Kidney stone types

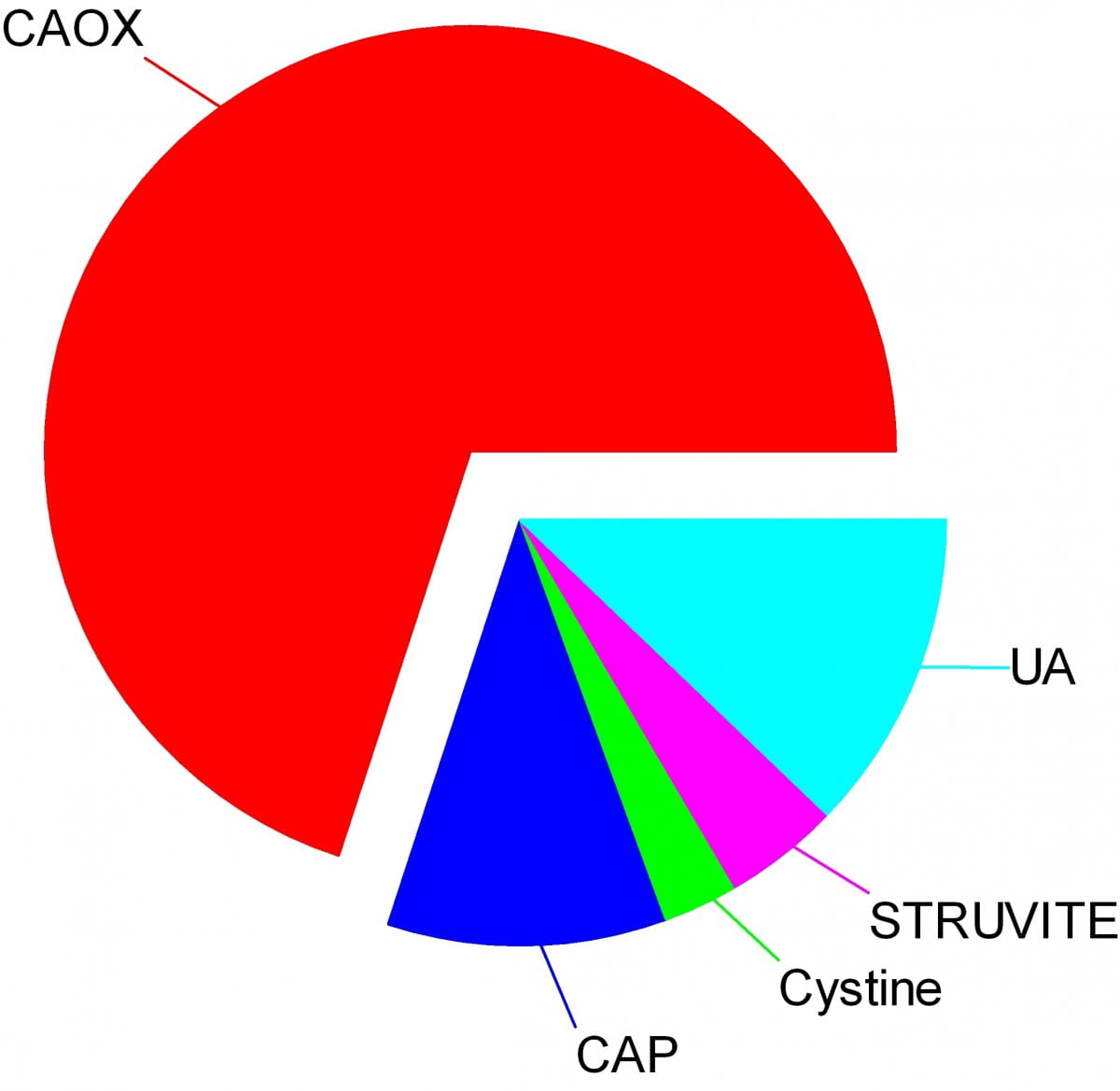
Crystals make stones and their names signify the kidney stone types. Here are the names of the crystals that make the stones: CAOX, Calcium Oxalate; CAP, Calcium phosphate; UA, Uric Acid; Cystine; Struvite.
The wedges on my pie chart show the relative abundances of stone types in our large population of stone forming patients. Calcium oxalate stones predominate by a wide margin in our clinic and in all others I know of.
The names, matter because the whole science of stone prevention focuses upon stone crystals. Each kidney stone crystal creates its own unique illness and requires specific treatment. That is why we name stones by the names of their crystals and why when stones are analysed the results are reported by these very same names.
Being a bold and rather large graphic, the featured picture does what I intended, brings the main facts into view as, at a circus, the great animals and the small animals circle the ring by way of an introduction. Come. I will show you all the common stones, like at a fashion show, or a circus parade. You can watch as they go by and remind yourself, or wonder, which ones might have been yours.
Here they are.
Which type do you have?
You might think your doctors know what stones you have formed, but don’t rely on it. People move, doctors move, health records are far from ‘all electronic’. That stone report from 4 years ago could lie in a dusty filing cabinet, your new doctors unaware it exists. Worse, it could hide in a dresser drawer and you forgot it you put it there. Perhaps even more worse, the stones might stay in that drawer, never analysed at all. Find the stones, find missing reports, urge analysis by your physicians. They can help you most if they know your stone analysis.
When they do not know, physicians can still mount prevention efforts but with less focus and probably less effect than when guided by a knowledge of the crystals. So always seek treatment. If a stone comes along the way, make every effort to get it analysed.
Why should you care to know all this?
Because you will conduct much of your own treatment, and over many years.
Since stones tend to recur, prevention requires treatment over long periods. These treatments work by altering urine chemistry in a direction that minimizes the risk of forming crystals. Such altering of urine chemistry requires control of fluid intake, lifestyle, and diet, and sometimes additional use of medications.
Just as the sailor who aims along a chosen track against the random, misdirecting, confusing sea and air maintains a constant way in proportion to that skill which comes from knowing the way of the boat, patients who aim to keep a certain kind of condition in their urine despite the demands and temptations of the world do so, I believe, in proportion to skills that come from knowing how their work and lives and foods affect their bodies, and how those crystals form which they so much desire to prevent.
Put another way, knowledge is power.
Why is this article so long?
I wanted to put all five main types of kidney stones. That makes a long story. But probably you will care to read about only your own type.
I should mention here, to save a lot of confusion, that stones often contain mixtures of crystals.
The pie chart refers to the most common crystals in a stone, for which the stone is usually named. Much of the time, minor crystal components are not crucial, but sometimes – to jump forward a bit – they are. Even a trace of struvite or cystine, for example, can have great diagnostic importance.
Calcium stones
Calcium Oxalate Crystals
In the great circle atop this page article, the calcium oxalate stone, being most common, occupies a lion’s share of the space. 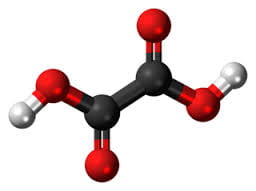
The calcium oxalate crystal forms when calcium combines with oxalic acid. Oxalic acid (at left), a dead end waste product that the kidneys remove, contains two carbon atoms (the large black spheres), four oxygen atoms, and two hydrogen atoms (silver).
At the acidity of urine, the positively charged hydrogens leave their negatively charged oxygens. As a result the oxalate molecule carries two negative charges. In the figure at right one negatively charged oxygen attracts the hydrogen of a nearby water molecule (H – O -H) while another attracts a positively charged calcium atom.
You can imagine how another oxalate ion (the name for a charged molecule in water) could attract the same calcium, or another calcium atom attract the bottom oxygen on the oxalate molecule so the chain extends and makes a crystal. You can see more about this in a video I made. Broadly speaking – though my more expert colleagues may bridle at such a simplification – the calcium atoms and oxalate molecules combine by the attraction of their opposite charges.
The calcium oxalate kidney stone comes in two varieties, calcium oxalate monohydrate and calcium oxalate dihydrate. The former are harder and therefore more resistant to fragmentation by lithotripsy. Likewise, the former appear more often when elevated levels of urine oxalate are present.
Calcium oxalate stone formers
From Systemic Diseases
Sometimes this kidney stone arises from a systemic cause, like bowel disease, primary hyperparathyroidism, or primary hyperoxaluria. Only physicians can establish that a known disease – like bowel disease – is the cause of stones. Only physicians can discover underlying primary hyperparathyroidism as a cause of stones. Patients cannot do much for themselves except provide as complete a medical record as possible.
Idiopathic
Most of the time this kidney stone arises simply from the interplay between inheritance, diet, and aspects of daily living. We call such patients idiopathic calcium oxalate stone formers, from Greek ἴδιος idios “one’s own” and πάθος pathos “suffering”.
Even though physicians discover the links between daily living and stone production, and select those changes that can prevent new stones, patients themselves must create and maintain those changes. I believe patients can so this in proportion to how well they understand what is needed, and why. When changes in daily life are not enough, physicians add medications, so even then patients remain active therapists for their own disease.
Stones usually form on kidney surfaces
About one million nephron units make up a normal adult kidney. The calcium oxalate kidney stone type does not grow in the tubules of the nephrons but ‘outside’ them, on the surfaces of the renal pelvis where final urine collects and drains through the ureter to the bladder. Here is a video that shows how they can form.
Calcium phosphate crystals
Phosphate ion and urine pH
Calcium phosphate stone crystals form when calcium atoms combine with phosphoric instead of oxalic acid and produce the calcium phosphate kidney stone.
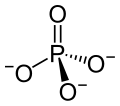 Phosphoric acid is simply a phosphorus atom (shown as the ‘P’ in the line drawing to the left) with 4 oxygen atoms bonded to it. One oxygen atom has two lines for its bond to phosphorus; this oxygen cannot provide any charge with which to bond calcium atoms to make a crystal. The other three have ordinary bonds that are shown by a line, and a dashed and solid arrow. These two arrows mean simply that the oxygens lie above and below the plane of the paper – so if you built the molecule with sticks and balls it would have a three dimensional shape.
Phosphoric acid is simply a phosphorus atom (shown as the ‘P’ in the line drawing to the left) with 4 oxygen atoms bonded to it. One oxygen atom has two lines for its bond to phosphorus; this oxygen cannot provide any charge with which to bond calcium atoms to make a crystal. The other three have ordinary bonds that are shown by a line, and a dashed and solid arrow. These two arrows mean simply that the oxygens lie above and below the plane of the paper – so if you built the molecule with sticks and balls it would have a three dimensional shape.
One of the three negatively charged oxygens never has a hydrogen on it in urine but only in exceedingly acidic solutions. A second charged oxygen is always occupied by a hydrogen atom in urine.
This makes the third oxygen, variably occupied by a hydrogen in urine, a tie breaker.
In a urine of average normal acidity (pH around 6), most of the tie breaker oxygens have their hydrogen leaving the phosphate ion only one negative charge. Not enough to make a crystal.
When the urine is abnormally alkaline (pH above 6.3 or 6.5), the variable oxygen becomes charged so the ion has two negative charges that can combine with calcium to make crystals. For this reason the calcium phosphate kidney stone tends to occur in people who produce a more alkaline urine than those who produce calcium oxalate kidney stones.
Brushite vs. hydroxyapatite
Much like calcium oxalate, calcium phosphate crystals begin simply as one to one pairings of doubly negative phosphate ions with doubly positive calcium atoms. This initial crystal is named brushite. Brushite, which is an equal mixture of calcium and phosphate ions, can convert to hydroxyapatite (HA), which has a more unbalanced proportion of calcium to phosphate. Hydroxyapatite crystals make bones hard.
Because less soluble than brushite, hydroxyapatite cannibalizes brushite. The organic molecules in urine modify this process.
Calcium Phosphate stone formers
From Systemic diseases
Primary hyperparathyroidism and renal tubular acidosis raise average urine alkalinity (higher urine pH) and foster calcium phosphate kidney stones. Many uncommon genetic diseases do the same.
Idiopathic
Idiopathic calcium phosphate stone formers share a common set of traits. Perhaps because urine contains far more phosphate than oxalate, they form more frequent and larger stones than idiopathic calcium oxalate stone formers. Often the stones originate as crystal plugs at the terminal ends of the kidney tubules. More crystals deposit over the end of the plug open to the urine, to make the final stone. Crystal plugs damage the cells that line the tubules and cause local scarring.
Uric acid stones
Uric acid crystals
Structure and charged sites
A breakdown product of DNA and RNA, uric acid forms crystals in abnormally acidic (low pH) urine. Obese and diabetic people, those with gout or kidney disease typically produce abnormally acid urine. I know how the urine becomes acid, but leave it for elsewhere on the site.
Uric acid, the molecule we are interested in here (shown to the far right), has two linked rings made of carbon atoms (they are at the angles where lines join), with  interposed nitrogen (N), oxygen (O), and hydrogen (H) atoms.
interposed nitrogen (N), oxygen (O), and hydrogen (H) atoms.
This molecule has only two charged sites, the nitrogen atoms at the bottoms of the rings. In urine of pH 6 or so, one nitrogen lacks its hydrogen and therefore carries a single negative charge. In more alkaline solutions both nitrogens lack hydrogens, but urine does not normally achieve such alkalinity (pH>8).
When urine pH is low (<5.5) and both nitrogens have their hydrogens, the molecule lacks any charged site, so water can no longer find a hold on the molecule. It crystallizes. It simply leaves the water as water droplets themselves form from the high and vaporous late afternoon clouds and fall from the air as the warm rains of springtime.
Relation to water
Water molecules are each a single oxygen atom (large ball) bonded with two hydrogen atoms (small balls) as in this picture from Wikipedia. The hydrogen side has a positive, the bare side of the oxygen a negative charge. So water molecules link to each other, 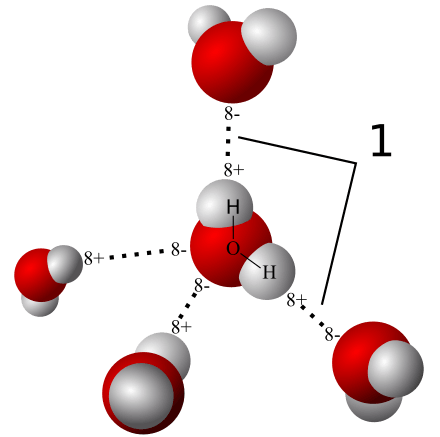 positives to negative surfaces, to make up the clear and seemingly continuous fluid we drink, swim in, and hold up umbrellas to keep off of us when it rains. They link by charge at angles, shown by the number ‘1’ so as to make up a three dimensional macrame.
positives to negative surfaces, to make up the clear and seemingly continuous fluid we drink, swim in, and hold up umbrellas to keep off of us when it rains. They link by charge at angles, shown by the number ‘1’ so as to make up a three dimensional macrame.
To be ‘in solution’ means to have some charge to which water molecules can link up with by attraction. Calcium atoms are positive and become surrounded by a shell of water molecules facing it with their bare negative surfaces. Oxalic and phosphoric acids have negative charges and are surrounded by water molecules pointing their positive or hydrogen sides to them.
Uric acid at neutral pH has its one negatively charged nitrogen water can grasp. But when pH falls, and neither nitrogen has any extra charge for water to bind with, how can the molecule remain among the water molecules? It cannot. The molecules stack into solid crystals and fall from solution.
Uric acid stone formers
The stones can be orange – red, large, and numerous
The stones can be red or orange because uric acid crystals absorb hemoglobin breakdown products that are red – orange pigments in urine. Sometimes uric acid crystals pass in urine as a red orange gravel.
Uric acid does not have to connect itself to some other atom or molecule to make a crystal, in the way that calcium must bond with oxalate or phosphate ions to make calcium oxalate or calcium phosphate crystals. When pH is low enough to extinguish its charge, uric acid can crystallize very fast, in seconds, and pass as an orange gravel in the urine. If retained, such crystals can grow rapidly into large stones. Because there is much more uric acid in urine than there is oxalic acid, uric acid stones can grow very large and rapidly. Some fill up the entire collecting system of the kidney.
Urine pH controls stone formation
But because the whole process depends almost completely on the acidity of the urine, uric acid stones are very easy to treat. Just a modest amount of supplemental alkali will make the urine of almost any patient alkaline enough that the hydrogen atoms are removed from the one crucial charged nitrogen. Water can bond there so uric acid remains in solution. Because so simple, treatment prevents stones with certainty. Relapse need never occur.
Mixed stones require special care
Unfortunately, however, stones commonly contain uric acid mixed with calcium oxalate. In this case, one needs to track down the cause of the calcium oxalate stones as well as make the urine alkaline enough to stop uric acid stones from forming. Calcium phosphate crystals mix with uric acid only rarely, because it takes a rather alkaline urine to remove the hydrogen atoms from phosphate so it has two negative charges and can bind efficiently with calcium atoms. At that higher pH, uric acid will have its charge site and remain in solution.
Struvite stones
Urea and the planet
Kidneys cannot make struvite. Bacteria make it. Not all bacteria, either. It takes bacteria that normally thrive in the soil, and they do it for ancient and compelling reasons. These bacteria produce the kidney stone named Struvite after Heinrich Christian Gottfried von Struve (1772–1851).
Animals deposit urea (at left) all over the planet when they urinate. Plants cannot use it.
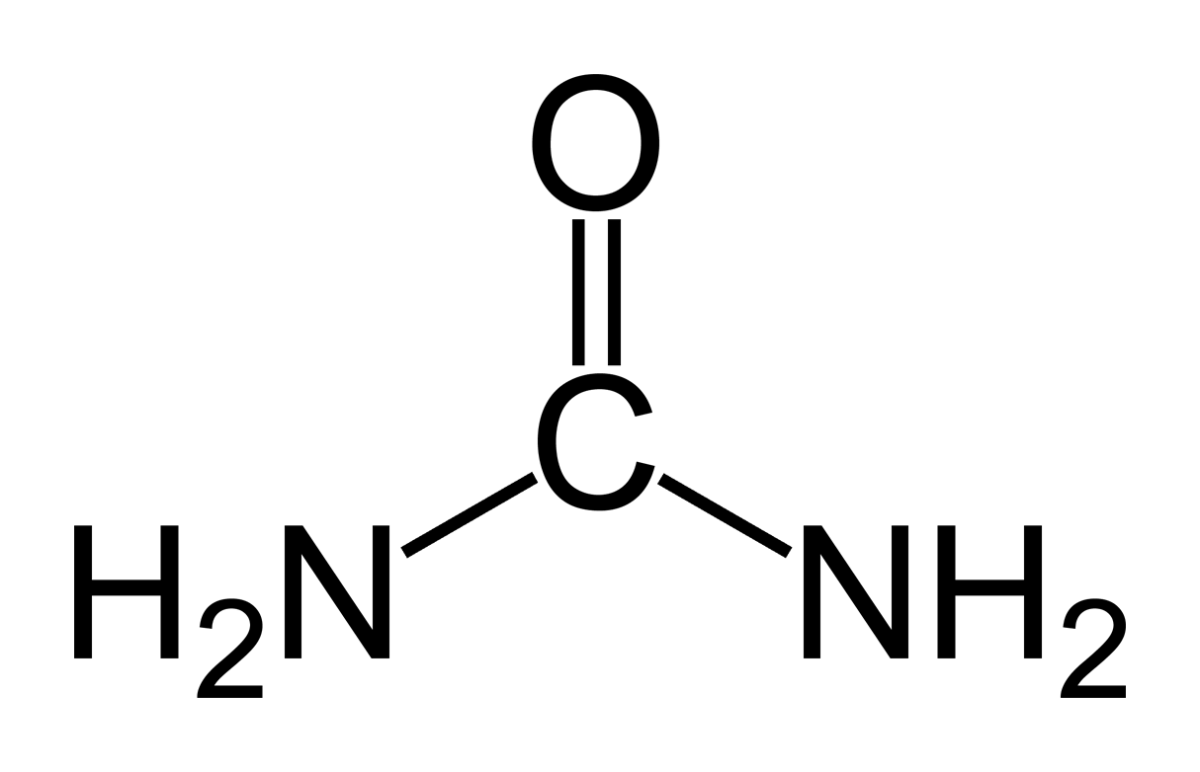 Like oxygen, nitrogen is an essential for life yet dangerous. It is integral to proteins, DNA and RNA. As these molecules are broken down and remade, some of their nitrogen slips by and can form poisonous compounds unless caught up in safe waste products. Of these, the main one, urea, contains 2 nitrogen atoms bound to a single carbon atom (‘C’ in the picture to your left).
Like oxygen, nitrogen is an essential for life yet dangerous. It is integral to proteins, DNA and RNA. As these molecules are broken down and remade, some of their nitrogen slips by and can form poisonous compounds unless caught up in safe waste products. Of these, the main one, urea, contains 2 nitrogen atoms bound to a single carbon atom (‘C’ in the picture to your left).
Uric acid contains 4 nitrogen atoms (look back at the picture of it). Birds and reptiles excrete most of their nitrogen as uric acid; mammals like us excrete nitrogen mainly as urea.
As the animals of the world urinate on the soil, their urea brings nitrogen to plant roots, but the plants cannot use it. They cannot release the nitrogens from the carbon atom that holds them. Those soil bacteria that make struvite crystals have an enzyme, called urease, that can release the nitrogen for plants to use as their nitrogen supply.
So, soil bacteria with urease maintain the nitrogen cycle of the earth.
Struvite crystals
As they release nitrogen from its carbon in urea, the nitrogen takes up a proton making ammonia (NH3). Ammonia is a powerful alkali and takes up another proton.
As it does so, the working bacteria surround themselves with spheres of very alkaline fluid enriched with ammonium ion (NH4) that carries one positive charge. Soil magnesium ( an atom with two positive charges) and phosphate sans all of its protons (an ion with three negative charges) spontaneously form their triple salt: three negative phosphate charges, two positive from magnesium, one positive from NH4).
The crystals anchor the bacteria and help create a porous nitrogen rich soul good for plants to grow in
The struvite kidney stone
Why they start
Because urine is filled with urea, soil bacteria that get into the urinary tract can break it down to ammonia and create struvite from the magnesium and phosphate urine always contains.
You might wonder how soil bacteria get into the urinary system.
Because we eat them, with foods that are not cooked, and they become part of the intestinal bacterial population from an early age. In us and around us, they find a way into the urinary system, especially in women whose shorter urethra makes entry easier. No matter how skillfully used, any instrument put into the bladder can carry our personal soil bacteria with it.
What they do
Because they live among molds and fungi, soil bacteria easily mount resistances to antibiotics, so antibiotics given for a urinary tract infection will tend to kill sensitive bacteria and select out those that can resist them.
Soil bacteria can produce struvite stones de novo, or infect calcium stones to produce a mixed stone. Either way, struvite stones are infected by their very nature. They can become huge. Their bacteria can injure the kidneys, even enter the bloodstream and cause sepsis.
Treatment is a mix of thoughtful surgery and selection of antibiotics after such surgery to kill bacteria that remain. If the stones are a mixture of struvite and calcium crystals, new calcium stones need to be prevented.
Cystine stones
Inherited kidney abnormality
 Lemon yellow with a sugary coating these form only in people who have an inherited kidney disorder called cystinuria.
Lemon yellow with a sugary coating these form only in people who have an inherited kidney disorder called cystinuria.
Although the kidneys function well, they permit abnormal amounts of four amino acids to enter the urine. Three do not matter that we know of. The fourth makes crystals and the cystine kidney stone type.
Cystine
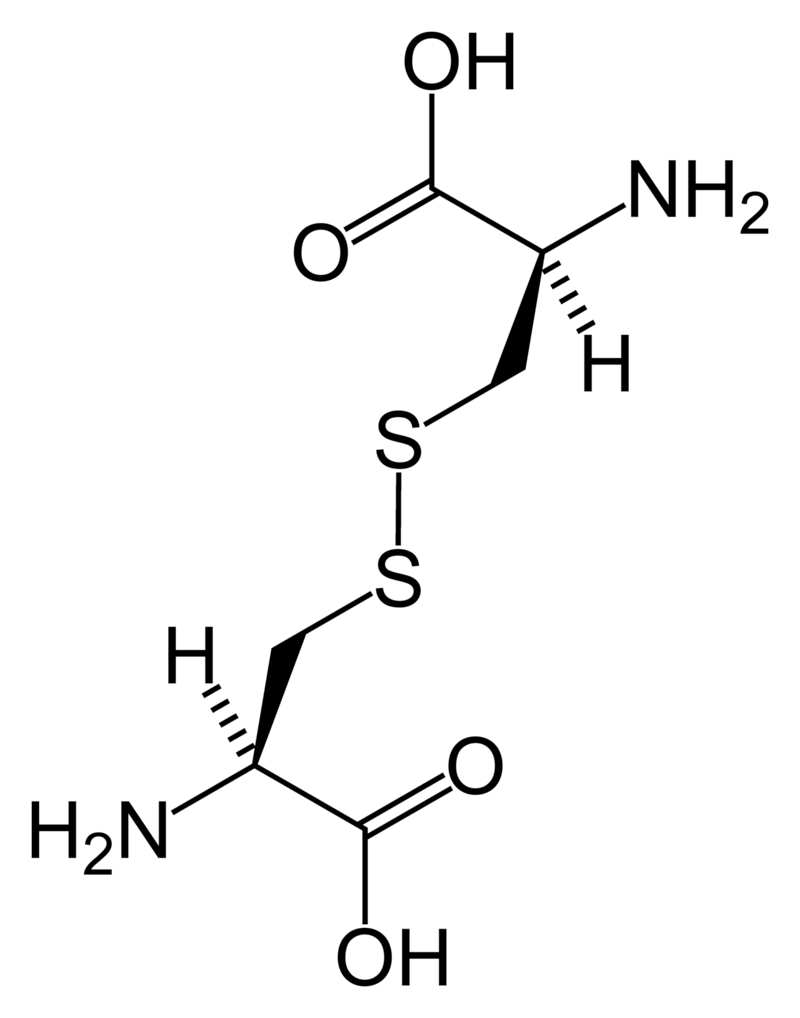
Cystine (left) forms through the coupling of two identical amino acids – called cysteine – through their sulfur atoms (‘S’ in the line drawing).
Each cysteine contains two carbon atoms – not shown except as corners – bonded together (shown by the single long line that connects the two corners) as in oxalic acid.
One carbon atom has 2 oxygens bonded to it; the other has one nitrogen (which makes it an amino – nitrogen containing – acid), a hydrogen atom, and a sulfur atom. As for phosphate, the dashed and solid arrows simply mean the hydrogens and sulfurs lie above and below the plane of the page and a stick model would have a three dimensional shape.
Cystine Crystals
Cysteine itself is very soluble because the sulfur atom has an appreciable negative charge.
But the big, long cystine molecule has very little charge because the sulfurs bind to each other. So, like uric acid, cystine loses intimacy with water molecules and simply leaves the solution as crystals. Also like uric acid, the process is fast.
Cystine stones
Because people with cystinuria lose large amounts of cystine in their urine stones readily grow large, and fast.
Stones probably form in the urine itself. But cystine crystals can plug the ends of kidney tubules, as calcium phosphate crystals do, causing cell damage.
Since cystinuria is an inherited disease, stones may begin in childhood.
Effective treatment always requires very large amounts of fluids to dilute the urine. The few effective drugs resemble cysteine. Their sulfur groups bond with cysteine to form a ‘mixed disulfide’ more soluble than cystine. But their side effects can limit use.
Rare stones
Here and there we find patients who make uncommon crystals and require very special care.
Uric acid, as an example, can form odd crystals such sodium or ammonium acid urate, especially in people with bowel disease and chronic diarrhea.
Anti-viral drugs can crystallize in urine and form stones only recognized for what they are through stone analysis.
Very rare disorders of metabolism can produce molecules which crystallize in the urine, for example 2-8 dihydroxyadenine.
Although it can take a while before the right answer emerges, stone analyses will put physicians on the right track for these special cases.
The end of a very long post
That’s my parade.
The common animals and the rarer animals have gone by, and you have glimpsed the main ones, big and small.
The one point is what it was at the beginning. Each kind of kidney stone has its own ways, and treatment requires we know which one you have.
Likewise, for whatever that one may be, it is good to know as much about it as you can know. For long term prevention of stones is hard to come by and ultimately what the patience and and consistency of patients themselves matters most.
If you don’t know which stones you have made, find out.
Track down old reports and pull them together.
Keep copies and send everything to the doctors who care for you.
Fred Coe MD
Fix your typos
Hi Marsha, It is easy to say, and not wrong. But in fact very hard to accomplish. This site has well over 100 articles with an average of about 5000 words, meaning about 500,000 words in all. Most of those I have written myself. I try to be accurate but writing solo has its limits. I have no resources to pay an editor or even pay people to help in editing. I accept no sponsors nor ads, have no paywall, and ask for no contributions. My university offers no funds, either. I have done it in the service of world stone prevention, and as a way of giving back to as many people as I can for all the support I have received in life from public grant moneys and a life as a professor. So I have always had two alternatives. Simply not do this kind of public offering and have a more perfect public facade, or do it and reveal some visible flaws of performance for people to not incorrectly criticize. I mean by this, my books, research articles, and medical reviews are published by commercial houses that can afford editors, so typos are rare enough. But few can read them. Many are behind publisher paywalls. So, there you have it. One person writing so much, unsupported and his own editor, and doing it in spare time – I am employed otherwise, can not achieve what he would view as his own ideal. Nor yours. Regards, Fred Coe
Hi Dr. Coe. I am so thankful for your website. It has helped me in many ways. Please have as many typos as happen to come up while providing this valuable information….. and to personally respond to each persons plea for help in regards to their personal situation….hundreds of people. I wish my own doctor took the time to provide me with even the most basic information, and I am paying him. Thank you for giving so much of yourself! Also, I have spent hours reading your articles and unlike Marsha I have noticed far more typos in the 5 newspapers I read regularly than here. You were far more gracious in your reply than I would have been… but that is one of my visible flaws. We all have them. Thank you for choosing to publicly display yours.
Hi Cathy, I guess some people respond more to typos than others. As I work alone they are so hard to catch! Thanks for the kind words, and that you find the site worthwhile. Regards, Fred
Hi
Dr. Coe
I am currently being evaluated as a kidney donor for my sister. They suspected kidney stones from a scan. My 24 hour had one elevation which Brishite 2.80
What is this exactly and do you feel it will impead my ability to be a donor?
Thanks!
Hi Cheri, Here we do not use anyone with more than one or perhaps 2 stones, small ones, and no prior stone passage, and also 24 our urine testing must show no important stone risk such as high urine calcium or oxalate excretion. You are at best a marginal candidate, and probably will not be accepted. Regards, Fred Coe
Hi
Dr. Coe
I am currently being evaluated as a kidney donor for my sister. They suspected kidney stones from a scan. My 24 hour had one elevation which Brishite 2.80
What is this exactly and do you feel it will impead my ability to be a donor?
Thanks!
Hi Cheri, Here we do not use anyone with more than one or perhaps 2 stones, small ones, and no prior stone passage, and also 24 our urine testing must show no important stone risk such as high urine calcium or oxalate excretion. You are at best a marginal candidate, and probably will not be accepted. Regards, Fred Coe
Hi Dr Coe, thank you for all the information and work creating this website, appreciate your time and effort.
I had excruciating pain in my side, unbearable accompanied with nausea and vomiting. Went to hospital and they suspected kidney stones, gave me I.V and pain killers. Upon researching before stumbling across your site, I came across lemon juice, apple cider vinegar and baking soda to provide help in breaking up stones? I increased my water intake, I know I don’t drink enough water and for some reason am hardly ever thirsty, also sweat very little compared to most people which I attributed my lack of thirst, still I do make an effort to drink water and force myself before bedtime especially. I also noticed on your list of high oxalate foods that spinach is the highest, which I eat everyday at least two or three times per day, in salads or juices/smoothies. I also consume almonds and cashew daily too, I’ve been eating these high oxalate foods especially spinach in large amounts for ten years. Plus I stopped drinking dairy over ten years ago. I’m 37 years old, eat clean and workout. My self diagnosis so far is lack of water, consuming high oxalate foods and possible low calcium intake.
I had an ultra sound which states I have “sand” in both kidneys? I’m currently in Mexico and thats the most information I could gather via using google translate speaking with the clinic. I started drinking lemon juice and now baking soda, two days after my hospital episode I passed a 4mm stone, from searching pictures on the internet it looks like a COAX stone in my opinion.
So my question is, if I were to assume its a COAX stone does lemon juice and baking soda help prevent and break up stones? What is this “sand” they are referring to and is sand just tiny particles built up? Hopefully not the size of stones and therefore should pass with increased water intake?
Please let me know your thoughts and thanks in advance, regards!
Hi Jay, If you can, have the stone analysed so you know what it is. Given inadequate fluids and a high oxalate diet, you may have an answer as to cause, but do not omit a proper and organized evaluation. Here is a reasonable plan. YOur present remedies are just that; figure out the cause and use specific long term treatments. Regards, Fred Coe
Hi Dr Coe, thank you for all the information and work creating this website, appreciate your time and effort.
I had excruciating pain in my side, unbearable accompanied with nausea and vomiting. Went to hospital and they suspected kidney stones, gave me I.V and pain killers. Upon researching before stumbling across your site, I came across lemon juice, apple cider vinegar and baking soda to provide help in breaking up stones? I increased my water intake, I know I don’t drink enough water and for some reason am hardly ever thirsty, also sweat very little compared to most people which I attributed my lack of thirst, still I do make an effort to drink water and force myself before bedtime especially. I also noticed on your list of high oxalate foods that spinach is the highest, which I eat everyday at least two or three times per day, in salads or juices/smoothies. I also consume almonds and cashew daily too, I’ve been eating these high oxalate foods especially spinach in large amounts for ten years. Plus I stopped drinking dairy over ten years ago. I’m 37 years old, eat clean and workout. My self diagnosis so far is lack of water, consuming high oxalate foods and possible low calcium intake.
I had an ultra sound which states I have “sand” in both kidneys? I’m currently in Mexico and thats the most information I could gather via using google translate speaking with the clinic. I started drinking lemon juice and now baking soda, two days after my hospital episode I passed a 4mm stone, from searching pictures on the internet it looks like a COAX stone in my opinion.
So my question is, if I were to assume its a COAX stone does lemon juice and baking soda help prevent and break up stones? What is this “sand” they are referring to and is sand just tiny particles built up? Hopefully not the size of stones and therefore should pass with increased water intake?
Please let me know your thoughts and thanks in advance, regards!
Hi Jay, If you can, have the stone analysed so you know what it is. Given inadequate fluids and a high oxalate diet, you may have an answer as to cause, but do not omit a proper and organized evaluation. Here is a reasonable plan. YOur present remedies are just that; figure out the cause and use specific long term treatments. Regards, Fred Coe
LAS MUESTRAS CONSISTEN DE VARIOS FRAGMENTOS DE CÁLCULO IRREGULARMENTE FORMADOS, PESANDO UN TOTAL DE 133 MILLIGRAMOS
LOS FRAGMENTOS DE CÁLCULO ESTÁN COMPUESTOS DE MASAS COMPACTAS DE ORIENTACIÓN ALEATORIA A LAS AGUJAS MONOCLÍNICAS RADALES DE MONOHIDRATO DE OXALATO DE CALCIO, CON DEPÓSITOS INTERNOS DE APATITO MICROCRISTALINO DE HIDROXILO. LOS OCTAHEDRONES DE DIHIDRATO DE OXALATO DE CALCIO ESTÁN EMPOTRADOS EN LAS PERIFERÍAS. LAS MATRICES DE PROTEÍNA ESTÁN DEMOSTRADAS.
Hi Pilar, I am afraid my Spanish is inadequate to reading what seems like a stone analysis report. But I would guess it is calcium oxalate monohydrate and dihydrate with the usual included protein matrix materials. It is the most common stone, but I have nothing more to add. Regards, Fred Coe
LAS MUESTRAS CONSISTEN DE VARIOS FRAGMENTOS DE CÁLCULO IRREGULARMENTE FORMADOS, PESANDO UN TOTAL DE 133 MILLIGRAMOS
LOS FRAGMENTOS DE CÁLCULO ESTÁN COMPUESTOS DE MASAS COMPACTAS DE ORIENTACIÓN ALEATORIA A LAS AGUJAS MONOCLÍNICAS RADALES DE MONOHIDRATO DE OXALATO DE CALCIO, CON DEPÓSITOS INTERNOS DE APATITO MICROCRISTALINO DE HIDROXILO. LOS OCTAHEDRONES DE DIHIDRATO DE OXALATO DE CALCIO ESTÁN EMPOTRADOS EN LAS PERIFERÍAS. LAS MATRICES DE PROTEÍNA ESTÁN DEMOSTRADAS.
I have received a report that the kidney stone is 100% protein. What does that mean and what is the significance. Thank you for your expertise in this matter!
Hi Janet, Protein stones are uncommon and I do not know why they form. But sometimes they are simply crystal aggregates that have taken up a lot of urine proteins so the crystal itself does not show up on FTIR analysis. These stones can be a lot of trouble – symptoms when they pass. I would look for standard causes of stones – crystal risks – and reverse them. Here is my standard plan. Regards, Fred Coe
Thank you for such a prompt and complete answer! Janet
I have received a report that the kidney stone is 100% protein. What does that mean and what is the significance. Thank you for your expertise in this matter!
Hi Janet, Protein stones are uncommon and I do not know why they form. But sometimes they are simply crystal aggregates that have taken up a lot of urine proteins so the crystal itself does not show up on FTIR analysis. These stones can be a lot of trouble – symptoms when they pass. I would look for standard causes of stones – crystal risks – and reverse them. Here is my standard plan. Regards, Fred Coe
Thank you for such a prompt and complete answer! Janet
Hi, Dr. Coe,
Thank you for all the information on this website. Two weeks ago I had to get surgery for a 10x8mm kidney stone stuck in my ureter just above the bladder. It has been a very painful couple of months that I would never want to repeat. This is the second episode of stones in 2 years; however, this is the first time for surgical removal. Any advice you can provide to avoid another repeat performance? My stone tested 90% Calcium oxalate monohydrate and 10% Calcium phosphate (apatite). Thank you in advance!
Hi Kim, The whole site is about prevention. Here is a good starting place. Read through the links, too. Regards, Fred Coe
Thank you so much
Hi, Dr. Coe,
Thank you for all the information on this website. Two weeks ago I had to get surgery for a 10x8mm kidney stone stuck in my ureter just above the bladder. It has been a very painful couple of months that I would never want to repeat. This is the second episode of stones in 2 years; however, this is the first time for surgical removal. Any advice you can provide to avoid another repeat performance? My stone tested 90% Calcium oxalate monohydrate and 10% Calcium phosphate (apatite). Thank you in advance!
Hi Kim, The whole site is about prevention. Here is a good starting place. Read through the links, too. Regards, Fred Coe
Thank you so much
Dr. Fred Coe,
I passed a stone in Dec 2016. It was a 5mm x 4mm x 3mm stone. I was told from my previous doctor that it was the only one i had left (I had a scan done from a hospitalization for stones). The past 2 months I have passed 2 stones and know I currently have atleast two 2mm ones still in one of my kidneys. I seem to be growing them at a fast rate. The only stone I was able to collect has been the one from Dec 2016. I was just recently able to get it tested. I got my results back about 2 weeks ago. My results were: 5% Calcium Oxalate Di-Hydrate, 55% Calcium Oxalate Monohydrate, and 40% Calcium Phosphate. For the most part I know how to adjust my diet but from what I can understand the CP seems higher than normal and that diet alone doesn’t do anything to them. I am taking a magnesium supplement, a B- Vitamin complex, Grapefruit seed extract to help my undiagnosed IBS (came from my doctor, he wanted to see if it would clear up the potential “IBS”), and 4 pills a day of Himalaya Uricare. He told me that the Uricare would dissolve the stones. I’ve been looking into taking Pomegranate supplements to help as well. I’m only 29 years old and I’ve been in the hospital passing numerous stones for the past 3.5 years. I’ve had a nephrostemy tube placed in while pregnant before and then removed after I gave birth. I’ve also had to have a stent placed in my right ureter and eventually removed as well. I’m not sure what else to do and the 40% seems higher than what I have researched to be the norm for that type. Any advice and/or help is greatly appreciated. Thank you for your time!
Hi Natasha, You are forming calcium oxalate/calcium phosphate stones, and trying to find a remedy. This is not ideal and can become very confusion very fast. Here is a good starting article on how to find a better way. Here is an article about calcium phosphate stone formers – which you are. The approach to every stone former is more or less by rote, and here is a reliable way. By no means try to cast around for remedies, real treatment follows knowing cause and it works. In particular with tubes in place you need to stop crystallization now, before complications set in. Regards, Fred Coe
Thank you for your reply and information. I will definitely read your suggested links and follow through.
Hi Natasha… I’ve been on a somewhat similar roll. Try out distilled water if you haven’t yet. It helped me a lot.
I pass 4-8mm stones calxium phosphate stones every single year. I get ESWL pretty much annually. I also take migraine medicine ( zonisamide ) daily which can cause kidney stones although I was getting them prior to the medication. This is the only medicine that works for my migraines. I was just out of work for a month because of a 6×8 mm stone blockage in my ureter that resulted in a kidney infection that my Dr couldn’t detect because it didn’t show up in my urine so I became septic. Its a long story and was hell. Anyway, my Dr says there is nothing I can do to prevent my stones. Do you have any ideas? I don’t drink soda or caffeine already.
Please excuse any typos I’m on my cellphone.
Hi Julie, Your drug is a weak inhibitor of carbonic anhydrase and before stopping it – the usual advice – I would pursue standard prevention practices. Here is a good plan. Assuming you have no systemic cause, here is my best overall treatment approach. If you have a systemic disease your physicians can treat it specifically. So there really is a lot you can have done, but your physicians need to be responsible and be sure you use them. Regards, Fred Coe
I pass 4-8mm stones calxium phosphate stones every single year. I get ESWL pretty much annually. I also take migraine medicine ( zonisamide ) daily which can cause kidney stones although I was getting them prior to the medication. This is the only medicine that works for my migraines. I was just out of work for a month because of a 6×8 mm stone blockage in my ureter that resulted in a kidney infection that my Dr couldn’t detect because it didn’t show up in my urine so I became septic. Its a long story and was hell. Anyway, my Dr says there is nothing I can do to prevent my stones. Do you have any ideas? I don’t drink soda or caffeine already.
Please excuse any typos I’m on my cellphone.
Hi Julie, Your drug is a weak inhibitor of carbonic anhydrase and before stopping it – the usual advice – I would pursue standard prevention practices. Here is a good plan. Assuming you have no systemic cause, here is my best overall treatment approach. If you have a systemic disease your physicians can treat it specifically. So there really is a lot you can have done, but your physicians need to be responsible and be sure you use them. Regards, Fred Coe
I just had a CT scan and they think my 5mm Stone is in the tissue of my right kidney. I have had issues over the last couple of years with kidney pain my last scan showed a 4 mm stone also right side in dec 2016. What will happen to the stone stuck in there if in fact it is can it grow? could it be the 4mm that has gotten bigger my Dr didn’t seem to think it is a problem but I don’t want more problems
Hi Gayleen, I presume this is a deposit within one or more kidney tubules. These are more common in calcium phosphate stone formers. WIthout more information, it is hard for me to offer more to you. Regards, Fred Coe
I just had a CT scan and they think my 5mm Stone is in the tissue of my right kidney. I have had issues over the last couple of years with kidney pain my last scan showed a 4 mm stone also right side in dec 2016. What will happen to the stone stuck in there if in fact it is can it grow? could it be the 4mm that has gotten bigger my Dr didn’t seem to think it is a problem but I don’t want more problems
Hi Gayleen, I presume this is a deposit within one or more kidney tubules. These are more common in calcium phosphate stone formers. WIthout more information, it is hard for me to offer more to you. Regards, Fred Coe
With MSK, I form a lot of stones. I am on an aggressive treatment plan over the past month. Previously stone composition was 98% calcium ox dihydrate 2% monhydrate. Last month composition changed after many years and now is 93% monohydrate,4% dihydrate,and 3% carbonate apatite. The stone composition is harder now with this change as I understand. Is this serious? My goal of course is prevention,but is there anything I can do to change the composition? How to change mono to dihydrate so stones are softer and more responsive to treatment?
Hi Elan, these changes in stone composition are not really that remarkable but do point to a lower urine calcium with still too much oxalate – pure guess as when the stone actually formed as opposed to passed is unknowable. Rather than consider this change, I would focus on the serum and 24 hour urine data and see to reversion of whatever is causing the stones. MSK, if really present, often permits stones with rather little urine abnormality, and perhaps you are in that category. Regards, Fred Coe
With MSK, I form a lot of stones. I am on an aggressive treatment plan over the past month. Previously stone composition was 98% calcium ox dihydrate 2% monhydrate. Last month composition changed after many years and now is 93% monohydrate,4% dihydrate,and 3% carbonate apatite. The stone composition is harder now with this change as I understand. Is this serious? My goal of course is prevention,but is there anything I can do to change the composition? How to change mono to dihydrate so stones are softer and more responsive to treatment?
Hi Elan, these changes in stone composition are not really that remarkable but do point to a lower urine calcium with still too much oxalate – pure guess as when the stone actually formed as opposed to passed is unknowable. Rather than consider this change, I would focus on the serum and 24 hour urine data and see to reversion of whatever is causing the stones. MSK, if really present, often permits stones with rather little urine abnormality, and perhaps you are in that category. Regards, Fred Coe
Hi, i’m 32 and within 2 years i’ve had 2 stones and 7 mild episodes treatable at home. (Calcium – Oxalate) I’ve been told I could perhaps have MSK, however, I have not gone in again to do the ultrasound to see if I get diagnosed. My main concern are these frequent episodes. What i mean by that is i’ll have mild kidney pain one day maybe two (for most of the entire day/days) and within two days of that, it starts with strong pressures in the rectum/ureter area turning into an excruciating pain in the pelvic area/ bladder. I usually take ibuprofen 800mg and if bad enough i’ll take percocet. This will last only about a day or two max. I went to my urologist about a year ago and he mentioned it could be from crystals being released from the kidney rather than a large form, stone. Ive been drinking lots of lemon water and distilled water and my episodes have decreased immensely. I just got one yesterday and so I wanted to get your thoughts and see if indeed this sounds like an action from crystals being released.
Hi Jamie, The minor attacks may well be crystals and they mean you are not fully treated. Here is a good article on proper evaluation – be sure you know what has caused the stones. Treatment has to protect more of you than just stone disease. Regards, Fred Coe
Thank you for your reponse Dr Coe. Based on many of your articles i’ve read, looks like my first stone was calcium/oxalate but these minor attacks i’ve had perhaps have become calcium phosphate. (Can you have MSK that are based on calcium phosphate crystals?) Without proper testing though, i’ve changed my diet so that my ph level is lowered so that my levels are more acidic and when eating .. i’ll combine foods that are rich in calcium and oxalate at the same time. (For example, i’ll eat beets with cheese). I can say I have been free of any attacks/kidney pain thankfully!!!
However, I now have these new symptoms… When stressed or emotional, i feel as though my blood pressure goes very high. My skin gets really red, i start to sweat profusely and feel sometimes as though i will pass out and chest pains. From some of your articles, i’m now wondering if my stones have opened up another pathway to medical problems.
Hi Jamie, Given these episodes perhaps you might want to purchase a home blood pressure machine and measure your blood pressure. If it is high, or not, determines what to do. I note ‘without proper testing’ but perhaps forgot why not. Regards, Fred Coe
I am checking on what to do to prevent stones and, hopefully, breaks some down. My husband has been passing multiple stones a year for the last few years. His last stone was 9mm and he had to have it broken up. He passed a 3.5 a few days later and hasn’t been able to pass the next one in the last 3 weeks. We had the stone evaluated (the 3.5) and it came back as Calcium Oxalate Monohydrate/Calcium Oxalate Dihydrate AND Calcium Phosphate Cabonate? It also stated Carbonate-Apatite on the paperwork. We would like to find out what he can do to prevent all of these. When they did another CAT scan (since he couldn’t pass this one in the last 3 weeks since the procedure) The result was that he had several 2mm stones down about to pass (I don’t remember the name of the position) and multiple more in both his left and right kidney. It would be great if we had a way to break them down, and ultimately prevent them completely.
Hi Jesse, Your husband has had many stones, and they have a cause. You cannot dissolve calcium stones but you can prevent them. Begin here: this article gives links into the preventions. This one links to the kidney stone book, also a lot about prevention. It works; do it. Regards, Fred Coe
I am checking on what to do to prevent stones and, hopefully, breaks some down. My husband has been passing multiple stones a year for the last few years. His last stone was 9mm and he had to have it broken up. He passed a 3.5 a few days later and hasn’t been able to pass the next one in the last 3 weeks. We had the stone evaluated (the 3.5) and it came back as Calcium Oxalate Monohydrate/Calcium Oxalate Dihydrate AND Calcium Phosphate Cabonate? It also stated Carbonate-Apatite on the paperwork. We would like to find out what he can do to prevent all of these. When they did another CAT scan (since he couldn’t pass this one in the last 3 weeks since the procedure) The result was that he had several 2mm stones down about to pass (I don’t remember the name of the position) and multiple more in both his left and right kidney. It would be great if we had a way to break them down, and ultimately prevent them completely.
Hi Jesse, Your husband has had many stones, and they have a cause. You cannot dissolve calcium stones but you can prevent them. Begin here: this article gives links into the preventions. This one links to the kidney stone book, also a lot about prevention. It works; do it. Regards, Fred Coe
I have a friend who gets recurrent stones. She was told that her most recent stones are composed of brushite. The urologist told her that there isn’t must research about these stones, other than the patients have frequent reoccurrences in stone production. Is there any more insight/research that you can provide?
Hi Azia, brushite stones are a variety of calcium phosphate stones and are prevented more or less in the usual ways. Here is my best on it. If you follow what the article says and you need meds as well as diet, – your friend, I mean, needs them – it is worthwhile as brushite stones do recur. Regards, Fred Coe
I have a friend who gets recurrent stones. She was told that her most recent stones are composed of brushite. The urologist told her that there isn’t must research about these stones, other than the patients have frequent reoccurrences in stone production. Is there any more insight/research that you can provide?
Hi Azia, brushite stones are a variety of calcium phosphate stones and are prevented more or less in the usual ways. Here is my best on it. If you follow what the article says and you need meds as well as diet, – your friend, I mean, needs them – it is worthwhile as brushite stones do recur. Regards, Fred Coe
Hello
I went into the ER with main about 6 weeks ago to find out I have a large 11mm kidney stone in my left ureter mid way down. I have 2 smaller stones in my lower pole area of my left kidney the larger is 6mm. And a small 3mm in my right kidney. I was booked for ESWL April 11. I was told that the 11mm stone was now at the bottom of the ureter on top of the bladder and the 2 stones in the left kidney were not seen by a KUB X-ray. I did have lots of pain and nausea before the ESWL. What I’m confused about is how did this large stone move down the ureter when it was large and stuck and where did these other 2 go. They couldn’t have passed due to this large one blocking? Then after the procedure I passed fragments for 24 hours and stopped. I was told to collect the fragments but I also urinated black powder with the brown/ tan fragments? I didn’t keep nobody told me this? Also after 48 hours I have no more fragments and my urine is clear again. Does this mean I am stone free?
Thank You
Robin
Hi Robin, The confusions are no doubt because the KUB x ray has poor resolution. If you have pain and there is doubt about where and how many stones are present an ultrasound would usually be helpful, and if needed a CT scan – though that involves unwanted radiation. Of course it is your urologist who needs to do whatever is needed here, and I am a simple bystander. So take my remarks for what they are and consult him/her to be sure about things. But it is not sure that stones are gone just because the urine is clear. Obstruction is always a hazard and your urologist has all the responsibility to assure against it. Regards, Fred Coe
Hello
I went into the ER with main about 6 weeks ago to find out I have a large 11mm kidney stone in my left ureter mid way down. I have 2 smaller stones in my lower pole area of my left kidney the larger is 6mm. And a small 3mm in my right kidney. I was booked for ESWL April 11. I was told that the 11mm stone was now at the bottom of the ureter on top of the bladder and the 2 stones in the left kidney were not seen by a KUB X-ray. I did have lots of pain and nausea before the ESWL. What I’m confused about is how did this large stone move down the ureter when it was large and stuck and where did these other 2 go. They couldn’t have passed due to this large one blocking? Then after the procedure I passed fragments for 24 hours and stopped. I was told to collect the fragments but I also urinated black powder with the brown/ tan fragments? I didn’t keep nobody told me this? Also after 48 hours I have no more fragments and my urine is clear again. Does this mean I am stone free?
Thank You
Robin
Hi Robin, The confusions are no doubt because the KUB x ray has poor resolution. If you have pain and there is doubt about where and how many stones are present an ultrasound would usually be helpful, and if needed a CT scan – though that involves unwanted radiation. Of course it is your urologist who needs to do whatever is needed here, and I am a simple bystander. So take my remarks for what they are and consult him/her to be sure about things. But it is not sure that stones are gone just because the urine is clear. Obstruction is always a hazard and your urologist has all the responsibility to assure against it. Regards, Fred Coe
My kidney stone was Carbonate Apatite 90% and calcium oxalate 10%. I can find a lot of information on the calcium oxalate but not on Carbonate Apatite and since this was the bulk of my stone I would like to know more about it and if there is preventative measures that can be taken. I was 36 weeks pregnant when my stone had to be surgically removed and I want to ensure this doesn’t happen in my next pregnancy early on.
Hi Ashley, calcium phosphate stones are a bit special, because most common in young women. Here is an article about them. Treatment is much like for calcium oxalate stones except that potassium citrate may not be ideal. Be sure and have your physicians do a full evaluation; often the stones are ascribed to pregnancy but I doubt that in most cases. Regards, Fred Coe
Ashley,
I had a kidney stone removed almost two months after having my daughter in December. It was 10% calcium oxalate dihydrate, 45% calcium oxalate monohydrate, and 45% carbonate apatite, about 7-8mm. I wondered if the pregnancy had anything to do with it as I was sick for the first five months! I could barely eat or drink and when I finally could, I wasn’t on my best behavior. I just signed up for Jill Harris’ course and am hoping she can give me more insight and see what I need to do to prevent future stones.
Hi Amanda, YOur stone has a lot of calcium phosphate in it (carbonate apatite); given this kind of stone prevention is very important. Pregnancy vitamins perhaps played a role, but you need a full evaluation when you have stopped nursing – if you are doing that. From the results you will need to plan treatment. Here is a pretty good article on the calcium phosphate stone, and on treatment of calcium kidney stones. Regards, Fred Coe
My kidney stone was Carbonate Apatite 90% and calcium oxalate 10%. I can find a lot of information on the calcium oxalate but not on Carbonate Apatite and since this was the bulk of my stone I would like to know more about it and if there is preventative measures that can be taken. I was 36 weeks pregnant when my stone had to be surgically removed and I want to ensure this doesn’t happen in my next pregnancy early on.
Hi Ashley, calcium phosphate stones are a bit special, because most common in young women. Here is an article about them. Treatment is much like for calcium oxalate stones except that potassium citrate may not be ideal. Be sure and have your physicians do a full evaluation; often the stones are ascribed to pregnancy but I doubt that in most cases. Regards, Fred Coe
Ashley,
I had a kidney stone removed almost two months after having my daughter in December. It was 10% calcium oxalate dihydrate, 45% calcium oxalate monohydrate, and 45% carbonate apatite, about 7-8mm. I wondered if the pregnancy had anything to do with it as I was sick for the first five months! I could barely eat or drink and when I finally could, I wasn’t on my best behavior. I just signed up for Jill Harris’ course and am hoping she can give me more insight and see what I need to do to prevent future stones.
Hi Amanda, YOur stone has a lot of calcium phosphate in it (carbonate apatite); given this kind of stone prevention is very important. Pregnancy vitamins perhaps played a role, but you need a full evaluation when you have stopped nursing – if you are doing that. From the results you will need to plan treatment. Here is a pretty good article on the calcium phosphate stone, and on treatment of calcium kidney stones. Regards, Fred Coe
I just passed another kidney stone this morning and I am on a regular cycle of one every year to two years. The first stone and second stone that I passed were crushed and examined and I was told that they were calcium citrate stones. I cannot find any information on them. The last CT scan of my kidneys 10 years ago showed that I had 12 in one kidney and 8 in the other. I was told to eliminate almost all of my diet at that time, which I refused because they could not tell me it would help with any certainty. They suggested no red meat, broccoli, citrus fruits, or dairy products. I have since been diagnosed with celiac disease (like my mother) and I am wondering where I can get more info. I will be going to my physician with the new stone for analysis and treatment soon.
Dear Brian, I suspect the stone analysis is faulty; calcium citrate is so soluble a salt one cannot imagine a stone made of it. Celiac disease is a form of malabsorption and could promote calcium oxalate stones – perhaps what you form. I presume your physicians are expert in the area of Celiac disease, so just mention to them about the possibility of increased urine oxalate from that condition. They may have already considered this possibility. You have a complex problem. Regards, Fred Coe
I just passed another kidney stone this morning and I am on a regular cycle of one every year to two years. The first stone and second stone that I passed were crushed and examined and I was told that they were calcium citrate stones. I cannot find any information on them. The last CT scan of my kidneys 10 years ago showed that I had 12 in one kidney and 8 in the other. I was told to eliminate almost all of my diet at that time, which I refused because they could not tell me it would help with any certainty. They suggested no red meat, broccoli, citrus fruits, or dairy products. I have since been diagnosed with celiac disease (like my mother) and I am wondering where I can get more info. I will be going to my physician with the new stone for analysis and treatment soon.
Dear Brian, I suspect the stone analysis is faulty; calcium citrate is so soluble a salt one cannot imagine a stone made of it. Celiac disease is a form of malabsorption and could promote calcium oxalate stones – perhaps what you form. I presume your physicians are expert in the area of Celiac disease, so just mention to them about the possibility of increased urine oxalate from that condition. They may have already considered this possibility. You have a complex problem. Regards, Fred Coe
I’m a 44yo male, had my first kidney stone at age of 18. Since then I have had over 20. I was told they are Calcium oxalate stones when they checked (15yrs. Ago).
Anyway, since I had so many, I thought I just knew when to go to the doc. I’d just do the “home remedies” and pass them… and some did. But what I didn’t know was there was a 15mm Stone stuck in my left uriter. And I couldnt even feel it. Long story short, after about 4 years of not passing any stones this one had got sick. It turned out that that stone had caused some major problems and they estimated that it has been stuc for nearly 4 yrs. I ended up needing to get my left kidney removed in an emergency surgery.
Don’t ignore any symptoms! It’s best to check with a doctor when symptoms start. Lack of Pain is a poor sign that something is wrong. If you’ve had a kidney stone before, you know what to look for. A check is better than the alternative.
Thanks for the article. I wish that this info would have been available when Instarted getting kidney stones in the 90’s.
Hi Jon, Loss of a kidney from painless obstruction – so unfortunate! Prevention is now a big deal for you. They can come again. Here is a good place to start. Regards, Fred Coe
I’m a 44yo male, had my first kidney stone at age of 18. Since then I have had over 20. I was told they are Calcium oxalate stones when they checked (15yrs. Ago).
Anyway, since I had so many, I thought I just knew when to go to the doc. I’d just do the “home remedies” and pass them… and some did. But what I didn’t know was there was a 15mm Stone stuck in my left uriter. And I couldnt even feel it. Long story short, after about 4 years of not passing any stones this one had got sick. It turned out that that stone had caused some major problems and they estimated that it has been stuc for nearly 4 yrs. I ended up needing to get my left kidney removed in an emergency surgery.
Don’t ignore any symptoms! It’s best to check with a doctor when symptoms start. Lack of Pain is a poor sign that something is wrong. If you’ve had a kidney stone before, you know what to look for. A check is better than the alternative.
Thanks for the article. I wish that this info would have been available when Instarted getting kidney stones in the 90’s.
A few years ago my doctor in another city removed a crystal from my knee fluid that he labeled calcium dihydrate. I have the photo and it looks like a 4-leaf cover with the leaves almost touching. I also have a Mayo diagnosis of hyperoxaluria, from an unknown cause. Is a calcium dihydrate crystal the same thing as calcium oxalate, or is it calcium phosphate, or something else? I am trying to figure out if my stone disease is also the mechanism causing joint degeneration. I didn’t have the photo at the time I went to Mayo, and my doctor at Mayo has now retired. Her replacement is unavailable for the foreseeable future.
Hi Chris, You are alarming me. If you have a form of primary hyperoxaluria – what Mayo works on – you need to stay in touch with Mayo or another equivalent center as the disease is dangerous and almost no physicians in usual practice know enough about it. The retired physician is no doubt Dawn Milliner and I am sure she would not want one of her PH patients without an appointment. The joint crystal may well be calcium oxalate because in what I surmise is your condition plasma oxalate levels can be above normal. Be careful, call Mayo back; feel free to use my name and refer to this note. My colleague there who specializes in hyperoxaluria is Dr John Lieske, and he would certainly want you to have ideal care. Regards, Fred Coe
A few years ago my doctor in another city removed a crystal from my knee fluid that he labeled calcium dihydrate. I have the photo and it looks like a 4-leaf cover with the leaves almost touching. I also have a Mayo diagnosis of hyperoxaluria, from an unknown cause. Is a calcium dihydrate crystal the same thing as calcium oxalate, or is it calcium phosphate, or something else? I am trying to figure out if my stone disease is also the mechanism causing joint degeneration. I didn’t have the photo at the time I went to Mayo, and my doctor at Mayo has now retired. Her replacement is unavailable for the foreseeable future.
Hi Chris, You are alarming me. If you have a form of primary hyperoxaluria – what Mayo works on – you need to stay in touch with Mayo or another equivalent center as the disease is dangerous and almost no physicians in usual practice know enough about it. The retired physician is no doubt Dawn Milliner and I am sure she would not want one of her PH patients without an appointment. The joint crystal may well be calcium oxalate because in what I surmise is your condition plasma oxalate levels can be above normal. Be careful, call Mayo back; feel free to use my name and refer to this note. My colleague there who specializes in hyperoxaluria is Dr John Lieske, and he would certainly want you to have ideal care. Regards, Fred Coe
Hello,
I have just gotten home from my urologist after a night in the hospital, where I passed a 2 mm stone and they said they saw another 5mm in the upper pole of the same kidney (left).
I had a 5mm (right kidney) taken care of with ESWL a year ago, that stone was visible on x-ray – they told me this one was calcium. My doctor reviewed a CT I got last year and a 1mm stone was in the left kidney – I’m guessing it is now the 5mm that is still up there.
He said that the 5mm in my left kidney is most likely Uric Acid, because it doesn’t show up on X-Ray but does on CT? I just wanted to see if this is true. I would love to treat this stone the best way possible but don’t have any firm data on its composition. In short my questions would be how can you treat a stone based on composition if you none of it has come down to study.
Hi Alexander, I have two suggestions. Your physician can measure the HU (density on CT); uric acid stones have a low number vs. calcium stones, and this is a common thing to do. Your 24 your urine pH; If it is below 5.5 uric acid stones are plausible and one should raise the pH above 6 with potassium citrate salts. Of course, this requires you get an entire kidney stone urine panel so you know all of the stone risks and can assure in later measurements that the higher pH has not increased risk for calcium phosphate stones. This is what physicians do, so let your physician do it. Regards, Fred Coe
Hello,
I have just gotten home from my urologist after a night in the hospital, where I passed a 2 mm stone and they said they saw another 5mm in the upper pole of the same kidney (left).
I had a 5mm (right kidney) taken care of with ESWL a year ago, that stone was visible on x-ray – they told me this one was calcium. My doctor reviewed a CT I got last year and a 1mm stone was in the left kidney – I’m guessing it is now the 5mm that is still up there.
He said that the 5mm in my left kidney is most likely Uric Acid, because it doesn’t show up on X-Ray but does on CT? I just wanted to see if this is true. I would love to treat this stone the best way possible but don’t have any firm data on its composition. In short my questions would be how can you treat a stone based on composition if you none of it has come down to study.
Hi Alexander, I have two suggestions. Your physician can measure the HU (density on CT); uric acid stones have a low number vs. calcium stones, and this is a common thing to do. Your 24 your urine pH; If it is below 5.5 uric acid stones are plausible and one should raise the pH above 6 with potassium citrate salts. Of course, this requires you get an entire kidney stone urine panel so you know all of the stone risks and can assure in later measurements that the higher pH has not increased risk for calcium phosphate stones. This is what physicians do, so let your physician do it. Regards, Fred Coe
I currently just had surgery for several 10-15mm stones in my urethra. He said there were still several in a hard to read his place and needs to go back in. I have the same thing waiting on the othe other side to be fixed and double stints currently. Just got out of hospital because I was showing signs of septis. (Which I almost died from last year). I am so tired of being in pain and making these huge stones. My question is he says I have ammonium acid urate stones which is cause from excessive laxative abuse. I have not used laxative on a excessive basis. The dr prescribed me linzess to help with sluggish gut. Is this what is causing what can I do to help not produce them.
Hi Jennifer, I believe the linzess is indeed the cause. It alters ileal ion transport and causes potassium depletion. The crystal you make requires vast ammonium ion production yet a urine whose pH is near neutral – potassium depletion is the ideal cause. Stop the medicine and never use it again. Have your serum and 24 hour urine studies done for stone prevention – you will find the high ammonia and low potassium. When you have done a proper evaluation, the rest will be easy. You have a very serious problem with so many surgeries for such large stones, and sepsis is very dangerous. Regards, Fred Coe
I currently just had surgery for several 10-15mm stones in my urethra. He said there were still several in a hard to read his place and needs to go back in. I have the same thing waiting on the othe other side to be fixed and double stints currently. Just got out of hospital because I was showing signs of septis. (Which I almost died from last year). I am so tired of being in pain and making these huge stones. My question is he says I have ammonium acid urate stones which is cause from excessive laxative abuse. I have not used laxative on a excessive basis. The dr prescribed me linzess to help with sluggish gut. Is this what is causing what can I do to help not produce them.
Hi Jennifer, I believe the linzess is indeed the cause. It alters ileal ion transport and causes potassium depletion. The crystal you make requires vast ammonium ion production yet a urine whose pH is near neutral – potassium depletion is the ideal cause. Stop the medicine and never use it again. Have your serum and 24 hour urine studies done for stone prevention – you will find the high ammonia and low potassium. When you have done a proper evaluation, the rest will be easy. You have a very serious problem with so many surgeries for such large stones, and sepsis is very dangerous. Regards, Fred Coe
Finally caught stone, came back 100% Ammonium Urate Acid. Live in industrialized USA, Diabetic, Vegetarian and only medication Spironolactone (potassium sparing diuretic for blood pressure); never use laxatives. Worried about adding more potassium, interested in comment “The crystal you make requires vast ammonium ion production yet a urine whose pH is near neutral – potassium depletion is the ideal cause. ” Upcoming appt with urologist- primary doc told me to look up my stone on Google!!
Hi Louise, This is unusual. Your 24 hour urine data are essential to understand what is happening. If you would post them, I could try to comment. Regards, Fred Coe
Finally caught stone, came back 100% Ammonium Urate Acid. Live in industrialized USA, Diabetic, Vegetarian and only medication Spironolactone (potassium sparing diuretic for blood pressure); never use laxatives. Worried about adding more potassium, interested in comment “The crystal you make requires vast ammonium ion production yet a urine whose pH is near neutral – potassium depletion is the ideal cause. ” Upcoming appt with urologist- primary doc told me to look up my stone on Google!!
I am a RN and have had kidney stones for the last 20 yrs. Constant Surgeries to remove them. As I look at my records of PH over a lengthy time the PH runs between 5.5 -6.0 consistently. Stone Analysis: FIRST CONSTITUENT 70% Calcium phosphate (apatite) SECOND CONSTITUENT: 30% Calcium oxalate dihydrate . I have a ileostomy and no motility in my small intestine, I can only consume about 3-4 tablespoons of food and eat only once a day. No other health issus.
According to last ileostomy scope there was still food fragments in the small intestine after being NPO for 18 hrs. I grind all my food in grinder, eat lots of protein, very few carbs, some sugar in coffee. I do drink lots of fluid because my body feels constantly dry. My other labs appear unremarkable. I did have parathyroid tumor removed 2014. Calcium and other labs unremarkable. Im on very little meds, prilosec, B12 injections, and Vit D3. My bmi 18. I had surgery recently and the stones grew from 2mm to 9mm in 3 months. That seems like fast growth but Im not sure. Any advice or input you could give me would be very much appreciated.
Hi Annette, Ileostomy is a special kind of stone problem. The 24 hour urines I have studied show low sodium, low volumes, and high calcium oxalate and CaP supersaturations. Urine ammonia is high as a response to GI alkali loss. You do not mention 24 hour urine studies, so I cannot do more about the stone problem. In general, the issues are replenishment of alkali loss as sodium – not potassium alkali, and ways to increase urine volume despite the small bowel problems – one approach is to use beverages with glucose in them to facilitate jejunal fluid absorption. This is so complex a problem, however, that long distance and my relative ignorance of your details limits me to just these few general remarks. Regards, Fred Coe
I am a RN and have had kidney stones for the last 20 yrs. Constant Surgeries to remove them. As I look at my records of PH over a lengthy time the PH runs between 5.5 -6.0 consistently. Stone Analysis: FIRST CONSTITUENT 70% Calcium phosphate (apatite) SECOND CONSTITUENT: 30% Calcium oxalate dihydrate . I have a ileostomy and no motility in my small intestine, I can only consume about 3-4 tablespoons of food and eat only once a day. No other health issus.
According to last ileostomy scope there was still food fragments in the small intestine after being NPO for 18 hrs. I grind all my food in grinder, eat lots of protein, very few carbs, some sugar in coffee. I do drink lots of fluid because my body feels constantly dry. My other labs appear unremarkable. I did have parathyroid tumor removed 2014. Calcium and other labs unremarkable. Im on very little meds, prilosec, B12 injections, and Vit D3. My bmi 18. I had surgery recently and the stones grew from 2mm to 9mm in 3 months. That seems like fast growth but Im not sure. Any advice or input you could give me would be very much appreciated.
Hi Annette, Ileostomy is a special kind of stone problem. The 24 hour urines I have studied show low sodium, low volumes, and high calcium oxalate and CaP supersaturations. Urine ammonia is high as a response to GI alkali loss. You do not mention 24 hour urine studies, so I cannot do more about the stone problem. In general, the issues are replenishment of alkali loss as sodium – not potassium alkali, and ways to increase urine volume despite the small bowel problems – one approach is to use beverages with glucose in them to facilitate jejunal fluid absorption. This is so complex a problem, however, that long distance and my relative ignorance of your details limits me to just these few general remarks. Regards, Fred Coe
I have had my first surgery for kidney stones( several, most between 6-7mm). I had my stent taken out today. I am a petite 45 year old woman with diabetes. The breakdown of my stones were thus, 50% magnesium ammonia phosphate, 40% calcium phosphate, and 10% calcium oxalate dihydrate. The doctor assigned to me at the hospital is uncommunicative to say the least, and we are looking for a new urologist to get a urine analysis done. The only advice he gave me was to drink more water, which I already do(diabetic) and no pop(which I may have 1 can a month). I am concerned because medically I have had a lot of health problems in the past year and I am wondering if my kidneys and/ or thyroid is the underlying issue and is being overlooked. A few problems are: multiple UTIs(never had before), c-diff twice(again never had before) pneumonia, sciatica, anemia, low vitamin d, low iron, 2 blood transfusions (never had before) and the weirdest, I haven’t had a period for three years, and started again recently. There is more but these are the main ones I could remember. How do I pull all this information together to find a solution? Is it possible it could all be related, and if so, what type of doctor could look at all the information and see the underlying condition(s)? Right now, I am trying to find a urologist to have a urine analysis done ASAP, because I never want to experience this pain again. Sorry so windy, but I am getting desperate for medical communication until I find a new informative urologist that can ELI5. Thanks in advance, and if you have any recommendations for urologists in Columbus, Ohio, I would love to have them. Thanks again, Karen
Hi Karen, Your stone – magnesium ammonium phosphate is made by bacteria that can cleave urea to ammonia; usual candidates are proteus, klebsiella, pseudomonas, and enterobacter species in the urine and kidney. The calcium phosphate and calcium oxalate are from more common causes so you have two problems. The UTIs would be related to the stones, perhaps, as I just noted. Anemia may relate to infection, too. If you are near Cleveland, the Cleveland Clinic has a brilliant kidney stone surgeon: Manoj Monga. You are equally near Indianapolis, and Dr James Lingeman at IUPUI is equally as outstanding. I would go to one or the other and get things taken care of. By the way, I am not recommending the institutions but specifically these two physicians, so do not accept substitutes for them. Regards, Fred Coe
I have had my first surgery for kidney stones( several, most between 6-7mm). I had my stent taken out today. I am a petite 45 year old woman with diabetes. The breakdown of my stones were thus, 50% magnesium ammonia phosphate, 40% calcium phosphate, and 10% calcium oxalate dihydrate. The doctor assigned to me at the hospital is uncommunicative to say the least, and we are looking for a new urologist to get a urine analysis done. The only advice he gave me was to drink more water, which I already do(diabetic) and no pop(which I may have 1 can a month). I am concerned because medically I have had a lot of health problems in the past year and I am wondering if my kidneys and/ or thyroid is the underlying issue and is being overlooked. A few problems are: multiple UTIs(never had before), c-diff twice(again never had before) pneumonia, sciatica, anemia, low vitamin d, low iron, 2 blood transfusions (never had before) and the weirdest, I haven’t had a period for three years, and started again recently. There is more but these are the main ones I could remember. How do I pull all this information together to find a solution? Is it possible it could all be related, and if so, what type of doctor could look at all the information and see the underlying condition(s)? Right now, I am trying to find a urologist to have a urine analysis done ASAP, because I never want to experience this pain again. Sorry so windy, but I am getting desperate for medical communication until I find a new informative urologist that can ELI5. Thanks in advance, and if you have any recommendations for urologists in Columbus, Ohio, I would love to have them. Thanks again, Karen
Hi Karen, Your stone – magnesium ammonium phosphate is made by bacteria that can cleave urea to ammonia; usual candidates are proteus, klebsiella, pseudomonas, and enterobacter species in the urine and kidney. The calcium phosphate and calcium oxalate are from more common causes so you have two problems. The UTIs would be related to the stones, perhaps, as I just noted. Anemia may relate to infection, too. If you are near Cleveland, the Cleveland Clinic has a brilliant kidney stone surgeon: Manoj Monga. You are equally near Indianapolis, and Dr James Lingeman at IUPUI is equally as outstanding. I would go to one or the other and get things taken care of. By the way, I am not recommending the institutions but specifically these two physicians, so do not accept substitutes for them. Regards, Fred Coe
Over the years I have had kidney stones ranging from tiny to 9mm (which had to be removed last fall by surgery). The urologist said that I had two other fairly large stones (about 6mm) that could pass in the other kidney on their own or require surgery. The pain and thought of them left me until recently being 5 months pregnant. The side throbs have come back and I feel terrible for having forgot about them. I had kept one of the stones I passed at home a few years ago and am having a hard time identifying it. It’s extremely shiny/crystal like and a light beige color. I want to know what type it is so that I can somewhat be in control of my diet to prevent them from enlarging. I’m waiting for the urology office to get back to me but I am concerned with being pregnant what the protocol is for large stones? I’d imagine by now if the 6mm ones have not passed that they have increased in size and this has me worried for my unborn child.
Hi Christy, during pregnancy you should not try to figure out the cause of stones; wait until you have finished breast feeding. Stone analysis is crucial so get those stones analysed. Usually a stone attack during pregnancy is treated by stenting for small obstructing stones and leaving large stones alone until afterwards unless confronted by a serious obstruction, infection, pain attack, or serious bleeding. Diet change is not ideal while pregnant. IN other words, wait until alter then take serious efforts at prevention. Here is a good place to begin thinking about the approach. Regards, Fred Coe
Over the years I have had kidney stones ranging from tiny to 9mm (which had to be removed last fall by surgery). The urologist said that I had two other fairly large stones (about 6mm) that could pass in the other kidney on their own or require surgery. The pain and thought of them left me until recently being 5 months pregnant. The side throbs have come back and I feel terrible for having forgot about them. I had kept one of the stones I passed at home a few years ago and am having a hard time identifying it. It’s extremely shiny/crystal like and a light beige color. I want to know what type it is so that I can somewhat be in control of my diet to prevent them from enlarging. I’m waiting for the urology office to get back to me but I am concerned with being pregnant what the protocol is for large stones? I’d imagine by now if the 6mm ones have not passed that they have increased in size and this has me worried for my unborn child.
Hi Christy, during pregnancy you should not try to figure out the cause of stones; wait until you have finished breast feeding. Stone analysis is crucial so get those stones analysed. Usually a stone attack during pregnancy is treated by stenting for small obstructing stones and leaving large stones alone until afterwards unless confronted by a serious obstruction, infection, pain attack, or serious bleeding. Diet change is not ideal while pregnant. IN other words, wait until alter then take serious efforts at prevention. Here is a good place to begin thinking about the approach. Regards, Fred Coe
Dr. Coe,
What a fabulous web site. Thank you so much for taking the time to put this information together in such a readable form.
My question is about alcohol and caffeine.
I had not had any stones for almost 20 years.
Six months ago I stopped using both alcohol and caffeine completely.
Now I have had three separate bouts with COX/UA stones over the last month.
Could there be a relationship to my abstinence, or do you think coincidence at play?
Daniel
Hi Daniel, Possibly the loss of coffee mattered – coffee has a negative correlation with stones. Alcohol as well – same link. The uric acid component means your urine has become overly acidic, and coffee is an alkali. I would get 24 hour urine testing and find out what is causing your stones – I know the pH will be low, but what else? Regards, Fred Coe
Dr. Coe,
What a fabulous web site. Thank you so much for taking the time to put this information together in such a readable form.
My question is about alcohol and caffeine.
I had not had any stones for almost 20 years.
Six months ago I stopped using both alcohol and caffeine completely.
Now I have had three separate bouts with COX/UA stones over the last month.
Could there be a relationship to my abstinence, or do you think coincidence at play?
Daniel
I know you’re not a veterinarian, however, I have a dachshund that has had to have surgery to remove stones twice. She was 8 yrs old the first time and she’s 11 yrs old and just had them removed again. She only weighs 10.9 lbs. She’s had 4 stones each time and they are huge. They were almost an inch in diameter each. The analysis has been done, the results were Magnesium Ammonium Phosphate 70% and Calcium Phosphate 30% on both the interior and exterior. The Nidus is composed of 100% Magnesium Ammonium P04 6H20 (Struvite). I’m trying to figure out a diet for her and the vets are not nutritionist and really have no idea what to tell us. She eats a good brand of dog food, Dinovite (supplements/nutrients), Supromega Fish Oil and sometimes Coconut Oil in the am. Quinoa, homemade chicken broth and moringa powder in the pm. I could sure use some help. Anything you can tell me that would help or a link to where I can find a diet for her, I would really appreciate it. Thank you so much.
Hi Lori, Veterinary medicine is a deep specialty and I know nothing. If your present physicians cannot help you need to ask them for a referral. Animal stone disease is a deep and complex specialty, and I a fool to enter into it. Best, Fred
I know you’re not a veterinarian, however, I have a dachshund that has had to have surgery to remove stones twice. She was 8 yrs old the first time and she’s 11 yrs old and just had them removed again. She only weighs 10.9 lbs. She’s had 4 stones each time and they are huge. They were almost an inch in diameter each. The analysis has been done, the results were Magnesium Ammonium Phosphate 70% and Calcium Phosphate 30% on both the interior and exterior. The Nidus is composed of 100% Magnesium Ammonium P04 6H20 (Struvite). I’m trying to figure out a diet for her and the vets are not nutritionist and really have no idea what to tell us. She eats a good brand of dog food, Dinovite (supplements/nutrients), Supromega Fish Oil and sometimes Coconut Oil in the am. Quinoa, homemade chicken broth and moringa powder in the pm. I could sure use some help. Anything you can tell me that would help or a link to where I can find a diet for her, I would really appreciate it. Thank you so much.
Hi Lori, Veterinary medicine is a deep specialty and I know nothing. If your present physicians cannot help you need to ask them for a referral. Animal stone disease is a deep and complex specialty, and I a fool to enter into it. Best, Fred
Hello, Dr. Coe.
I have had kidney stones since I was in my mid thirties. I have recently been diagnosed with medullary sponge kidney, although notes mention the possibility back on 2009.
Until recently my stones seem to have been Utica Acid and could only be seen on u/s or CT’s. I’ve had numerous procedures to clean out stones. The last two procedures were 4 mo this apart with removal of over 120 stones (60 from the left and 40 from the right) in the first procedure. The second procedure yielded over 40 – the the doc stopped counting.
Now I am having stones begin to show up on X-ray as well.
I have never passed a stone. Mine are adhered to the micro ducts.
I suffer extraordinary pain on a daily basis… average daily pain runs at a 6-7, and spikes at 9-10 two to three times a month for several days at a time.
ER releases me with a sneer at “punctuate stones – too numerous to count” with no relief for the pain.
My last urine collection was a month ago. The first was completed on a Sunday, the second on a Monday. The results were all within normal range with the exception of mildly low citrate on the Sunday collection. On the past my 24 hour collections have also been in the normal range.
I saw Dr Moe at SW University of Texas in 2013. He agreed my urine collection at that time was perfectly normal and I did. Not look like a stone former from that standpoint. He had no explanation other than some people just have pain with stones in their kidneys. Plan to deal with it.
I now have two Urologists, one locally and one in Little Rock, AR at UAMS and a local Nephrologist. My Nephrologist is seeking an MSK specialist recognizing his own knowledge is too limited to help.
I cannot get a pain management clinic to assist with pain management due to the restrictions put on doctors with the new laws.
My biggest concern is pain management as I don’t pass stones but the constant pain is excruciating. The holmium laser procedures are being limited due to the increased risk of scarring from frequent procedures.
I am having increasing amounts of UTIs despite a daily low dose antibiotic to try to help prevent them. I just clear one up and another strikes. The pain with these infections is very intense.
My quality of life is deteriorating. I am trying to remain a productive citizen and mom to two kids, but the pain is ruling my life and limiting my ability to provide for my family. I do not want to be a victim.
I’m interested in how a normal weekend and weekday 24 hour urine collection play into all of this and what you recommend for pain management?
Warm regards and thank you for your consideration.
Hi Tammy, I doubt the many stones are uric acid,, and suspect they are calcium phosphate – perhaps brushite. Although numerous, my experience is that this kind of accelerated stone disease is rather easy to treat and often associated with normal 24 hour urine collection data. The amount of pain is unusual but may be in part for continued crystal formation. Dr Moe is an outstanding expert, by the way, so your problem must be unusually difficult to resolve. I doubt you have MSK; the physicians who did your ureteroscopy saw your renal papilla and should be able to say yes or no; I suspect it is not MSK but a more common form of tubule plugging. That is what they meant by adherent to micro tubules. I am willing to see you as a patient at U Chicago if your physicians believe I can be of some help. Regards, Fred Coe