 Our newest venture – the Kidney Stone Prevention Course.
Our newest venture – the Kidney Stone Prevention Course.
It arose from this idea: Kidney stone prevention depends a lot on proper diet and fluids, which patients control. This site tells people what that diet and what those fluids should be, but not how to eat that diet or drink those fluids in real life.
They have to learn how.
So we built the kidney stone prevention course to help them learn.
Just as Raphael imagined generations of brilliant minds come alive together in The School of Athens (Raphael, 1509 -1511; Apostolic Palace in the Vatican.), we – on a vastly lower plane of existence – imagined and have, in the kidney stone prevention course actuated the knowledge on this site into real life.
The Missing Link
Physicians know this. You can’t learn to practice from a book – or a website. You learn from other doctors and then perfect yourself in practice.
In the same way, patients cannot learn how to implement a prevention plan just by reading. They need a teacher. Then they can perfect themselves over time.
Now you know my assumption, my working hypothesis if you want to be fancy.
Who Shall Teach Kidney Stone Prevention?
Physicians
Certainly. But how much, how long, in what detail?
Do I have an hour for this? For each patient? Food is a big topic, almost infinitely detailed. Thousands of choices in each food category. I say, we need 65 mEq/d of diet sodium. I point out food labels. Portion sizes. Problems of eating out, take in. My hour passes as a cloud in summer, here and gone again. My patient leaves and is not educated enough to practice wisely. Too little, too short a time.
In fact, stone experts at one outstanding kidney stone prevention center now offer courses to scale education. Perhaps this will become more common with time. Perhaps physicians cannot allocate time to courses within the stringencies of modern practice
Nurses
Certainly, but nurses encounter the same problems as physicians. Who pays? Where does the time come from?
Dietitians
Certainly, and as a prime part of their professional education and training. But most – perhaps almost all – focus on large scale issues like diabetes, hypertension, CKD, and obesity. Kidney stones occupy a niche. Even running courses, the few in that niche suffice for too few patients; the US contains millions of stone formers. To serve them in traditional nutrition counseling demands a great expansion of skills within the profession.
A Kidney Stone Prevention Course
Between the organized and precious skills of professionals and the clutter and sheer chaos of everyday life, let’s interpose public education aimed squarely at diet and fluids for kidney stone prevention – try this and see what happens. Moreover, let us use modern technology to lower cost and save time.
Scale
A course permits one person to educate many people. Social media and web tools scale a course: people need not convene physically.
Cost
Physicians, nurses, nutritionists sell their time. People in a course split the cost amongst them. This makes education more affordable.
Patient Time
An hour of education might require another hour to travel there, park, unpark and go back home or to work. That takes time from work, or children, or other matters. A course transmitted using modern media makes travel to some one place unnecessary.
Curriculum
Any course arises from some compendium of reliable knowledge. Physicians and nurses and dieticians possess such knowledge in their minds but students in a course have no access to it apart from the hours of teaching. Just as patients cannot learn to manage diet and fluids by reading they cannot learn just by listening; they and their teachers need to share a common base of knowledge – like the textbook for any conventional course in a school or on the web.
We Have Produced a Kidney Stone Prevention Course
We have done it. I and my writing colleague Jill Harris.
It Depends on this Site as its Knowledge Base
Jill wrote many of the most popular articles on the site about diet and fluids, and set out to find a way to use her materials as a course for patients. She and they can use other articles as well as source material. The site itself rests on a foundation of peer reviewed articles from PubMed to which its main articles link.
She Does One on One Patient Education and Finds it Limiting
For a long time, Jill has worked one on one with stone patients and encountered the problems of scale and cost. She long ago gave up on a fixed office format and coaches by phone or web media. But even so, scale and cost limit her reach. For 12 years she did brief education calls for thousands of patients nationally who used Litholink as their testing service. From her practice and her past Jill came to understand that scale and media and cost create many kinds of compromises in what patients can get.
She Uses Social Media to Form Active Support Groups
The web abounds in spontaneous social media groups of kidney stone patients. Patients value them and use them. Jill formed one for those interested in the course and curates it personally.
She Has Tried Her New Course Format Five Times Thus Far
Out of it all she chose her present format and has used it in five courses so far.
Her courses make room for up to 12 people. This size optimizes cost per patient, efficient use of one teacher, and opportunity for each patient to interact and ask questions. It may change with experience.
The main topics follow the medical logic of the site: fluids, sodium, calcium, oxalate, how to read lab reports, and questions and answers. It runs in six one hour sessions. I have personally participated thus far in two question and answer sessions – at the ends of the first two courses.
Where Does the Kidney Stone Prevention Course Fit In?
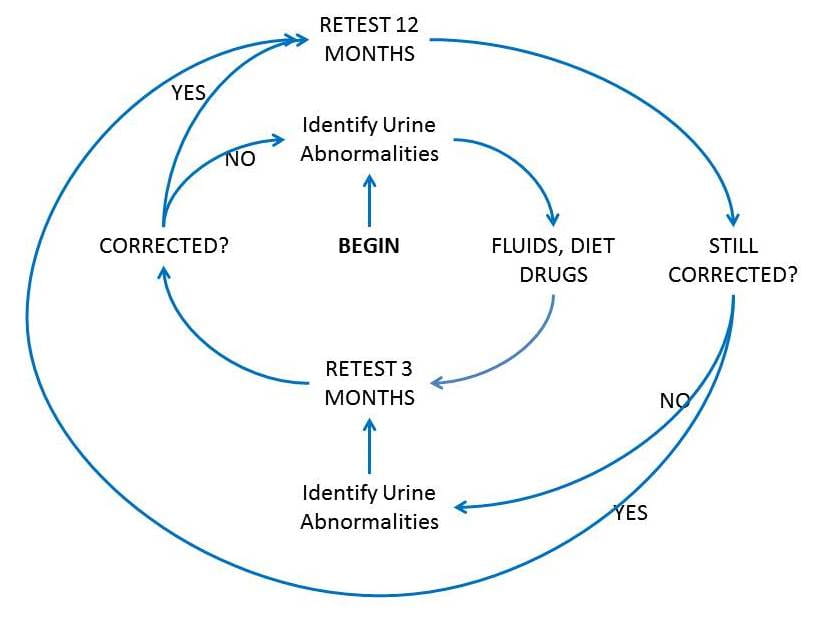
It fits within this figure that depicts my view of how testing and treatment work for stone prevention.
Things begin when physicians order initial tests (see ‘begin’ on figure) to identify the main abnormalities and make a treatment plan that includes diet and fluids.
Because the kidney stone prevention course aims at enabling the fluid and diet goals, it stands between when physicians identify those urine abnormalities and when patients adjust their fluid intake and diet within their lives so as to correct the abnormalities found.
It could also stand between any subsequent urine abnormalities due to unfavorable fluid or diet use and the retest to determine if the new treatment has the desired effects.
It acts much like Jill’s private coaching but with a group format that conveys greater scale, and lower cost per patient. Group interaction is a side benefit above private coaching. People get the audio file of every session.
They also get email support during the course. How much this adds and whether this can be maintained under increasing scale of courses remains uncertain.
What Has Happened So Far?
To date 57 people have enrolled in 5 courses of which 2 have completed. We have 22 email comments pending return of formal survey questions. Their uniformly positive tone encourages us that the courses are meeting real demands from patients.
Missing Parts
Responses to Poor Retest Outcomes
What happens when the 3 month retest results are poor for patient graduates of the course? Or 6 month, or one year retests?
Presently, nothing.
But in the future we will need another unit, probably individual free standing question and answer sessions for graduates who encounter less than ideal outcomes and need special issues resolved. They cannot redo the whole kidney stone prevention course but need the scale and cost benefits of group education.
Call this offering phase two. It serves not only problems from the 3 month retest but all subsequent problems graduates encounter within the purview of fluid and diet management.
Timely Review for Successful Graduates
Those of us with a long experience know that success breeds failure, that years stone free create a sense that all is well. But it may not be well and stones recur. Presently we consider some kind of one hour, perhaps yearly review for those doing well. Call it phase three.
Maintenance in Treatment
Ultimately physicians drive and maintain treatment. A course structure, a website – these are ancillary. But the outcomes of the courses concern us: Do people stay in their diet plans, their fluid plans; do their tests get done; are they good? We do not have a real plan right now. But need one soon.
Integration of the Kidney Stone Prevention Course and This Site
As a writer of her own articles Jill teaches from what she put up on this site. She also uses whatever I or others have written that concerns fluids and diet. Because the site rests upon the peer reviewed literature so does the course material and what patients learn.
One might think people would want to read an article, on sodium for example, before that part of the course. But no; they usually prefer to hear the discussion and then read, if at all. We have not collected formal data on this point but it suggests something about use of a knowledge source vs. direct education by a teacher.
Why Do I Say ‘We’ When Jill Does All the Work?
Because the site and the kidney stone prevention course work together.
I propose this specific combination of a web based course and knowledge base might constitute a new paradigm fostering large scale stone prevention. Modern media, web based, support public, affordable, scalable education about that part of patient care that patients must themselves accomplish. In stone disease and maybe beyond we desire to innovate and get better care for patients. Doing it, and ultimately presenting the results – this is coarse grained, public, clinical experiment. Not perhaps real research. We have no control groups, and aim only at the good of patients. But we will observe and see how well the graduates do.
Very excited about the webinar. Did not realize Jill was offering specific course work on kidney stone prevention. I agree that follow-up is critical. If I am to be successful with my program, I need to check in at least once a year. This way I know my numbers are good and I am staying on track.
I am looking forward to the Kidney Stone Prevention Course! I have registered but I didn’t see where I can request the oxalate list.
You did it already – automatic when you registered. Regards, Fred Coe
Hi! You get it st the end of the presentation- I will email them to everyone! Thank you for signing up! Jill
I am a 30yr retired military officer. I experienced my first stone while driving cross country for a change of duty station in 1988. More recently, in 2015, I passed another stone and during the imaging, they discovered an eight mm stone in my left kidney. In 2016, the eight mm stone had grown to ten mm and a four mm stone appeared. Eventually I passed and retrieved the stone and turned it in to my healthcare people. The ten mm stone had to be lasered.
The reason I am sharing all of this is because my healthcare provider is the VA. Needless to say, most of the stories you have heard on TV about the VA medicine – I have experienced. Specifically, the Urologist that lasered the stone recommended to me to have a 24 hr urine sample test. I collected the sample, turned it in to the VA hospital and have heard bupkis since. My Urologist (not the one who did the laser) continuously bemoans the fact that he has not retired and even asking his nursing staff about the results of the test have proved fruitless.
Meanwhile my anxiety over my propensity for stones grows and so far I have no intel from the VA. Thus I am trying to take care of my situation unaided by the VA. That is why I intend to enroll in this coursework identified in this post.
Thank you very much for your patience in reading my tales of woe.
Very respectfully,
Dave
Hi David, I know the VA has a lot of stories. The course will no doubt help you but you will need physicians, too. Good luck, Regards, Fred Coe
Hi Terri,
Exactly. No diet does fit all. That is why leaving your doc’s office with a generic “go on a low oxalate” diet won’t work. The kidney stone prevention course is a place where you can ask about your certain medical conditions and other restrictions.
The webinar will be recorded so no worries if you miss it live!
Jill
Hi David.
Thanks for writing. Look forward to having you in the kidney stone prevention course. It will help you tremendously. Please try and get a copy of your report before class starts. You don’t need it but it would be nice to have so I can take a look at it.
Talk soon-
Jill
I’ve tried to register for the course and it keeps giving me an error. It tells me that my email address is already in use. So I request password help and it tells me it doesn’t recognize my email. Is this a test? If so I’ve failed. Happy Valentines Day! Staying away from Chocolate! 💝😞
Hi Barb, I am sure you registered – But I will ask Jill to check out your comment. Regards, Fred Coe
Barb,
Sorry for you trouble. I had another tell me that as well. this belong to you- gbtorcaso , if so you are registered?
See you tomorrow!
Jill
I would love more information about this. I have been passing stones since I was 17. I am now 32, and have passed well over 200 stones! I pass at least one a month and am in constant pain. I have seen so many doctors, all without much hope, answers, or a real understanding of WHY I have so many.
Hi, The Webinar in Thursday is a good way to hear about it. Regards, Fred Coe
Rachel,
It’s sad that your physicians haven’t taken the effort to find out your specific cause of stones. My personal opinion is that they make too much money on your return visits. I’ve talked to many many people who have been told by their physicians that they are “just one of those types of people who are going to form kidney stones”. These prognosis are a sad testimony to the medical field, especially when there has been PLENTY of research and deeper understanding on causes and effective treatments for kidney stones. It may be time to find a urologist who will analyze what is actually going on in your body. Be sure to read Dr.Coe’s other writings about kidney stones and studies done on treatments for kidney stone prevention. Too many “remedies” only target kidney stones when they form. It’s more important to understand 1. why your body is forming them 2. what type of stone(s) you form 3. finding a solution for PREVENTION. I wish you well and best of luck in your endeavor to find relief. You’ve landed on a very informative and helpful site.
I do not believe the problem many patients with kidney stones have with urologists is mainly because they want patients to keep coming back and having surgery; because they want the money. The problem is few urologists in private practices are interested in stone disease. Urologists are trained to be surgeons in 5 and 6 year residencies. Many are therefore, interested in performing surgeries. They should refer patients to nephrologists who will help them, or other urologists if they know of any or at the very least, tell patients they need to go to a medical school. Preferably with a urology and/or nephrology residency program. Many states have state universities only, but some states have private schools too. Also places like the Mayo and Cleveland Clinics offer very good treatment and have locations in several states. Of course the program at University of Chicago for stone treatment is excellent too.
And no matter what kind of insurance a patient has: if they are a resident of a given state, the state university medical school must offer treatment for state residents. And there are financial programs to help with the cost of treatment. However these are set up around state and federal laws. Private universities have their own criteria for financial help.
A urologist with a subspecialty in stone disease explained this to me. Also many people don’t understand how urologists and nephrologists can work together and that there are advantages to seeing both specialists.
I am very fortunate that I had excellent medical care for 42 years. And long ago when I was hospitalized and I was about to be released after having pyenephritis and septicemia and recovering, my nephrologist saved me me from ending up back at the ER room. He insisted I have another IVP, which was largely used before CT scans which resulted in emergency surgery. My urologist and nephrologist argued about that while I sat in my hospital bed. Another cluster of kidney stones was getting ready to make a new obstruction very soon.
And it was not either of my doctors or the hospitals fault that I had been so sick and needed emergency surgery.
First, I’d love to watch the class but I can’t attend during work hours. Will it be recorded so we can watch it later?
Second you have to keep in mind everyone is different. There is not a one size fits all diet because most of us have some sort of restrictions. For example, I need to avoid lactose and foods that aggravate reflux including lemons so I can’t have lemon water. I also have limitations having had my gallbladder removed. And that’s cooking for me alone and not counting cooking for the rest of the limitations of my family.
Hi Terri,
Exactly. No diet does fit all. That is why leaving your doc’s office with a generic “go on a low oxalate” diet won’t work. The kidney stone prevention course is a place where you can ask about your certain medical conditions and other restrictions.
The webinar will be recorded so no worries if you miss it live!
Jill
I watched the webinar with great enthusiasm, Dr. Coe. It’s no surprise what she talked about is exactly what you and I discussed a year ago, when you did a thorough blood/urine analysis and put me on the right track regarding diet, fluid intake and medication. So far, so good. No stones to date!
Hi Dave, I am glad that things seem consistant, and I hope you do well. Best, Fred
I have completed the kidney stone prevention course and it was very informative and helpful. I also had an appointment with Dr Coe last October and I can’t tell you how much I appreciated his kindness and caring and explanation delving into my kidney stones. I have changed my diet significantly and realized that I wasn’t having the calcium I needed to prevent new stones. I have a question regarding magnesium- should I be concerned about how much magnesium I need because I have increased my calcium intake ?? I repeated my 24 hour urine yesterday. Fingers crossed for improved results !
Hi Sheila, thanks for the kind words. As you are my own patient, we will meet when you have your new results and I can help decide about the extra magnesium. Regards, Fred
Respected Sir,
I would like to know if hyperthyroidism(thyroid gland not parathyroid gland) cause kidney stone
Hi Krishna, hyperthyroidism does indeed cause kidney stones via increased urine calcium. It needs to be treated on its own and as a cause of stones. Regards, Fred Coe
Dear Sir,
How would I differentiate between whether the hyperparathyroidism or hyperthyroidism caused the kidney stone
Hi Krishna, The hyperthyroidism is treated first, and treatment is monitored by your physician. When it has been controlled, he/she can determine if your serum calcium is high and if so if serum PTH in that same serum is high or normal – not low, and that your 24 hour urine calcium is high. This fulfils the criteria for hyperparathyroidism. This matter is very complex and managed exclusively by your physician. Regards, Fred Coe
I had an intestinal bypass in 1973 for obesity. I lost 125 lbs and with monitoring my food
intake, I manage to keep the weight off. A year ago I was diagnosed with kidney stones
in both kidneys…small ones on the left and one large one on the right. I have not experienced pain and I am monitored by a urologist twice annually. Is this related to the
surgery I had 44 years ago?
Hi Marlene, Off hand I would guess they are, in that bypass surgery often raises urine oxalate considerably. I would be sure to have proper 24 hour urine studies to measure all stone risk factors with especial interest on urine oxalate excretion. Sometimes the urine oxalate is very high, and that is important to deal with. Regards, Fred Coe
Is the Kidney Stone Prevention course still being offered? If so how can I get more information?
Hi Denise.
Yes it is and it’s been very successful. You can go to jillharriscoaching.com/course to sign up. A new one will be starting in the next couple of weeks. They fill up quickly so sign up soon!
Warmly,
Jill
Jill thank you for your quick reply. Can you tell me what time and what day of the week you will be having the calls? I live in California and work full time so I want to make sure that it is on a day and time that I can call in. Also if we have to miss a call will there be a recording available? I’m looking forward to joining the class.
Dr Coe
I was in an auto accident 3 years ago. I had blunt trauma (bruising and contusions) to the right kidney with no penetration. Several weeks after accident upon routine blood and urine I was found to have blood in urine and elevated uric acid, kidney function tests. Referred to urologist for ct scan, 24 hour urine. Regular xray did not show stones, so they were assumed to be uric acid stones. No stones collsction or analysis done. Ct scan showed several kidney stones in right kidney. Put on potassium citrate er 15meq 1 tab 2x daily, theralith xr 2 tablets twice a day, increase fluids. I started to experience kidney stone attacks within 2 weeks and have had 5 attacks so far.
Recent ct scan still shows stones present in rt kidney. Prior to auto accident no hx of kidney stones. Had ct scan several yrs prior to accident prior to colonoscopy that showed no stones.
Do you know of any association of blunt trauma to kidney from an auto accident that caused damage and subsequent formation of kidney stones. My current age is 72. Thank you
Hi Beverly, The best guess is some kidney injury from the accident, loss of some kidney function, lower urine pH, and uric acid stones. They should stop with potassium citrate but all is in measurement. What were the 24 hour urine pH values before treatment? How about during that treatment. What else is wrong in the urine chemistries? On CT your physicians can ascertain uric acid by the magnitude of radiographic density – anyone can do it. Uric acid has a low density. Be sure you have been fully evaluated. Regards, Fred Coe
You prescribed daily 1200mg calcium intake for me in my October visit with you. Having trouble getting to 1200mg daily due to IBS. Have been eating daily greek yogurt, coconut milk, low sodium cottage cheese, string cheese. Can you recommend Calcium supplement to help make up the difference. I understand there are more than one type of calcium supplements. I am also on low sugar, low oxalate diet. Have lost 25 lbs.
thanks. Could you reply to my email account. I have trouble finding your replies again.
Beverly Dow
Hi Beverly, I will reply to you personally. Regards, Fred Coe
I just finished my sixth lithotripsy over the course of about 12 years. My first stones were tested and were calcium oxalate. I am a recently retired RN and need to get serious about prevention. I hope to sign up for the class.
Hi SUsan, Too many ESWL procedures and prevention is indeed right for you. The course is terrific. Here is a plan to read about. Bests, Fred Coe
I am a 62-year-old male whose first kidney stone was discovered in October, 2016. That is when my kidney cancer was found also. Though it was classified as Stage 1B, I am now considered Stage 3 CKD. Now I have to watch my sodium, potassium, phosphorus, and protein intake as well as my oxalate levels. I am looking for a diet program that takes all of this into consideration.
Hi Kevin, given CKD 3 you do not have to limit your diet potassium or phosphorus but simply avoid excesses. Protein intake can be in the normal limit of 0.8 to 1 gm.kg/day. For your kidneys stones, prevention should follow a complete evaluation for causes, so be sure that has been done. The courses are available as per the link from this article. Let me know if you have trouble contacting Jill Harris who runs them. Regards, Fred Coe
After my surgery, my Creatinine was 1.35. I had the 24-hour urine test done in June. My 24-hour Creatinine was 3.32, eGFR was 56, potassium was 4.1, sodium 142, calcium 192 oxalate acid was 56. Nephrologist told me to eat more fruits and vegetables and less meat. Will the course still help?
Hi Kevin, Your serum creatinine is a bit high but your 24 hour urine creatinine is mammouth. If the collection was accurate for 24 hours you have a very large muscle mass. The creatinine clearance (liter/day) is urine creatinine (mg/d)/serum creatinine (mg/l) which is in your case 3320 mg/d/13.5 mg/l or 245 l/d, or in ml/min which is what is usually calculated 171 ml/min. The eGFR equation assumes a urine creatinine but for people with so much muscle mass as you appear to have (normal urine creatinine is 1600 to maybe 2000 mg/day) your serum values gives a reduced clearance. The other possibility is that you are giving me a 48 hour urine creatinine or somehow over collected. Likewise your urine oxalate is very high, and perhaps that is also a collection artefact, or perhaps real. In any event your nephrologist might want to look at the urine creatinine and consider if the collection is correct. Regards, Fred Coe
Hi Dr Coe
you prescribed 1200mg daily calcium for me at our October visit. I am having trouble getting to 1200mg due to IBS and inability to tolerate whole milk products without pain. I have been eating daily greek yogurt, coconut milk, low sodium cottage cheese, string cheese. Can you recommend a calcium supplement. I noticed there are several types. Which is best for me. I have lost 25 lbs. I am on low sugar, low oxalate diet and exercising.
Thank you
Hi Dr Coe, I follow and talk to Jill on Facebook. I asked her and she felt you may be able to answer this question. How does Testosterone Replacement Thearapy (injections) affect the kidneys or stone production. Would steroids have the same effect?
I produce calcium oxalate stones but I’ve been following my diet closely to prevent forming new stones.
Hi Jason, Testosterone could alter urine pH or possibly calcium, although papers are pretty hard to find on this subject. In a highly contrived mouse model the androgen receptor seems to alter oxalate production by liver challenged with oxalate precursors. On the other hand, in menopausal women who formed stones or not, it was estrogen, not testosterone levels that correlated with stones. Among men with stones compared to normal men, serum testosterone was higher – a point in favor of the hormone as a cause. But that paper is very weak. So, poor science, little known. If you do not need the hormone stop it, otherwise, continue. Regards, Fred Coe
Hi Dr Coe, would this course be useful for me, in that, I have a 9 year old Bichon Frise/Shih Tzu with CA Oxolate Stones, I have an analysis from Guelph University. I’m reading the comments here, and wondering if diet and or tests, could assist me in developing a die for Rio, that will reduce the chance of CA Oxolate stones to return. I’ve read that kidney function and how it uses Calcium or doesn’t process it properly can dump excess Calcium into the bladder, which then binds with the Oxolate. I am devising low Oxolate food for him, but I need to know how to ‘stop’ the Calcium from binding with the Oxolate. Thank you.
Hi Susan, Stone disease in non human animals is a specialty in veterinary medicine, and far outside of our skills. Regards, Fred Coe
My vet recommended a special food for my bichon. She has not had a stone since and it has been years. I can’t remember the name of it and I keep food in a bin so I don’t have the bag, but ask your vet and if he does not know, google it. Good luck.
Hi PC, I am happy for your experience but need to make clear that veterinary medicine is as far from me as Venus or Mars. Everything is different for animal stones vs. human, and I have no knowledge at all about the former. Moreover this site is not relevant to animal stones. I say this to be sure no one is mislead and therefore no animal is harmed. Regards, Fred Coe
Hello, i would be interested in this Course, i Live in The UK, I have had Oxolate Kidney stones on and off foe 29 years, i have had several operations and am awaiting a 4th Ureteroscopy now, i have had 10 operations since 1988.
I am am my whits end with the Urologists, i am waking up early hours in the morning in agony, i am prone to Pyelonephritis (Infections) and hydronephronsis. i am due to see my Surgeon tomorrow for a Consultation, and don’t want to be fobbed off, i need answers! I have changed my diet, so i understand what i cannot and can eat, i would appreciate some feedback on what to say to him regarding all this, after 29 years, i still have no answers from them.
Many thanks
Miss Shirley Clarkson.
Hi Shirley, the course is about diet and may benefit prevention. But the whole of prevention is more than diet. Here is a reasonable review. I gather you have stones sans systemic disease; this is my best review of treatment for the common ‘idiopathic’ calcium stone formers. This article may help – it presumes interested physicians, however. Likewise this one about how to pull things together. With all the stones, I imagine you need both diet/fluids and medication. Regards, Fred Coe
Dr Coe, just thankfully found your site. Not tech-savvy, didn’t know how to submit comment without hitting “reply” to another’s, please overlook “intrusion!” Hoping you can advise! I am 68, retired RN, in Chicago burbs, had one oxalate stone removed in Oct 2015. Was given almost nothing in the way of stone prevention info, no initial baseline 24 hr urine had been advised or done right after stone removal. Was overweight/obese, poor lifestyle, basically made no changes. First 24 hr urine was Mar 2016, results of course were not good Was then prescribed K citrate 15mEq/day, and had my HCTZ (which I was already on for HTN) increased to 50 mg. Since May 2017, have lost over 25% of my body weight, so far, changed my diet and exercise, drinking a lot of H20, starting to watch Na+ intake, likely not enough Ca++, a work in progress. Many other lab test results have greatly improved. I am now tending to mild hypokalemia, no doubt diuretic-induced, and would like to get off the higher HCTZ, rather than add yet another med, KCl, to my list to compensate. Second 24 hr urine in Nov 2017, urine volume 3.75 L, pushing fluids for impending URI and for weight loss. I was told to cut back a bit on H2O and repeat test in one year. Is it possible to ever get off these meds, once they have been started? Can you take the K citrate without the added HCTZ? If so, are you still seeing patients? Please advise, and thank you!
Hi Joyce, I do understand the questions as a bit specific and also important. Yes, I do certainly see patients and in your case if you wish just call my secretary and come in with your data so I can be more helpful – Kathleen Dineen, 773 702 1475. Regards, Fred Coe
Hello,
I develop calcium oxalate stones on a regular basis. When I finally saw a doctor(when medicare kicked in so I could afford one)he and my urologist convinced me to have my thyroid removed and they both agreed I would not have another stone. I believed them and within 3 months of having it removed, I had my second stone surgery. Both doctors(term used loosely here) were red faced at my next appointment and the urologist suggested I see a kidney doctor who is having some success with prescribing a certain blood pressure medicine that has been known to interrupt the calcium stones from forming. I asked what were the worst side affects and death came up as one and I would have to be monitored each week(a real money maker). I declined as my blood pressure is usually 106/71. I find it hard to believe there isn’t a remedy for kidney stones as they go back thousands of years…perhaps not enough money to make off a cure? I now take an herbal remedy called Chanca Piedra, taken in capsule form each day. When I forget and notice that tell-tale dull, low back pain kicking in, I take 2 caps 3X a day for a couple of days and within a few hours the pain is gone and my urine stream is heavy and complete. I have not had an attack for 4 years now and I was having them every few months with incredible pain and lots of blood in the toilet. The herb is an old remedy from the Rainforest that has been used for hundreds of years. I also developed type 2 diabetes and the diabetes diet cancelled out the stone diet which was very defeating and with doctors who not only don’t have a clue, but lack even a caring attitude and this is their specialty! What this has done for me, however, is sharpened my own awareness of having to research each and everything I am told and not to take anyone’s opinion of how to treat you as gospel. It is exhausting to always second guess what is being told to you, but read, read and then, read again everything you can on the subject. You need to be your own advocate.
Hi Sharon, I know about the herb and have meant to write about it but have not had time. It has little evidence to support its use but it seems to have been a benefit for you and that is wonderful. The thiazide your physician recommended almost never has caused death and is in fact the main drug for high blood pressure – you do not have that! – and in that use has saved lives. The kidney stone diet is actually ideal for diabetics, being identical to the diet recommended to all Americans; take a look. One of the main reasons it is recommended in the US is against diabetes. What I do not much like about your prevention is that without that kind of diet you have no protection against bone disease – take a look. Regards, Fred Coe
I’m in Australia.
I’ve suffered extreme pain left side, left flank for 10 years.
I had a specialist do work on my vagina though I had two easy births and felt I’d never experienced a prolapse.
Another specialist booked me in to remove 1ft of my colon. I was sceptical. I lived with the pain for years until February 2018 when I ended up again in the Goulburn Base Hospital, Goulburn and saw a gastroenterologist who put me on a drip and ordered a CT scan. He discharged me the next morning in the same pain.
The CT scan again (I had many) showed a 2 cm stone in my left kidney. This was ignored.
I then sought further opinions from St Vincent’s Clinic, Sydney. I saw a gastroenterologist, Dr Alan Meagher, who said my symptoms did not match diverticulitis. I then saw Dr Kooner, Urologist.
I have been in treatment every 2 weeks since early March. Ureter stents, lasering, lithotripsy. It was no easy process. I’m now stone free. Go back to Dr Kooner in 8 weeks for another CT scan and seeing, Dr Mark Penny, Nephrologist, about proteinuria.
Dr Kooner saved my kidney which was being compromised by the large stone.
I’m drinking lemon juice water each day. My huge stone was calcium oxylate.
I’m wondering if this diet will suit me?
To stick on a program I need a weekly menu system. Does this diet contain a menu system?
Hi Rosemary, Prevention of more stones is a process, and the course is really only about diet counseling in the event that is all you need. Right now you need a full evaluation to find out why you formed stones in the first place. That begins with analysis of the stone and blood and 24 hour urine testing. Your physicians are in charge of all that. Here is my favorite overall article as a starting place. Regards, Fred Coe
Hi, I’m in New York.
My husband has kidney stones almost every year for about 30years.
Last May 17,2018 he has left plank pain that relieves by Naproxen but the following day,he has a bloody urine, nausea and vomiting. So I brought him to Emergency of Mount Sinai Hospital about 6pm because of pain,bloody urine and vomiting. CT Scan done. found out a 4mm kidney stone.By 10:30pm he was discharged bec.he was relieve with pain medication. Sunday night May 20,2018 he felt really bad pain which I took him back to the Emergency.And his primary doctor told my husband stay in the hospital until the kidney stone pass out.
So my husband stayed in the hospital until his urologist scheduled a Cystoscopy for both Urethral Stent insertion May 25,2018 @9:00am. The surgery takes about an hour and after the surgery he pass out about 6pcs of stones.I saw it bec.I stayed with him in the recovery room until they transport him to his room about 12:30pm.
At 6:30pm of the same day he was discharge with a urethral stents.
At home he was complaining burning sensation upon urination and bloody urine which is normal after surgery.May 27-29 he feels great!No pain,no bloody urine. So we went to his urologist appointment 2pm of May29,2018. The urologist remove the Stent on his office.We went to the restaurant for dinner and he pass out 1 stone.When we got home he has pain, bloody urine and pass out another 4 stones.Only a prescription pain medication relieve that pain.Until now he feels the same and I’m worried for taking this pain medication because he is Hypertensive and Type 2 Diabetes Mellitus.
What should we do Dr.Coe.I need your help.
Thank you
Hi Junifer, judging from the story he has many retained stones or stone fragments. His urologist can attend to them if needed, or they can pass. Being diabetic it is important to avoid obstruction as his physician knows. So, the immediate episode is workable and will resolve. Of greater importance, what are his stones made of? In diabetics uric acid is common and prevention is nearly perfect. If another kind of stone, prevention will still be effective. So when this is over he needs a proper program to prevent more. Here is a good place to start reading about what to do. Regards, Fred Coe
Hello Dr. Coe,
I recently passed my 2nd stone, (“several” 1-2 mm left in right kidney), composition:
6MM, 98% Calcium Oxalate Monohydrate, 2% Protein
My first was,
4MM, 96% Calcium Ox, 2% Protein, 1% ea Calcium Phospate Carbonate/Hydroxyl
My 24 hr urine comparison revealed,
Urine volume up from 1.71 to 2.54
CaOx down from 7.42 to 4.99
Urine Sodium down 171 to 105
Calcium/Creatine 211 to 207
Not good:
PH up from 6.0 to 6.1
Urine Calcium up 244 to 284
Protein .9 to 1.4
Phosphorus .826 to 1.085
Sulfate 30 to 55
Nitrogen 7.32 to 12.69
Calcium/kg 3.7 to 4.3
During this 24 hr analysis, I tried to keep it somewhat real and did not realize the sodium in “reduced sodium” soy sauce (2400 per 1/4 c.) so that was out of ordinary, will not use again!
I didn’t record foods in 1st 24 hr to compare.
Sodium 3,000 overall – holy cow if I ingested 1/4 c. so may be overstating
Protein about 69 (high also)
Calcium only 69% of 1200 goal
Thiazide recommended but doing another analysis in 3 months first. I really don’t want to take medication. Could this be off due to my diet sodium, protein, calcium above? Surprisingly my sodium was within range(?)
Suggestions? Thank you so much in advance!
Hi Lisa, One more! This one adds that you know your sodium was too high and calcium low, protein high. So, fix this and retest. Regards, Fred Coe
Any data on oxalate content and coconut milk
Hi M Butensky,
We have no hard data, but I do have my patients eat and drink coconut products and their urinary oxalate remains lower than before they started the diet (and adding coconut products).
Best,
Jill
Any information regarding nutritional drinks for cancer patients?
My mother underwent treatment and diet is almost exclusively Boost Very High Calorie (problems with swallowing and dry mouth).
She developed calcium oxalate kidney stones this year.
Hi Laura, If she is getting very high protein intake that could raise urine calcium and cause stones. It has soy protein and could be high in oxalate. The best approach is to do a 24 hour urine and see what is causing the stones. Regards, Fred Coe
What is the recommended protein intake for a 77 year old? Her current intake (from Boost VHC) is 66 Grams/day.
Hi Laura, I do not know her weight but 1 gm/kg of body weight is ideal usually. For special supplementation after illness one might want more for some limited time. Regards, fred Coe
Dr. Coe,
I am 63 and stand 75 inches and weigh about 190 lbs. I follow Jill’s course and my numbers are all good according to Jill. I had a total right nephrectomy in 2016 when I had my first and only stone and thyroidectomy in 2018. Both due to cancer. My eGFR is 54 and my creatinine is at 1.4. My nephrologist has limited my protein intake at the same levels as Jill and you recommend but I am noticeably losing muscle mass. I try to eat about 2500 calories per day. Any thoughts or advice?
Hi Kevin, Losing muscle mass is a medical problem, and a bit beyond the range of this site. Given the thyroid disease, perhaps your replacement dose of thyroid hormone is too high. Eating 0.8-1 gm/d of protein – the right range – should not cause muscle loss. Be sure you are not too low in protein – 24 hour urine PCR will show you that. Otherwise, if none of this works, your physicians will have to figure it out. Regards, Fred Coe
Good evening Dr. Coe. I am 40 years old and was diagnosed at 18 months old with primary hyperoxaluria. I understand that following the Kidney Stone Diet will not completely keep me stone free, but in your opinion will it help curtail the frequency of new stones? I take potassium citrate, but no other medicines or vitamins.
Hi Matthew, That is a very complex and potentially dangerous disease, and I hope you are receiving care via a major center with skills in its management. Diet is of marginal help except that high sodium intake and avoidance of diuretics are important to reduce risk of kidney damage.The linked case is hyperoxaluria from intestinal bypass, but oxalate is oxalate, and the physiology applies broadly. The low sodium aspects of the kidney stone diet are not correct for you, nor is the high diet calcium unless carefully monitored. I am sure you know that Mayo Clinic has a special program for PH1. Regards, Fred Coe
Howdy 🙂
I understand that eating dietary calcium with oxalates can bind the oxalates in the stomach and intestines, so that it can not combine in the kidneys and possibly form crystals. How many grams of dietary calcium from dairy sources should I eat to bind a gram of dietary oxalate? I’m thinking chocolate milk, putting cheese on my brussel sprouts (super good, btw :-), and such as that.
Second, I am reading conflicting studies about lemon juice vs orange juice consumption and effect on urine pH and forming oxalate stones. Which do you prefer?
Last, in all of the estimate tables that I have found, 8oz of “orange juice” is shown as about 1/10 the oxalates of an orange. The only thing I can conclude is that the oxalates are in the pulp of the orange, which is pargely eliminated in “no pulp” style OJ. Does that seem sound to yall?
Thank you very much!!!!!
Hi Dale, The equivalents for diet calcium vs oxalate are not known at the level you want. Therefore the best idea is to eat some high calcium foods – almost always dairy – with meals that have significant amounts of oxalate. As for the fruits, they often contain citrate as citric acid when tart (low pH) and citric acid does not produce alkali when metabolized and therefore cannot raise urine citrate. As for oranges, the rind is most likely to concentrate oxalate. Regards, Fred Coe
Hello, what a wonderful website! My question concerns a stone analysis with 10% Ca Oxalate Monohydratre and 20% Ca Oxalate Dihydrate. Brushite Crystal is 70%. It would seem that there is a small amt of Oxalate compared to Brushite. ls a diet low in Oxalate not needed here, but one low in brushite??? As always, fluids taken seem to be a priority in most literature. Thank you.
Hi Deborah, brushite stones are a special case and require special handling. They are a version of calcium phosphate stones. You need to start with a comprehensive evaluation, and will no doubt find high urine calcium and pH as main causes. Brushite is central in calcium stone production, and brushite stones can grow rapidly. Of importance treatment needs to be sufficient to lower urine brushite (calcium phosphate) supersaturation below 1, something your physicians certainly accomplish if they agree with what I have written. Regards, Fred Coe