink lots of water (no coffee, tea), watch the vitamin C.” Now I stumble onto your website and find I have to watch literally everything I put into my mouth in addition to drinking of fluids – and oh, by the way coffee and tea aren’t bad after all. First of all, I am annoyed that doctors seem to be so incredibly clueless and this is their job for goodness sake! Why hasn’t anyone told me this stuff before? Meanwhile we just moved which is giving me the opportunity to find a new set of docs. How do I go about finding someone who takes this seriously and is in the know? (By the way, my urologist was shocked when he went in surgically to get out a stone – this was an ER middle-of-the-night attack – and found “my tubes” are so narrow he didn’t think I could have passed the 2mm stone)! Should I be seeing both a nephrologist and urologist? I just read a study Aug 8, 2016 (Univ of Houston, Univ Pitt, Litholink) http://www.sciencedaily.com/releases/2016/08/160808115447.htm>. on hydroxycitrate which dissolved stones. I’m ready to be the human guinea pig…
Hi Carolyn, There is a real lot here. First, do you really have MSK? The article points out how hard that is to know. You need a proper evaluation to figure out why you form stones, and here is a nifty five step plan. Be sure the stone is analysed – there are potential surprises here and guessing is not a good plan. As for hydroxycitrate, it is in numerous health foods, may or may not be useful for stones, and is presently in a kind of limbo. Dr Asplin was my protege and is my close friend so I do know the paper well. There is no reason to believe it will dissolve human stones in people – that is just an imagined possibility. There are no trials as yet. Regards, Fred Coe
I was diagnosed about 2 years ago with MSK on one side. I was having terrible pain in my back and abdomen, went to my family doctor, was misdiagnosed (humiliating experience) and spent a lot of time in pain and finally ended up in the ER. A CT scan found from my urologist found the MSK. There really wasn’t a lot of followup from my Dr., it was pretty much. “Well, you have this sponge kidney and it’s causing you to have lots of tiny sand stones. Good luck with that, drink lots of water.” Now it seems every few months it flares up and I have a lot of pain, and sometimes a UT infection or kidney infection. I can deal with the pain, but I don’t understand why I keep getting the infections. I am glad I came upon your website with so much helpful information and comments from other people dealing with the same problems.
Hi Sherry, MSK is very particular and hard to diagnose from CT. You may have it or many other forms of stone disease. As for anyone with stones, follow a plan, and here is mine. I am sure one of your physicians will seen you through this rather simple set of tests and help you begin prevention so you do not make these stones. It is important. Likewise, I am sceptical about diagnosis of MSK from routine CT; perhaps they did more than the usual but most of the time the diagnosis by CT is uncertain. Regards, Fred Coe
Sherry,
I have had many similar issues (included the infections). Surprisingly, I have found a lot of relief through diet – for both pain and flares. I was diagnosed with MSK about 6 years ago, and was given what seems to be the typical “it won’t kill you, so just drink enough water and you should be fine” answer from the urologist I was seeing at the time. Needless to say, my problems continued to persist, so when I started college (I’m apparently an early bloomer for MSK, diagnosed in high school), I began looking for ways to help myself. I found a good book at the library – “The Better Bladder Book” by Wendy Cohan, RN – which I recommend to all my ‘kidney/bladder friends’. It’s not the complete answer to everything, but it helped me get a better sense of control about what my body was feeling, and what I could do to help it. I wish you good luck, good health, and low flares 🙂
I have a few questions. I’m a military wife so we move a lot. I was diagnosed 5 years ago and since have been able to control new stone formation and UTI’s pretty well. I have recently in the last year developed RTA. My current dose of potassium citrate to treat the hypokalemia and help with stone formation is 80meq. Is this a common dose in MSK patients? Is there a point where Nephrologist’s will stop increasing potassium due to safety concerns? My potassium in labs was recently 3.4. Also we are moving to Omaha, NE and I really struggle finding a nephrologist who understands MSK well. Is there anyone you would recommend? I also have hypoparathyroidism due to a thyroidectomy. This complicates my diseases immensely. I would love any recommendations on any of this info or referrals. Thank you!
Hi Jennifer, RTA is not usual in MSK, so I suspect you may indeed have RTA as a main issue and many crystal deposits in the kidneys that have led to the MSK label. Is your low potassium because of diuretics or because of your kidney disease? Did you need the citrate because your blood total CO2 was low? If you indeed have RTA with – I presume calcium phosphate stones – management is very difficult. You would be best off seeing someone who is really expert in prevention. The main approach- for real RTA – is to lower urine supersaturations as much as possible by whatever means is most effective and least intrusive. My best advice, if it is RTA, is to come to us at University of Chicago as the closest stone center to Omaha. As we are professors we have no significant financial incentives and I can feel free to make this suggestion. If it is a more routine stone issue I would simply find a good local nephrologist or urologist who has an interest in stone prevention. Regards, Fred Coe
The MSK diagnosis came several years before the RTA diagnosis. Though who knows which actually came first. Since I started passing stones at 19 they long suspected MSK but didn’t diagnose it until imaging supported it. Again I don’t know if it is an accurate diagnosis or not. I’ve never drank, I’ve never smoked, I rarely drink soda and I drink around 50oz of water every day. Sometimes more but 50 is my daily goal. I started needing potassium citrate within months of my hypoparathyroidism diagnosis. however a few years later is when they put me on HCTZ 12.5mg twice a day due to my calcium issues with the hypoparathyroidism. my HCTZ dose has never changed in the last 5 years but my potassium citrate is frequently being increased. Is there a diuretic that is potassium sparing that would still recirculate my calcium that i can ask my doctor about. I currently take 80meq of potassium citrate daily. i have had calcium oxalate stones in the past. I get frequent kidney/flank pain but i just suck it up because i have been told doing a urteroscopy can cause more complications than it helps by my urologist. I do also have significant nephrocalcinosis. I don’t know how it would work to try and come see someone in Chicago but it is worth considering if it means I will get appropriate care. I’m not necessarily as concerned with the stones. Either they pass or they stay but either way its fine. I’m more concerned with the electrolyte absorption and the frequent flank pain. I have also had my renin tested a few times. The first time it was 4.8 first thing in the morning and i was laying for the test. The second time it was 7.5 and again laying for the test. This has been very concerning to me but nothing has really been done for it and it hasn’t been checked again in 10 months. My aldosterone has also been high too first time was 29.3 supine and 18.1 supine. My first in the morning cortisol levels are very low but the cortisol infusion study showed a proper response. I am pretty medically savy but I am at a loss with this stuff. I often throw up due to flank pain but it is rarely ever a UTI or kidney infection. Anyway, contact information would be appreciated and i will look into whether i am able to come up there with my insurance.
Hi Jennifer, I wrote to you directly concerning this complex matter. Briefly, it sounds like thiazide, given to stabilize serum calcium reduced by hypoparathyroidism, is causing potassium wasting. Perhaps RTA is also present and worsening matters. See my personal email for more. Regards, Fred Coe
Hi… I have Medullary Sponge Kidney in both of my kidneys. I have had 3 lithotripsy procedures, multiple surgeries to remove stones, gotten bad infections, so many CT scans, pass a lot of stones on my own for about 16 years. I travel with my family and have to go to different hospitals and some Dr’s don’t even know what MSK is. Is there new research and study’s going on to help people with MSK. I do have pain sometimes and don’t pass any stones. Doctors tell me that there is nothing wrong, its something else not your kidneys. Is there a website to follow on any new findings on how to help us? Thank you for any information you can suggest or pass on. I would be willing to participate in any clinic studys as well.
Hi Michele, Is it really MSK? For example are your stones brushite or apatite? Have the physicians who have removed stones seen the MSK abnormality directly when in your kidneys? MSK or not prevention is much the same, so see if you have been fully evaluated and treated – here is a reasonably good summary. No one thing will prevent stones, it is a matter of making all needed changes, and when that is accomplished stones will be much reduced in most cases. Be sure that surgeries are necessary – many of your stones may be in kidney tissue and not movable, for example. Regards, Fred Coe
I had an ultrasound a week ago on my kidneys.
It says the following
impressions was bilateral medullary sponge kidney with evidence of nephrocalcinosis and small nonobstructing stones.
I have been in pain in my right kidney for a few weeks now. Does my diagnose cause pain? My urologists skips the part of the ultrasound that says I have medullary sponge and doesn’t ever mention it.
Do I need to see a neurologist instead?
Hi Angela, You need to be evaluated and treated to reduce new stone formation. Your physicians can provide what you need. Here is a good plan for you. MSK can cause pain because of stones and infections; stone prevention and treatment of infections are in order. I am sure your physicians will want to see to that. A neurologist does not seem appropriate. Perhaps your urologist might want to revisit your issues or recommend an alternative physician for you. Regards, Fred Coe
Hi. I was diagnosed with MSK in 1999 when I was 25 weeks pregnant, when they found an 11mm stone in my I refer causing hydronephrosis. They inserted a nephrostomy tube for the remainder of pregnancy. After that I have had 3-4 lithotripsies/year and one ureteroscopy with laser and stent placement over the next several years. I was diagnosed, about 2 years ago with moderate nephrocalcinosis. I had a kidney biopsy that showed that my diabetes and lupus are affecting my kidneys as well. I have had several tests done with have said I had MAN and nephrocalcinosis such as IVP, uktrasounds, CT with contrast etc. I am currently waiting to get back in to see my nephrologist as I have had constant pain that has several degrees of pain and a burning sensation in right flank as well as sharp, intermittent pain in left that radiates to front and down groin and in thigh. I have had protein and hematuria non stop for many years as well as constantly testing positive for microalbumuria. Do you think that this laser roofing would be beneficial for me? Thank you for this article. Very informative
Hi Denese, I am not so convinced about MSK; it sounds morel like other kinds of stone disease. Diabetics often form uric acid stones. Do you know what your stones are made of? Diabetic and lupus nephropathy together pose quite a complex issue – stones being perhaps the easiest part. I would try to avoid shock wave lithotripsy in favor of ureteroscopy. As for laser unroofing I am sceptical as some kidney tissue is lost and you may have impaired function. Regards, Fred Coe
Hi Doc. Can true extreme cases of MSK have the Mag 3 with nuclear and lasix? Also do MSKERS form calcifications elsewhere such as spleen, lung ect? Much thanks…. Carol
Hi Carol, MSK is a localized renal developmental disorder but has some genetic underpinning and possibly cysts elsewhere. I will refer your question to my colleague Dr Arlene Chapman who is an expert in cystic diseases and see if she can add. Regards, Fred Coe
Hi Carol, Dr Chapman knows of no calcifications in other organs in patients with MSK. The procedure you mentioned is appropriate. Regards, Fred Coe
Can you have MSK and have Kidney pain without a blockage?
Hi Faith, I am afraid many people say so, and I believe they are right. Whether pain is from microscopic obstruction within the sponges, infection, inflammation, or all of these we do not know. How to treat is controversial as the article says. Regards, Fred Coe
Hi Dr. Coe,
Thank you so much for the information. I am 45 y.o. and was diagnosed with MSK as an incidental finding on a CT scan 7 years ago, but was told it was nothing to be concerned about. My only potential symptom is that I have had recurrent UTI’s and possibly since early childhood. I also have recurrent bladder pain and spasms that are worsening as I get older. Are these possibly connected and is this something I need to investigate further if these are my only issues?
Thank you again.
Hi Paula, If the CT was not with infused contrast, the diagnosis is suspect at best. But someone saw a lot of calcium in your kidneys. The only bladder link beside infection would be crystal formation. I would ask your physician to look. Likewise given kidney calcium deposits you should have a proper evaluation. Regards, Fred Coe
I was diagnosed with MSK 3 years ago following a .8mm stone at age 67. My doctor referred me to a nephrologist who did the week-long urinalysis and prescribed potassium citrate er 10mEq, which I have been taking since then. However, the doctor never did any follow up, except to ask me if I had any kidney stones about a month after starting the prescription. My concern is long-term effect of the pot cit, how it has changed my blood chemistry, bone density, etc. I have asked my gp for a referral to a nephrologist in her practice. What questions should I ask them? What tests should I have? Thanks!
Hi Barb, It sounds like not everything was done in order. Here is a good plan – check it out. Here is an article on how to get the most out of your next medical visit about stones. Let me know, Regards, Fred Coe
This article is great. I have been given an “unofficial” diagnosis of MSK. A CT Scan showed what they officially diagnosed as nephrocalcinosis and both my urologist and nephrologist jotted down “medullary sponge kidney” on a notepad and verbally told me they think I have it but no official recordings of it anywhere. You can imagine this has lead to frustration with all of the information out there that can be alarming. Since dx (late last year/beginning of this year) I’ve passed one stone on my own, and am currently treating a UTI for the third time in six weeks. A kidney ultrasound showed a “shadowing” according to an er doc that could be either a lipoma or a stone; I need to follow up with the doctor to find out. It’s frustrating to be told you “might” have something when I want to treat what I actually have! Thanks for your knowledge.
Hi Marykate, Neither a CT not anything else but an infusion study can make MSK clear, and that is fine. Prevention of stones is much the same – you should be sure to get fully evaluated – here is a good plan. As for your physicians, they are busy – here is a tips page about how to use your visits. If you had a recent CT shadowing on an ultrasound is not important – malignancy detection via CT is very exact. As for stone vs. lipoma, ultrasound has the basic problem of uncertainty – the only benefit is lack of radiation. I would not get repeated CT scans but rather put my energy into prevention as noted above. Regards, Fred Coe
Are MSC and high blood pressure connected?
Hi Rosa, Kidney stones and high blood pressure are connected, so MSK may well be. In any event treatment is as for all high blood pressure – low sodium diet, aerobic exercise, weight loss and then meds as needed. Regards, Fred Coe
Are the affected kidneys larger than the normal? Can a cyst be 50-60 mm large?
Hi Rosa, Yes they can be. Usually cysts are not so large on routine x rays. Be sure what the radiologist said; there are marked difference between medullary sponge kidneys, simple kidney cysts and other forms of kidney cyst diseases. Regards, Fred Coe
Radiologist said i have medullary sponge kidney and cyst with that size-50-60 mm. Is that possible?
Hi Rosa, I presume you have two issues, MSK and a simple but large cyst. Prevention of more stones would be the same with or without the cyst. Be sure you are getting all you can to reduce new stones. Regards, Fred Coe
Thank you.
I am known to have MSK, having been diagnosed in 2011, after a 10years of symptoms.
I also believe that in the past I was diagnosed with renal hyper-acidosis and given K+ citrate.
After multiple blood tests and urine collections, I had a trail on bendrofluazide , but had to stop as I kept having dizzy spells, have always had a blood pressure on the lower side of normal.
I have managed my pain at home, with simple analgesics and have been fortunate in not having UTI’s .
My concern is that recently my Family doctor started me on clonidine 0.2mg patches weekly for symptoms arising from the menopause, hot flushes and insomnia .
I started the treatment with a single .1mg patch but as this had not controlled my symptoms increased the dosage. I then developed increased flank pain with microscopic heamaturia , unable to control the pain myself ended up in ED on oral morphine.
I had a repeat CT scan, 3 days after the pain had settled which showed bilateral punctate and rodlike calcification in keeping with known MSK, apart from a growing simple renal cyst nothing else was reported, no renal or ureteric stones no dilation..
The presumption is that I passed the stone, however now 7 days later I am again in pain in my flank, not as severe but troublesome.
So, despite widespread reading I can find no evidence that clonidine alters the behaviour of MSK, what are your thoughts?
Many thanks
Hi LIsa, Clonidine has no obvious effect to cause kidney pain nor create new stones. But urinary bleeding with flank pain is most likely stone passage or crystals. That the pain persists means something urological, and I am sure your urologist can find the cause. Of course, stop the clonidine as it was a comfort medication – perhaps something has changed because of it and the best way to be sure is to stop it. Being a central sympathetic blocker, the drug could alter ureteral dynamics and move fragments from the kidneys into the bladder. That is a theoretical idea with no trial data. Regards, Fred Coe
Thank you,
Dr. Coe,
My 14 year old son has chronic flank pain on both sides, and he is now starting to have cramps in his abdomen. In 2015 he passed a small stome. We have been to UVA and John’s Hopkins Pediatric urology and nephrology. Drs just tell us that he is either constipated or there is nothing wrong. He has had numerous CT scans and sonograms. that appear to be normal. We went to a local urologist who believes, based on his symptoms and with my husbands history, he has MSK. My husband was diagnosed with gross hematuria syndrom at age 18 and has had similar systems his whole llfe. Our primary care Dr gave him Tramadol to amange the pain. Do you know of any Drs on the East coast that could help us. I don’t feel that a 14 year old should be on pain medicine 3 to 4 times a month.
Hi Sally, Your son has had a stone, your husband had hematuria at age 18, now your son has repeated pain as your husband did. To me, this sounds like crystal attacks from idiopathic hypercalciuria in someone prone to crystallize – stone formers are like that. No one sees anything on CT but if they look at the urine during an attack they may see blood and crystals. Crystalluria, hematuria and pain are very common in childhood IH. Treatment is easy. Mention this to your physicians and see what they think. You have been to the best places. As for MSK, this must mean that multiple calcifications have been found on CT, or else the word is highly misused. Either way, your husband and son deserve full evaluation for stone disease; I predict hypercalciuria will be found – highly hereditary, and treated. Regards, Fred Coe
I have a question. I was diagnosed by a urologist about 12 years ago with MSK. About every 3-4 years I deal with kidney stones from it. Now i’m seeing a different urologist and start over every time I see him. So right now i’m dealing with an asymptomatic stone in my left kidney and having pain in my right kidney. I tell him its renal colic but get instantly shut down because there isn’t a stone there. I know whats coming because this is how my stones start (3-4) in a couple months. I have been to the ER and they say its my back which it isn’t. I showed them i can pick things up and twist and move my back and have no problems. I don’t know what this is and need help. If feels like renal colic every once in a while and felling of being punched in my kidney. do you have any suggestions?
Hi Gina, I do. Possibly you are passing crystals or tiny stones – has your urine been tested for blood when you have pain? Has anyone looked at it under a microscope for abundant crystals? Have you done 24 hour urines and if so do you have high supersaturations? Let me know – chack with your physicians. Regards, Fred Coe
yes it was tested monday and there was blood. he looked under the microscope and said he didn’t see anything. 24 hour urine was done along time ago and i don’t remember the results. i just know there wasn’t a lot of urine and the yelled at me for that.
I have had left pain in my side since childhood. I have been diagnoses with gravel like kidney stones. I have had many many passings or what felt like passings of kidney stones. I have also had a cyst found on my left kidney. During my second pregnancy over 12 years ago my left kidney couldnt keep up with the needs of the baby and the docs were concerned but it didnt show till very late in the pregnacy. Every time I go to the doctor I get met with the same things take this 24 hour usine test that either comes back fine because Im not haveing a major episode. I have tryed so many times to get help to figure out how or what is wrong and I get met with multiple dead ends. I want to go back to a kidney doc but it has to be aproved by my gp and he wont aprove it. I am in pain every day but some days are worse than others with attacks every two months of stones. I find myself going to the er when it is extremly bad and they say the same things renal collic stones . what should I do ??? thank you megan
Hi Megan, I guess the main issue is whether you pass stones or gravel. Have you collected any? Has any been analysed? Are stones seen in the kidneys? Without more, I have trouble trying to help. Regards, Fred Coe
gravel seen in the kidneys none have been analysed and trying to get them seems to be illusive.
Good day,
– 6 years ago I had Uroseps, all around right kidney, first doctors wanted to remove the kidney, but the day after they clean m abdomen and around kidney they sent me to CT and saw that kidney is working, so they kept me one month in hospital on so many antibiotics, and after manure was inside kidney they did some local procedure to take that out. I wear percutaneous injection.
– 5 years ago I was removed one stone from ureter without any complications.
– 4 years ago I was diagnose MSK by IUV I have my both kidney fulled with those little stones , and I had one little stone stoked in my right ureter, it was removed but during night on my release home I got uroseps. I wear JJ stent one month.
– Now my problem is that I have pains very often, and my urine have sometimes eritrocite and small amount of bacteria
– My Urea, Kreatinin, PTH, vitamin D, 24h urine are ok. I never had bad results when I do analyse. But my kidney are full of those stones.
I am 30 years old, dont have kids yet, I am looking for advice how to deal with this, and is it dangeurose to get pregnant.
Thanks in advanced!
Hi Andrijana, Sepsis is very dangerous and you are very fortunate to have done well. I doubt your 24 hour urine tests are really normal, unless your stones are in fact due to infection. Their analysis is very important. You need a real plan, and here is a lead into a good one. It is all about the stone type, what the 24 hour urine findings really were, and how to stop more stones. That is essential for you, having so many. If the stones are indeed from infection, you should have the problem fixed before pregnancy if possible. Regards, Fred Coe
Hi,
Thank for quick response. I had my stone analyzed 3years ago and the contentis: mostly VEVELIT (Whewellite): CaC2O4H2O then VEDELIT (Weddellite): CaC2O42H2O and a little n=bit of KARBONAHIDROKSILAPATIT (Carbonatehydroxylapatite):Ca10(PO4)5(CO3) (OH)2.
And in my 24h urine from October only Urea was under limits 157 (250-570)mmol/24h.
I started looking for opinions where ever I can, since in my country we dont have experience with this.
Regards,
Andrijana
Hi, Your stones are calcium oxalate. The key measurements you need are 24 hour urine calcium, oxalate, citrate, and creatinine. If you can get a complete 24 hour stone panel so much the better. Risk of stones increases when calcium is above 200 mg (5 mmol) oxalate is above 25 mg, or citrate is below 400 mg. Serum calcium must be normal or you have a systemic disease. Here is a good article about an evaluation. Here is one about your type of disease. Regards, Fred Coe
Thanks again!
This is very clearly written and explanatory, for which I thank you.
Can you provide any illumination for what “MSK: Polyarticular degenerative changes” would mean? I know what degenerative indicates; I think I’m trying to visualize “polyarticular”.
This is part of my most recent CT stone study (non contrast), and I won’t see my primary until 9/28 nor the urologist until 10/6. I’m just trying to visualize what the radiologist is describing and can’t, alas.
(That is the sum total of the comment under MSK heading, for the record, though the calculi and perinephric fat stranding are positively waxed over elsewhere in the report.)
Thank you in advance.
Best,
Lucy
Hi Lucy, you refer to the radiological report. The degenerative changes refer to your spine. The MSK impression can mean nothing at all as a non contrast study cannot differentiate MSK from many stones. The stranding means recent obstruction. You need full evaluation for the causes of your stones, and prevention treatment. No one knows if it is MSK except with contrast or after a ureteroscopy when they can look directly at the kidney papillae. Regards, Fred Coe
I am so sorry not to have been more complete.
I had a ureteroscopy and basket retrieval of multiple calculi through Wake Forest in 2011. (I had my first contrast (IVP) through George Washington in 1995 followed by lithotripsy.)
I was supposed to follow up with urology with Wake in 2012 but got caught up with other stuff and frankly put it out of my mind since no stones were moving, though due to a bout of severe gatroenteritis I have one high-res CT study (can’t remember if it’s with contrast or without) somewhere around 2014.
Now the stones have made themselves known again, and they’ve grown and multiplied in my neglect, if I understand this report properly.
But thank you. I’ll see my primary and the new-to-me urologist soon.
Thank you for such an insightful informative article. I have a question, I have what is being labeled as MSK via ultrasound, but I think nephrocalcinosis is more appropriate because the cause is either the period I had high serum calcium due to hypervitaminosis D, or due to kidney injury from iodine contrast administed for CT pulmonary embolism evaluation. Or both since both occurred same month. Is it possible to develop calcification in the areas injured/burned by contrast?
What can I do to prevent further calcification? I got the advice to consume lemons and citrate but my understanding is if the calcifications are phosphate the opposite would be needed I would need to acidity my urine while lemons make the urine alkaline? I would be grateful for any advice in my case. Thank you.
Hi Mrs K, I gather you have renal calcifications of unknown composition and have had a bout of vitamin D intoxication. The latter can indeed cause the former, whereas contrast may reduce kidney function but does not cause calcifications. I would be fully evaluated for any causes of stones or calcifications and reverse any remaining issues. This is my best guide article. Never assume the cause, test and find out. Regards, Fred Coe
Thank you for a quick reply! I have been tested for other possible causes but nothing else has been found. All points to the very symptomatic and blood test confirmed vitamin D intoxification, if it is indeed calcification from that bout what is your guess as to the composition of the calcifications and which approach (medicine, diet) should I take to reduce and preventing further buildup? Early on I found lemon water increased my renal colic, and the urine was milky when it was alkaline after a calcium rich meal (turned clear when vinegar was added to the turbulent urine). Does this sound like phosphate calcifications?
I have a hard time finding any info on how to deal with this from Drs or tbe internet. If you have any insight i would greatly appreciate it. Thank you.
Hi, Your whole story worries me. Vitamin D intoxication would produce calcium phosphate stones and tissue calcium deposits. On CT the two cannot always be told apart. As for your crystal story, it suggests high urine calcium excretion with calcium phosphate crystallization as urine pH goes up from the lemon. You have said your evaluation has been complete and normal but I am not so sure that is correct given the crystals. The vitamin D intoxication would have raised your urine calcium massively and your blood calcium also could have risen but if that is over both should have become normal. Ask your physicians to reconsider matters, perhaps. Regards, Fred Coe
Yes what I desribed has normalized soon after and has remained normal since. Calcium levels are nomal now both in urine and serum. Now I am just left with nephrocalcinosis in kidney. And trying to figure out if the calcification as a result from that episode can be reduced/dissolved with dietary changes (low calcium diet, eating food that make the urine perhaps?
Hi, I doubt that can happen. But the presumed calcium phosphate crystals are still an issue; why do they form. Would you share your actual urine calcium and pH values, and urine calcium phosphate supersaturation? At best lowering supersaturations might put off more papillary calcifications. But vitamin D excess can cause medullary and even cortical calcifications that would be more or less indifferent to urine chemistry. Regards, Fred Coe
Thank you so much! I really appreciate you taking the time to read my questions and respond. I will get a copy of my results and post them for you at a later time, I would very much like to share them with you for your opinion. If this type of calcification is indifferent to urine composition does that mean it shouldn’t worsen over time? I really wish there was something more I can do to undo the damage, it might not be perfect but do you have specific recommendations for phosphate stones? Because if there’s a chance it will help, I’ll take it. I have read your insightful article on supersaturations and will act on that for now. Thank you once again!
Hi, Tissue calcifications in the papillary ducts – exposed to urine – can serve as anchored surfaces for new stones. Crystals in the interstitial spaces – between tubules – cannot form stones and are indifferent to urine conditions. Phosphate stones and calcium oxalate stones are treated alike, almost. Regards, Fred Coe
Turns out my Doctors never did the saturation tests, they just always ran a basic urinalysis on the urine collected. He also said he won’t order it since I don’t have stones. Is there a lab that can do these tests without a Drs prescription? Like an at home/send in test… Wish I could get this test on my own directly from the lab as needed.
Hi, I am afraid present laws make physicians indispensible. I would chat with my physician about getting a proper evaluation. If he/she is not interested perhaps someone else can be recommended who is. Best, Fred Coe
can you explain my mri result please “increase in bilateral renal parenchyma abnormality consistent with worsening medullary sponge kidney
thank you
Hi Marcella, Off hand, and without the details, I am afraid I cannot be of much help. Generally we never use MRI for stone work as one cannot see the stones. Possibly the stones are creating an artefact. This is one for those who did the test. Sorry I cannot do better. Regards, Fred Coe
Hi ,
Im a 29 year old female, ive had 64 lithrotripsys in 14 years. I currently have had a 27 mm stone in my left and a 9 and 12 mm in my right. Ive constantly had kidney infections and UTI. I have medullary sponge kidney disease. ive been battling this disease since i was 15, Ive had respectfully over 300 Cat Scans done. Im a traveler so ive had scans in many states, The radiologist in california and Iowa said no more cat scans unless its life threatening but doctors keep pushing it, to the point they refuse treatment unless i have one.
My question is, Should I be worried about the stone in my left kidney? Im in a ton of pain always, which they say if its in my kidney it shouldnt cause pain, but every time i bend or walk fast it feels like its grinding away the meat in my kidney. And I fall to the ground. Its been 4 months since i was diagnosed and no doctor will accept me, they keep sayin go back to my specialist in Iowa City. the pain management is terrible, my blood pressure is always 170/130 or higher, their solution is more blood pressure meds and anti biotics, well they recently stopped the anti biotics due to them not working anymore.
Im lost…
Dear Amanda, I cannot believe 64 SWL! Stop having them. If you have MSK they are useless. In general no one needs so many. You do not mention stone type, nor prevention efforts. Start here, because your case is a total confusion and not of your own making. As for CT scans, 300 sounds out of all bounds. My only hope is that your doctors in Iowa – I guess at the university – prevail. You need more consistent physicians, and likewise some repository of all of your records to stop repetitions. Most of all you need prevention. I advise home blood pressures as hospital readings may reflect pain and stress. Regards, Fred Coe
Thank you for extensive research and detailed article.
I apologize for below book; however, I find your article very interesting and pondering if I suffer MSK, as suspected, per below Renal Ultrasound report. Pls note, Ultrasound and CT performed due to suspected kidney stone(s); however, diagnosed with colitis; therefore, treatment for colotis priority, and I have not followed-up with regard to potentially suspected MSK, as MSK never mentioned to me at hospital, as I read report online via hospital patient portal.
Further, I have no recollection of any urologist advising I suffer MSK.
I am thirty-nine (39) yr old female; more UTI and kidney infections than I can recall, beginning at very young age (approx four (4) yrs old); multiple kidney stones past fifteen (15) yrs requiring surgical removal and ESWL; prescribed Macrobid daily, when pregnant (seventeen (17) yrs ago) due to UTI and Group B strep (diagnosed at only fourteen (14) weeks pregnant, nearly misscarried); blood present in urine EACH urinalysis past several yrs, despite negative for UTI.
I live in Houston, treated by several urologists in medical center; multiple physicians/urologists advise, I have extremely tiny bladder…one (1) urologist states, “smallest bladder I have ever seen”; urethra dialated at age nineteen (19).
CT Adb & Pelvis WITH contract and Renal Ultrasound at latest ER visit (unrelated to UT issues, as was diagnosed w/colitis at visit) reveal the following (and compared to prior CTs) CT Abd & Pelvis WITH Contrast (5/16/17): lesion in liver; “low-density lesions in both kidneys have become apparent with the appearance of multiplicity suggesting bilateral renal cysts. No evidence of hydronephrosis or perirenal edema.” -END.
Renal Ultrasound (5/16/17): “The renal pyramids are abmormally echogenic compatible with nephrocalcinosis.” Impression: Abmormal echogenicity of the renal pyramids compatible with nephrocalcinosis. This is typically seen in medullary sponge kidney.”-END.
Prior ER visit (unrelated to UT issues; same symptoms as above, 5/16/17 ER visit; however, colitis undiagnosed) CT Abd & Pelvis WITHOUT Contrast (4/14/16): “Punctate calcification is identified in the superior pole clyx of left kidney. Hazy calcification density is projected at the level of the papillae in right kidney compatible with nephrocalcinosis.” Impression: “Right renal nephrocalcinosis. Punctate nonobstructing stone in left collecting structures.” -END. No renal ultrasound at 4/14/17 visit.
If above is sufficent for you to answer question…Is above sufficent for MSK diagnosis?
If no, what additional diagnostic testing is required?
Again, thank you for the very informative article, all your hard work, and reasearch.
Hi Randee, I doubt that you have MSK given your results. What I would advise is a complete study to determine why you make stones. Colitis itself can promote stones. Here is my best overview about how to proceed. Regards, Fred Coe
hello, my name is maddy. im 19 years old and for a log time i have suffered with kidney infections and kidney stones. i was just recently seen about this problem and diagnosed with MSK. however im not sure if thats what is really going on with me. another question i have is can having MSK cause infertility? my fiance and i want to have a baby in the next two years or so but im not sure if i can. ive sone alot of research and cant find a correct answer for this question. can anyone help?
Hi Maddy, Stones in youth usually have obvious reasons. MSK is often over diagnosed. One needs either an infused CT or a direct look inside the kidneys during ureteroscopy. So I imagine you have lots of calcified areas in your kidneys and have been labeled. The key is to have proper testing and prevention. Here is a good way to plan. Get tested and get on a prevention program. As for fertility and pregnancy, in general stones do not have an effect. Regards, Fred Coe
Hi dr Coe,
I was wondering if you could help me out. About 5 mths ago I had a uti, that went to a kidney infection- dr thought I had a stone but I had a ct scan and no stones were found. But they picked up a large fibroid in my uterus. I have microscopic blood in my urine during this infection, it then cleared up but I seem to be getting worse. I have had about 5 ultra sounds suggesting msk or nephrocalcinosis. My last ultra sound suggested that I have 2 simple cyst on my left kidney. I have extreme anxiety due to all of this and my muscles and bones ache. Also I feel that my thyroid gland randomly swells up and down. But my thyroid levels all come back within normal range. My bloods always come back normal. But I have randomly elevated Crp levels. My urine suggest ph level 8. Protein nil, glucose nil, specific gravity 1.011, leucocytes 4, erythrocytes 75( this was during my monthly cycle) squad epi cells 3. I have lost about 10kg in 5 months, not sure if this is due to depression and anxiety- I am now taking 10mg of an ssri- seems to help a bit. I also had a miscarriage in January and while I was in the hospital they said my potassium levels were slightly low and gave me a drink to help. I feel so tired all the time. And I feel that when I do eat, it seems I just need to go to the toilet and have loose motions. It’s like my body is not obsororbing any nutrients. Do u think I have msk and it’s all linked? I have never passed a stone before as I have herd the pain is really bad. I get flank pain and side pain- more when I have my monthly cycle. Or if I have apple cider viniger it tends to be more painful. But I notice my spine hurts too in the middle. Like a throbbing and burning pain. I am yet to see a specialist, I am at my wits end. Thank you again
Bliss
Hi Bliss, You have indeed had some trouble with a miscarriage and infection. MSK is a stone disease but it sounds like you are not clear if there are stones or not. If your CT was negative for stones they are not present as it is the gold standard. Ultrasound is far less precise. Check on the CT report. If negative go back over it with your urologist; usually a negative CT is the end of the stone story. Here is a nice article about confusion that may help you sort things out. By no means fret about stones if your CT is negative. Regards, Fred Coe
Hello, I have a friend who has this and she has it in both kidneys. She hasn’t been suffering from stones seemingly weekly at this point. She has to be in the ER more often that she wants. She has had 4 specialist and she likes the one she has now. But I don’t know I guess I am trying to find out on her behalf if there is some treatment she is missing out on or something.
Hi Andre, Perhaps she has MSK perhaps not; as the article points out it is hard to be sure about. If your friend is having stones weekly and has four specialists, prevention is not working well. Here is an article that may help her and possibly them, as well. Regards, Fred Coe
My fiance was just diagnosed with MSK, and it is so severe that the prefer to do a total Nephrectomy instead of a partial Nephrectomy as originally planned. He is only 27 and we are just worried about future issues and him only having one kidney left. Both urologists have said that if we did a partial it would only leave about 30% of a fully functional kidney anyway and they are worried it would just start to develop more stones eventually leading to a total Nephrectomy anyway. Also, he has a history of DVT and we are currently having issues keeping his INR at a steady level. As of today, his INR was a 1.5 and he has been on 120mg of lovenox q12° AND 7.5mg of warfarin daily x2 weeks. So, my concerns and dilemmas are would you feel comfortable taking an otherwise healthy 27 year old’s kidney? Would you be worried about clotting factors/bleeding out during surgery? Should we try to remove most of the stones and possibly a partial Nephrectomy instead of a full?
Please excuse my scattered thoughts, this has all been so overwhelming the past few weeks.
Hi Brielle, I would be horrified at removing a kidney that functions well just because of stones. Do not do this without seeking an opinion at a major university level urology program with expertise in stone management. I have never permitted anyone to remove a healthy kidney for stones. I never will. Regards, Fred Coe
I have MSK as my sons also have. One son is deceased not due to MSK. I had two sisters, one without MSK, her children do not have MSK and my oldest sister had MSK, all five of her children have MSK. I had an IVP and parathyroid tests as well as a 24 hour urine. It is definitely MSK. Some older ER physicians have told me I’m in kidney failure. I told these Physicians I am not in kidney failure and to check the pH of my urine because I can regulate the pH of my urine I do have microscopic blood and I will say that when you look at my kidneys with x-ray it does look pretty nifty to a doctor. It is obviously autosomal dominant in my family. If one parent has MSK then their children will have MSK. The treatment changes on who you go to see. I have been told recently to increase my consumption of calcium and not to take in any calcium oxalate foods or fluids. I refuse hydrochlorothiazide because I’ve done the research and Hydrochlorothiazide increases the number of stones formed but my youngest son has been told to take hydrochlorothiazide as well as some type of phosphoric acid medication and he has been told to limit his calcium which is the old way of dealing with MSK as far as what I’ve researched. I consider iced tea poison because I threw my first stone when I was in my late 30s but my sons threw their first stones when they were 18. They also love chocolate milk and obviously didn’t listen to me about not drinking ice tea or chocolate milk. It was frustrating whenever I would see that MSK is not hereditary because it is hereditary in my family. My kidneys look like marbles were thrown into my kidneys randomly but I am educated enough to understand that my kidneys are not in failure so whenever the emergency room doctors are not educated they come up with some crazy ideas like I’m in failure just because my kidneys look like they have about 40 or 50 holes in each kidney or marbles depending on what you want to believe. I have minimal blunting in my callyxes and I’m not sure I spelled that right but the last time I was told that was when I was in my mid-30s so I do know there is some damage. It is becoming easier for kidney stones to fall out of my kidney although I have not thrown a kidney stone that required surgery probably in the last 10 years I often throw what looks to me like tiny slices of almost see through isinglass if you’re old enough to remember what isinglass is. I don’t see where changing my lifestyle is going to change anything because I think I’ve done a pretty good job knowing that I have this condition and I also have problems with my spine I have had to have fusion surgery and at the time of my first three-level cervical spine fusion surgery I was told there were two more levels that would need work but the insurance companies won’t pay for an MRI I don’t know whether the two disorders have anything to do with each other although calcium could be a leaching from my spine perhaps because my youngest son also has disc disease. I have not had to have any procedures on my kidneys in quite awhile and that is something I’m happy about. I have delayed insulin response and I refuse insulin when I’m in the hospital because I know if I have a high reading I will have a corresponding low and if I’m given insulin I could very well go into what is commonly known as sugar shock. I am actually underweight for my age and I also have high fats in my blood and I was given cholesterol meds and I went into liver failure therefore I refuse any cholesterol meds. I’m not sure whether that plays apart in anything or not but I know of everything that I have my fusions cause me the most grief because of the pain. I had extremely high blood pressure because of the extreme pain and I am taking pain medication as per my doctor it sometimes scares me at my age to be taking pain medication especially with what’s going on in the news but I know I am not given any combination with fentanyl. For some reason when people overdose fentanyl seems to play a part. I just thought I would tell you in my family how msk is passed down and it is autosomal dominant but what is strange is if a mother or father has this then their children all will have it.
Hi Susan, Some reports exist of apparent familial MSK, as your’s appears. MSK has no immediate relationship to disk disease, or diabetes. High blood pressure is definitely linked with kidney stones. Kidney failure is very rare and usually from surgical complications. If stones are themselves causing pain one can consider ureteroscopic surgery to remove stones from the cysts, this is highly experimental, no trials, and should be done only in surgical stone centers of the highest quality – if at all. Regards, Fred Coe
Sorry I am not sure how to begin a new question so I had to start as a reply to this thread.
My son is 42 and has ulcerative colitis and MSK. Over the past 5 years his calcium oxylate stones are forming so quickly he is having lithrotripsy every 8-10 weeks. Intense pain at most other times as well.
It’s very debilitating and making his regular anxiety much worse as well.
I have been reading with interest the results of using fecal matter transfers to cure some case of UC. As no is sure if his stones are a result of his UC or MSK if they were because of his UC and this could be cured by the FMT could that technically cure his stones? Many thanks
Hi Wendy, Ulcerative colitis can provoke stones via dehydration and altered diet, so I would suspect it. Fecal transplant has no proven role in stone prevention; in ulcerative colitis I cannot comment. But lithotripsy every 10 meeks is excessive and he needs proper prevention care. As well, I would speak with his urologist about use of ureteroscopy vs shock wave lithotripsy if it is the latter that is being used. You do not mention 24 hour urine results or prevention efforts but that is where I would put all of my emphasis. As for MSK, it is often over diagnosed as the article states, and shock wave lithotripsy is not ideal most of the time. You seem very thoughtful, and I would recommend reading the articles on prevention – here is a favorite of mine. Regards, Fred Coe
Hi,
I was diagnosed with MSK in 2013 when I was getting a CT for a suspected gallbladder attack. They could find nothing wrong with my gallbladder but referred me to a kidney specialist because they saw that there was something abnormal about my kidneys. (I am not implying the issues that had me at the doctors for my gallbladder was infact related to my kidneys, they just happen to notice something was off at that time). The kidney doctor told me I had MSK but that everything looked fine and I had no sign of stones or plaque and that I may never have any issue or have ever known I had the condition had it not incidentally shown up on that scan. Fast forward a couple years I start getting intense pain on either side of my lower back when I need to pee but do not go (like at work when I try to wait 10 min for my lunch break) It is so painful I am in agony but is totally gone within seconds of voiding and the process of voiding is not painful. In addition I get dull achy pain in the same lower back on both sides that comes and goes and varies in intensity never getting unbearable and often going away for week or months at a time. When I revisited my kidney doctor I was told I probably just have back problems and need to see a chiropractor. I was told I might experience pain associated with MSK but that it would be because of the development of kidney stones would present in the same way kidney stones do.
My question for you, dose this sound like a reasonable assessment? If they are wrong and I am experiencing pain from MSK could I be causing damage by not investigating the source and taking some kind of action? and Finally is it possible to diagnose someone with MSK if they have no stones or plaque? all reports I have read including yours here talk about diagnosis because of the presence of these and the way they form.
Thank you for reading this and thank you for such a detailed report on MSK I have learned more from this page than I did researching all other sources combined.
Hi Ellie, In the absence of any kidney calcifications, I must presume the CT was with contrast infusion and visualized the actual sponge cysts. You should check on what was really found and how. If you keep having problems another plain CT without contrast and limited to just the kidneys may show some crystals, and if not I would be suspicious that the pain is otherwise than from stones. Regards, Fred Coe
Please help me find a Dr in Pittsburgh that is compassionate and understanding to this disease. I am so discouraged and falling into depression from lack of treatment by my existing Urologist. Heck, I would come to you if you felt like you could help me.
Hi, Julie, I found this physician at University of Pittsburgh. Kelly Victoria Liang, MD, expresses an interest in kidney stone prevention and trained at Mayo Clinic as a renal fellow. One of my very successful trainees in kidney stone disease is now a senior physician at Mayo and no doubt she would have benefitted from his knowledge. Her research is not in stones, but among the whole faculty there only she mentions the disease. I would contact her. Regards, Fred Coe