
 Up to this point we have considered only increase of urine volume as a means of stone prevention. The effect of increased urine volume is to reduce urine supersaturation with respect to stone forming salts and therefore reduce the risk of crystal formation which is the basis for kidney stones.
Up to this point we have considered only increase of urine volume as a means of stone prevention. The effect of increased urine volume is to reduce urine supersaturation with respect to stone forming salts and therefore reduce the risk of crystal formation which is the basis for kidney stones.
WHY CITRATE
Mechanisms
Supersaturation with respect to the calcium stones depends upon urine concentrations of calcium, oxalate, phosphate, and citrate, and, in the case of calcium phosphate stones, or uric acid stones, urine pH. Giving citrate salts can reduce urine calcium excretion and increase urine citrate. Urine citrate binds urine calcium in a soluble citrate complex, which reduced calcium salt supersaturations. Citrate inhibits crystal formation, growth and aggregation. The alkaline citrate salts can raise urine pH.
 Epidemiology
Epidemiology
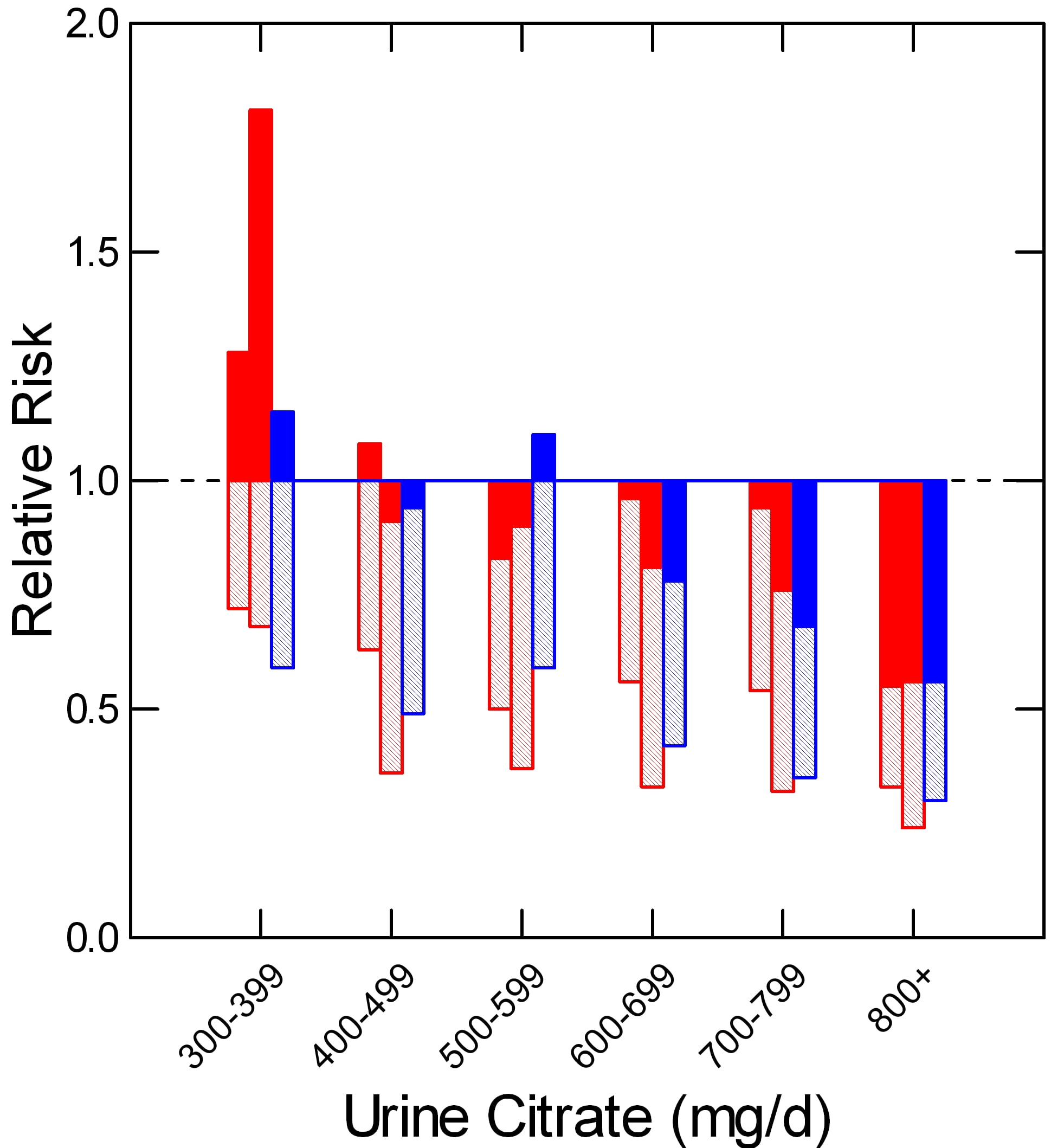
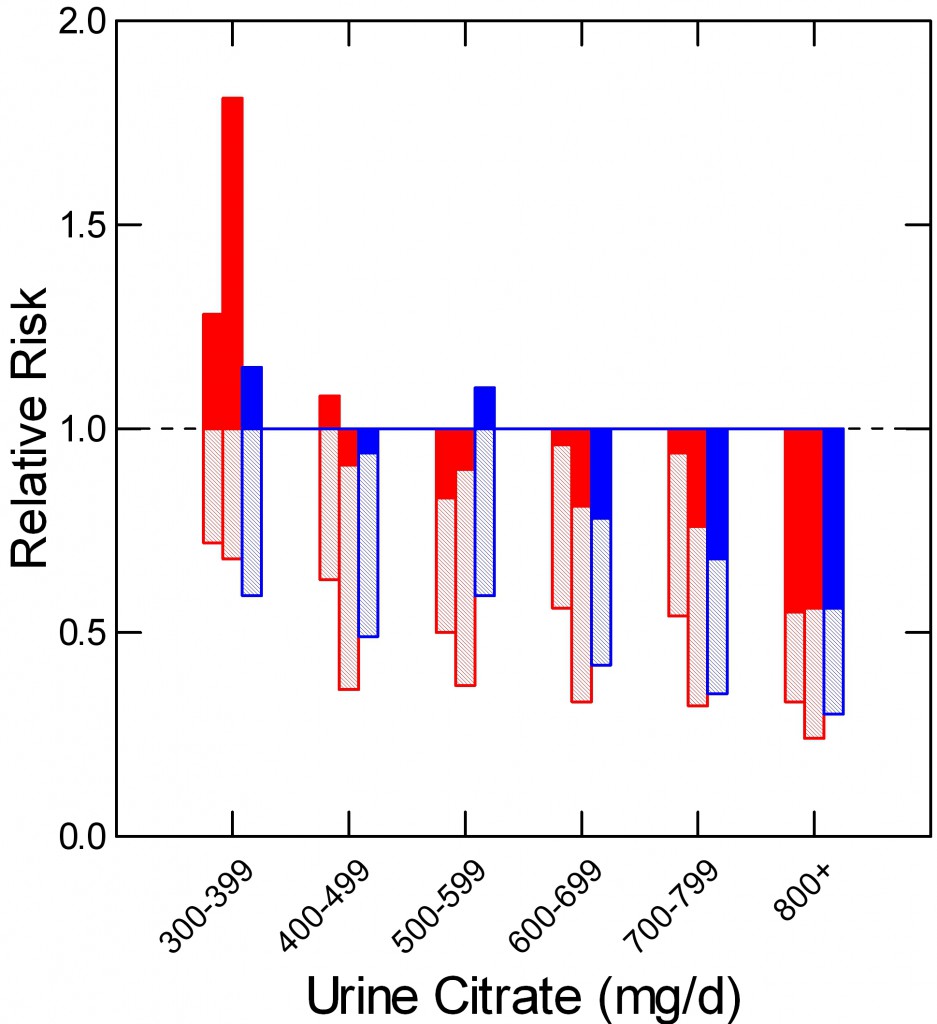
In a prospective study of two nurse (red) and one male physician cohort (blue) Curhan found that relative risk of kidney stone onset (vertical axis) rose as urine citrate excretion (shown in hexiles along the horizontal axis) fell. Below 400 mg/day of urine citrate risk was – compared to above 800 mg/day) increased by nearly 2 fold. Mean relative risk is at the ends of the shaded bars. The upper 95% of risk is at the tops of the filled bars. Even though the average risk (end of crosshatched bars) remained below 1.
CALCIUM STONES
TRIALS
Although I had quibbles with some of the comments it included, I believe the recent American College of Physicians (ACP) review of kidney stone prevention trials was done properly, and therefore have selected for review here those they felt were technically adequate.
Below is a detailed presentation of the five studies. Here is a link to my spreadsheet with all of the numbers. It also contains my references for thiazide treatment.
Ettinger et al (J Urol 158:2069-2073, 1997).
Sixty four patients with at least 2 stones in the past 5 years and at least 1 within the past year before the trial were given placebo (33 cases) or potassium magnesium citrate (63 mEq citrate, 42 mEq as potassium and 21 mEq as the magnesium salt in combination pills) – 31 cases. Each pill contained 21 mEq of citrate; 2 pills were taken 3 times a day. The trial was designed to last for 3 years. There were 5 and 9 women in the placebo and treatment arms. Urine citrate excretions were not different before treatment (549 and 587 mg/day, respectively, nor were urine volume, pH, calcium, oxalate, or any other stone forming risk. After a one month grace period in which new stones were not counted, any passage or radiographic appearance of new stones, or growth of previous stones was considered a treatment failure. During the trial, 15 subjects left the treatment arm, 8 the placebo arm.
New stones or growth of old stones occurred in 63.6% (16 cases) of the 25 placebo cases who finished the trial and in 12.9% (2 cases) of the 16 treated cases who finished the trial. If the 6 subjects who left the treatment arm because of drug adverse effects are added in as treatment failures the drug effect remained significant (8 of 22 or 33%).
Of note, this particular formulation is not available in the US. A version of the supplement is available OTC but the dose per pill is so low that it is impractical for anyone to use it. So the trial is part of a proof of principle, but not actually applicable to clinical practice in this country.
Lojanapiwat et al (International Braz J Urol 37:611-616, 2011)
Unlike the Ettinger study, which concerned spontaneous stone formation, this study concerned new stones or growth of residual fragments after shock wave lithotripsy (SWL) or percutaneous nephrolithotomy (PERC). Their subjects were 80 initial patients, all 8 weeks after either procedure, and either stone free or having no residual stone fragments >4mm diameter (Numbers are in the Table). Hypocitraturia (<325 mg/day) was present in 20/39 who received citrate and 15/37 who did not.
| SWL | PERC | Total | |
| STONE FREE | 24(8) | 15(5) | 39(13) |
| RESIDUAL STONES | 26(17) | 11(9) | 37(26) |
| Total | 50(25) | 26(14) | 76(39) |
They were randomized into 39 treated and 37 placebo treated groups and followed for one year which 76 of the original 80 completed. Numbers receiving citrate in each group are in parentheses. Sodium potassium citrate was given as 81 mEq/day in 3 divided doses).
Of the 13 cases who were stone free and received citrate, 12 remained so vs. 15 of the 26 given placebo. Of the 26 who had retained fragments and were given citrate, 8 were stone free vs. 1 of the 11 controls and 16 others given citrate showed no change (13) or reduction in size (3) vs. 2, no change and 2 decreased size among the 11 placebo. These differences were judged significant at the p<0.05 level by the authors.
Soygur et al (J Endourology 16:149, 2002)
This trial considered 90 patients after SWL for lower pole stones who had residual stones <5 mm or were stone free. They were randomly assigned to potassium citrate (50 mEq/day in 3 divided doses) or placebo (Table). The trial lasted one year. The end
| Citrate | Placebo | Total | |
| STONE FREE | 28(0) | 28(8) | 56(8) |
| RESIDUAL STONES | 18(0) | 16(6) | 34(6) |
| Total | 46(0) | 44(14) | 90(14) |
points were stone free or not and residual stone size increased or not.
New stones occurred (parentheses) in none of the citrate treated stone free patients and in 8 of the placebo treated patients. Among the residual stone group, the fragments disappeared in 8 treated cases and failed to grow or shrank in the others vs. growth or new stones in 6/16 placebo cases. The differences in growth or new appearance were all significant.
Of course, both of these post treatment trials are subject to the biases of a radiography study, but observers appeared to have been suitably blinded to the patient groups.
Hofbauer et al (British J Urol 73:362-365, 1994)
In this trial, an equimolal sodium / potassium citrate was given in doses that maintained urine pH in the range of 7 to 7.2 vs. placebo. Therefore, although patients were allocated randomly to active treatment or placebo, the trial could not be blinded. By the three year endpoint, 22/25 placebo and 16/25 active drug subjects remained. New stones occurred in 16/22 placebo and 10/16 active drug subjects. This difference was not significant. This study is the only one with a negative outcome. It is also the only study that was not double blinded.
Barcello et al (J Urol 150:1761, 1993)
Stone formers with urine citrate excretion rates below 643 mg/day (3.4 mmol/day) were allocated to potassium citrate 60 mEq/day in 3 divided doses. Their mean urine citrate excretion was 359 mg/day. At the end of three years of followup, 20/28 placebo treated and 18/27 citrate treated subjects remained. New stones occurred in 14/20 placebo and 5/18 treated cases, a significant departure from chance.
GRAND SUMMARY
| NEW STONES | |||
| YES | NO | TOTAL | |
| TREATED | 20 | 115 | 135 |
| NOT TREATED | 77 | 71 | 148 |
| TOTAL | 97 | 186 | 283 |
Despite the variability of design, one can, with nerve, simply ask about the beneficial effects of citrate salts across all the trials. In all five trials 283 people completed the desired treatment period. Of these, 97/283 (34%) formed new stones or, in the case of the post procedure trials showed growth of retained fragments. Among all patients who were given citrate salts, 20/135 (14.8%) formed new stones or showed growth of retained fragments vs. 77/148 (52%) of those given placebo.
I have not added back the 6 cases from the Ettinger trial who left because of drug side effects.
From this we can reconstruct a sense of the value of the treatment as applied to the mixed practice of post surgical management and overall medical prevention.
Let us assume these numbers will hold for the future.
For every 1000 cases like the ones in the trials, 520 untreated cases will form new stones or show stone growth after a procedure vs. 148 cases/1000 cases with citrate, a savings of 372/1000 cases overall.
I realize I am not calculating in the most satisfactory manner as a statistician, but I rather like the coarse grained, even vulgar nature of my count me up.
QUALITY OF EVIDENCE
A Personal View
The trial community exhibits the kind of methodological fussiness one expects and applauds in any scientific situation. Among their ilk the citrate effect is viewed as modest at best, the evidence, by their likes, fair.
I am sure they are right according to the mores and social instincts of this discipline, but I do not come from nor inhabit that discipline, and therefore have an altogether different way of counting – for that is all one does after the impatient and often indifferent subjects have played out their roles in the work.
How likely is it, I ask myself, that citrate salts do not prevent new stones or fragment growth?
Not at all likely.
Why assume anything but that blinding was performed when specified, that radiograph readers were competent and blinded to the groups patients were in, that stone events were counted fairly and compared to radiographs to estimate new stones? If we make these assumption of honesty and skill, the marked downward skew from alkali is just too large to be by chance.
My bet will be on the drug, and if I bet that way, I will always win.
Do We Need More Trials For Calcium Stone Formers?
For me, no. It would seem a waste of money.
Some trials treated patients with reduced urine citrate, others did not. Some trials looked at new stones over 3 years, others at residual fragment growth one year after urological procedures. Will another 50 or even 100 cases be likely to change the outcomes? If so, in what way, and why?
It is true that one trial showed no effect and that trial was not blinded. It is actually a drag on the results as I did not remove it.
We Do Need a Trial of Citrate for Calcium Phosphate Stone Formers?
I do not know how often this must be said. Calcium phosphate stone formers must lurk in each of the trials I have reviewed, but I do not know their outcomes. One trial insisted stones be at least >50% calcium oxalate. That means perhaps a few had considerable phosphate is stones.
Calcium phosphate crystal formation is sensitive to urine pH whereas calcium oxalate stone formation will not be. The reason is that calcium phosphate supersaturation requires divalent phosphate be present, and the pKa for the second proton is about 6.8. Citrate salts can raise urine pH, so they can raise supersaturation with respect to calcium phosphate salts. On the other hand, citrate is an inhibitor of crystallization both because it is calcium binding and because it directly affects calcium crystal growth.
ROLE OF TESTING
The very same ACP report from which I derived the studies shown here presented an annoying set of comments that infers we might as well just give a drug like potassium citrate without knowing stone composition, or doing serum or urine testing that concerns stone pathogenesis.
For this reason, I offer some remarks on that subject. This is in the special context of citrate treatment. I have made more general remarks of a negative sort about the APC comments.
Does Stone Analysis Matter?
How can it not? I have already mentioned the problem of phosphate stones. Do we not have to exclude struvite is stones? The odd patient with cystinuria who has slipped by? Drug stones? Conversion from calcium oxalate to calcium phosphate stones?
Do Serum and Urine Testing Matter?
How can they not?
SERUM
Do we want to give potassium loads to people with reduced renal function?
Having prescribed potassium, do we not want to monitor for serious increase in serum potassium; some patients are older, some diabetic, some take ACE or ARB medications, some age or change drugs over the years we treat them.
Do we not want to diagnose primary hyperparathyroidism? You cannot without serum testing and 24 hour urine testing to be sure calcium excretion is not low.
24 HOUR URINE TESTING
If we do not obtain and measure 24 hour urine samples, how can we know anything? Some patients may have very high urine citrate levels. Some may have very high urine pH values.
Here and there urine oxalate is very high, from primary hyperoxaluria, or occult malabsorption syndromes, or very odd food habits.
People change their habits and develop diseases.
Moreover, people do not always take their citrate. Fall in urine ammonia in relation to urine sulfate, and rise in urine potassium assure one they are taking the drug.
URIC ACID STONES
Do We Need a Trial for Uric Acid Stone Formers?
NO
No one really questions that alkali salts will raise urine pH, nor that raising urine pH will reduce uric acid supersaturation and prevent stones. It is common practice. I doubt anyone will pay for or perform an RCT to test this question.
That they will not is very important, because it raises an unexpected question.
WHY NOT?
We Know the Chemistry
Uric acid is a large flat mainly hydrophobic molecule with most of its charge on a single proton receptor site. The protonated from has a very low solubility in urine of around 90 mg/liter whereas 24 hour urine uric acid excretion ranges from 400 to over 1000 mg daily depending upon diet purine loads. The pKa of the proton receptor site is about 5.3 in urine.
Given these facts we can calculate uric acid supersaturation from the urine concentration of total uric acid and the pH, along with minor adjustments for the effects of ionic strength on the pKa. High supersaturation will lead to a snowstorm of uric acid crystals. Raising urine pH to above 6 will generally reduce supersaturation below 1 and end uric acid stone formation.
Everyone Knows Alkali Work
There is a lot of uric acid excreted every day, so uric acid stones can grow rapidly. Uric acid gravel has an orange red color and is often seen. When alkali are given, the gravel goes away only to come back if patients miss doses. The absence of new stones is obvious.
No One Treats Without Stone Analyses
Who can be sure of stone composition without stone analysis? Even during treatment of someone who has produced uric acid stones, calcium oxalate or calcium phosphate stones may begin. So people know the stone type, and proceed by custom.
No One Treats Without Testing Serum and Urine
Uric acid stones are common in diabetics and people with reduced renal function; potassium loads are potentially dangerous. Perhaps this is more obvious among uric acid stone formers than calcium stone formers, although given wide spread use of ACE and ARB drugs and NSAIDS, potential risk is everywhere.
The amounts of alkali needed can be variable, and the only reliable way to ascertain is 24 hour urine testing. Likewise for compliance.
Therefore routine practice monitors before and during potassium citrate treatment of uric acid stones.
TRIALS ARE UNNECESSARY
IN this situation, no one has and probably no one will propose a trial of alkali for uric acid stones. But, there is an almost exact parallel situation for calcium phosphate stones, yet such certainty as pertains to uric acid stones certainly does not exist.
CALCIUM PHOSPHATE (CaP) STONES
Do We Need a Trial for CaP Stone Formers?
YES
WHY?
We Know the Chemistry
Calcium cannot combine with mono-valent phosphate but only with the divalent form. The pKa for dissociation of the second proton of phosphoric acid is about 6.8 in urine, although the precise value varies with ionic strength. Given the molarities of total phosphate, calcium, citrate – which binds calcium – and other ligands that have modest effects, the supersaturation of brushite – the usual initial urine CaP phase – can be calculated as well as we can calculate the supersaturation for uric acid.
Like uric acid, phosphate and calcium are abundant in urine, so the amount of crystal that can be produced in a day is similar to that of uric acid. Therefore stones can, and do, form rapidly and become large.
As in the case of uric acid, high urine CaP supersaturation can produce snows storms of crystallization; though certainly not common, patients can recognize this as white urine.
On physical chemical grounds, to lower CaP supersaturation below one and keep it there is to prevent CaP stones as surely as one prevents uric acid stones by raising urine pH and lowering supersaturation below one. Why, then, is not this treatment as self evident as alkali for uric acid stones?
Everyone Does Not ‘Know’ Treatment Works
We have no drug corresponding to alkali.
We can raise urine pH safely but cannot lower it.
Acid loads raise urine calcium losses and can be detrimental to bone mineral balance. Higher protein intake is a possible way to lower pH, but not all kidneys respond to acid with a prompt fall in pH. In some cases urine ammonium ion excretion will rise. In others, acid retention may occur. Urine calcium will tend to rise.
So treatment is not as transparent as for uric acid.
But Treatment Must Work Exactly the Same Way
We can lower CaP below 1 with fluids and measures – reduced diet sodium and thiazide – that reduce urine calcium, and we can monitor supersaturation as we monitor urine pH and uric acid supersaturation.
Furthermore, patients can tell if white urine has ceased.
Moreover, because stones are often actively forming, effective treatment is reasonably obvious.
However, these measures may be difficult to achieve. Thiazide is not always tolerated, reduced salt diet not always maintained.
Citrate is a powerful inhibitor of crystals, and it would be good to know if it were beneficial for the CaP stone former.
It seems that citrate will reduce stone formation / growth. It has been suggested elsewhere on your site that lemonade might be an easy inexpensive way to get citrate and at the same time – increase fluids. Lemonade without sugar (which increases calciuria) is even better. some of the trials you summarize divided up the citrate supplements to TID. Do you think that is an important feature to stress to patients? I have also read on your site that most stones form at night (presumably aided by decreased fluid intake when you are asleep). Would you theorize that having a sugar free lemonade before going to sleep would be of particular benefit compared to other times of the day?
Hi Randy, I think whatever the form it is better to spread the alkali out. Lemonade is not as efficient as Crystal light – the latter has more citrate. The US guidelines say that 5 servings of fruits and veggies a day will provide 4,500 mg of potassium with works out to about 40 mEq of potassium anion, so perhaps we should just give up on the juices and just have everyone eat right. As for night time, urine calcium stays up in people with hypercalciuria, and thiazide does not lower it enough. Fruit at bedtime might be ideal. I really should refine all this in the articles themselves, but there are so many details! Best, Fred
Thanks, Dr Coe. Your site has grown so big I don’t know how you can manage it all? Time to train a grad student to make these edits!
Hi Randy, It is big enough I will eventually need some part time help keeping links clean. But I like the questions, and answering them. Best, Fred
We have a pet pig who has a calcium carbonate urolith. We believe it to be dietary related. I would like to put him on some sort of preventative moving forward. Would potassium citrate work as well for preventing calcium carbonate stones?
I’m sorry, Jen, veterinary medicine is outside my professional scope. I would be guilty of malpractice. There are experts, and you should ask one. Regards, Fred Coe
I have had a single 11 mm uric acid 80%,calcium oxalate 20% stone. My urine citrate was 550,urine ph 5. I was not a big water drinker and was on high protein diet. My urologist has not recommended anything except to drink enough water to produce 2.5 l of urine a day. On my 24 hr urine I produced 2200 mls. Does drinking alkalinized water (ph 9.5) help? And what else should I do ?
Hi Randy, Given an 80% uric acid stone and urine pH of 5.1 you should be on proper dosing of a reliable alkali such as potassium citrate 20 mEq twice daily. Beverages and the like are one thing, but uric acid in stones is totally preventable with sufficient alkali and will recur with less than that. Please review this with your physician. To me, a recurrent uric acid stone is a preventable and unfortunate event. Regards, Fred Coe
Thank you very much. I now have a Ct proven second stone 6 mm. I am calling urologist stat to get placed on Potassium citrate. Is there a chance this will dissolve the current stone?
Hi Randy, I do not know because stones dissolve from outside in and the process can be slow. But be sure the dose of potassium citrate produces a 24 hour urine pH of at least 6, which may take 40 – 60 mEq of the medication. Also, you have some calcium oxalate in stones and that may continue to form. So get a proper evaluation. Here is a plan for you. Regards, Fred Coe
Hello Doctor,I am on potassium citrate now ,just trying to get used to it. Started with 10 meq daily after 4 days Im nauseaos from this. Also added Real lemon juice 2 tbsp. a day in water..by day 3 I did a urine ph and it finally went from 5 up to 8,but not for long. The next day I could not take the pill.Also they are large pills,I looked at the 15 meq pill and said no way can I swallow these.
I am having enough trouble with the ten..
Any tips for reducing Gi side effects?
Hi Randy, One pill cannot suffice and you cannot stand taking them anyway. I would suggest a liquid form of potassium citrate. Also, Crystal light contains 20 mEq of potassium citrate in a liter of the lemonade, which is equivalent to 2 pills. Regards, Fred Coe
Hi Dr Coe,thank you for you reply. I have just sent for potassium citrate pure crystalized powder as recommended by my urologist .I hope I can tolerate this when I drink it in liquid form.I will keep you posted. Thanks again I really appreciate this website .
Dear Dr,
From the studies it appears that Potassium Citrate will reduce the chance of forming and will shrink existing stones. With myself definitely scared of surgery (Percutaneous Nephrolithotomy) is there any data that would show how long the process takes to shrink larger stones ( 4 centimeters)? Currently taking Potassium Citrate 10 mEq and Allopurinol 100 mg for a 4 centimeter stone in my left kidney. I’m sure increasing the pH to 5.5+ will slowly breakdown the stone depending on composition but at what rate. Appreciate any feedback. Thank you
Hi Chris, If you mean uric acid stones, potassium citrate will raise urine pH and the higher pH can in principle dissolve the uric acid crystals. But 4 cm is very large and it could take a very long time. The allopurinol is without value if for the stone and I would discuss stopping it with your physician. The pH you need is above 6 on the 24 hour urine – average pH for the day. Such big stones often are multiple smaller ones glued together so as things come apart you may begin passing lots of smaller stones. The big problem is the ratio of surface to volume which is 1/radius. Small stones are all surface big ones all volume so it is like licking a large lollypop – slow. If the stone is not obstructing and your surgeon feels you can wait safely, so it; but it is the surgeon’s judgment. Best, Fred Coe
What does it mean when all of oxalate, calcium and uric acid is way too high in the urine? What does it mean when calcium does not stay inside of your body? Like when she uses the restroom, she urinates the calcium? What is this and how can it be fixed?
Hi Kelsey, When everything is high the urine may be over collected – one can tell from the urine creatinine. If everything is high diet is not ideal. When urine calcium is high and it is real – not from over collection – it is usually a genetic trait. The high calcium can cause kidney stones and also bone mineral can be lost. Here is an article about the trait. It can be treated with diet. Regards, Fred Coe
I had urinary stone, uric acid dehydrate 90%, ammonium acid urate 10%, 1.3mm, 1/16 inches, in size, causing some scratches in urethra. check by urologist on 7-10-12, since then till now 5-8-17, I am drinking more water when the urine is concentrated. some days I may see some tiny stones. KUB x-ray and sonogram 11-23-15 show no stone identified. any chance I may be in a surgical case? thanks,
Hi Tim, Uric acid stones arise from too acid a urine pH; potassium alkali raise pH and prevent more. The tiny stones you see are probably uric acid. Water is a poor treatment because in an acid urine the volume needed to prevent crystals may be very large. Speak with your physicians about potassium citrate 10 mEq tablets, 2 twice a day. Regards, Fred Coe
Hi Dr Coe. I just received crystalized pure Potassium citrate powder .I am trying to calculate how many teaspoons or fractions of to take to equal 20 meq ofPotassium citrate. By my research there is 9.8 meq per 1000mg. My order has 250 g of potassium citrate =8.82 oz.,By my estimate I figure I need 2000mg to approx =20 meq,However I don’t know how this calculates to fraction of teaspoon? Can you help me?
Hi Randy, According to Wikipedia crystalline potassium citrate has a density of 1.98 gm/cm^3 Water density is, of course, about 1. You do indeed need about 2 gm to get 20 mEq. A teaspoon holds 4.92 ml (cm^3) of water, or just under 5 gms. Given its density your material is twice as heavy for the same volume. 10 mEq is actually 1080 mg, 20 therefore 2160 mg. So you need 1.1 cm^3 – about 1/5 of a teaspoon. The problem is packing, I have never looked at the stuff; for my arithmetic it would have to pack like flour not be chunky. Perhaps a better way is to buy a food scale that can weigh one gm to the nearest 0.1 gm. Regards, Fred Coe
Hello Dr. Coe,
My mother was recently informed she has osteoporosis. Due to the information that I’ve read about calcium using up phosphate in the body. I informed her that she should calcium phosphate . Now I’m reading about calcium phosphate stones.
Would adding magnesium citrate help alleviate the possibility of stones?
Or would switching to calcium citrate be a better option to avoid stones.
Thanks so much for your help and time!
Nate
Hi Nate, Osteoporosis in someone without kidney stones has its own treatment world. A high diet calcium intake from foods 1,000 to 1,200 mg is always worthwhile as is adequate serum vitamin D levels. From there, it is decisions about medications, and this goes far beyond what this site is about. High calcium diet from foods is not known to promote stones – calcium supplements can do this. Regards, Fred Coe
hi doctor,
I wanted to know if you could please recommend potassium citrate pills for multiple- frequent stones with urine citric acid (24 hours) level of 0.59 mmol/24Hrs, as I am a kidney stone patient for almost 20 years .
I am not drinking plenty of water due to my meditation now a days.
kindly tell me for how long I have to take the pill 10mg or 20 mg BID or TDS and what are its side effects if taken for long time.
your kind reply is awaited…
irfan
Hi Irfan, The better approach is to find out why you make stones and get selective treatment. I wrote this guide book exactly for you, take a look. Regards, Fred Coe
thanks but the guide book didnt help me about hypocitraturia. what is its cause and treatment…?
regards
irfan
Hi Irfan, This article tells about citrate and how the pills work. The treatment evidence for citrate is here. Regards, Fred Coe
Hi Dr. Coe,
I’m a 29 year old female and I’ve been suffering with kidney stones for 3 years. I’ve had then removed twice, but they keep returning in both kidneys. I recently did a 24 hour urine test which revealed that I have “abnormal” amounts of calcium in my urine. In addition to this, my urologist stated the rest revealed high amounts of oxalates and high amounts of uric acid in my urine. My doctor also told me I was producing 1.7ml of urine when it should be 2.8. I am SO very frustrated with trying to figure out how to not be dealing with this forever. Also, I feel cutting animal proteins from my diet and cutting oxalates leaves me with virtually nothing to eat. This is so hard! (I do not drink soda at all except for the occasional ginger ale dor upset stomach or juice). I have been upping my water intake and adding lemons to the water, but what more can I be doing and what do you suggest for consumption that helps with both uric acid and high oxalates? My doctor also prescribed hydrochlorothiazid for me now. Im weary of starting medicine if I can address it with diet. Any help you can provide would be immensely helpful!
Hi Whitney, You did not mention the kind of stones, but seem to have idiopathic hypercalciuria. I imagine that is your main problem. Here is a source for your treatment. The entire stone guide book is also for you as it says what to do and gives links to the more complex articles. Regards, Fred Coe
Hi,
recently I have got kidney stones and I could arrange the stone analysis. the analysis for the stone indicated it as CALCIUM CARBONATE stone of 2mmx2mm size. one stone of 5mm is still present in my right kidney. What are the dietary controls I have to take and what medicines to dissolve this undelivered stone.
thanks
sandeep
Hi Sandeep, Your kind of stone usually arises from an unduly alkaline urine and high urine calcium. But treatment without evaluation is futile. Here is a good plan. This is about the failure of random treatment.
I have had bouts of uric acid stones in the past and my dr. has prescribed one Potassium Bicarbonate effervescent tablet (25mEq) twice a day. I haven’t had any kidney stones since I began taking it 3 years ago, have had a hard time getting my two doses in each day. Would Crystal Light work the same/as well? And how would I know? Measure the pH of my urine myself?
Hi Sarah, Yes, alkali; Crystal light has 20 mEq of alkali in each liter so it should substitute. 24 hour testing is the prefered way to be sure. Here is my new article on uric acid stones – more complete than I had before. Regards, Fred Coe
HELLO SIR, MY NAME IS JAKSHAY. I WANT TO TELL YOU HELATH QUES.ABOUT MY 3 MONTH SON VIHAAN.A FEW DAY AGO,BLOOD COME IN URINE OF SON.SO,I WAS GONE TO OUR PED.DOCTOR.DOC.SAID FOR USG & URINE RM REPORT.SO,WE DONE BOTH.IN USG REPORT MULTIPULE (3 TO 4 IN EACH KIDNEY) STONE OBSERVED IN BOTH KIDNEY WITH LARGEST SIZE IS 4MM & IN URINE RM REPORT RBC NOTICED 35 TO 40/HPF, CRYSTALS OF CALCUIM OXLATE NOTICED.SO,OUR PED.DOCTOR SUGGEST US TO CONSULT A PED. NEPHROLOGIST FOR OPNION FOR SUCH FORMATION OF STONE.SO,WE CONSULT A PED. NEPHROLOGIST IN OUR CITY, SHE DONE 24 HRS URINE REPORT OF MY CHILD.AFTER REPORT COME SHE SAID THAT YOUR BABY HAVE HYPERCALCURIA & REASON FOR HYPERCALCURIA IS EXCESS DOSE OF VITAMIN D3 & CALCUIM SYRUP.SO,PRESENT SHE GIVE US k-CIT SYRUP(3 TIMES IN DAY) FOR ONE MONTH AS A TREATMENT & ASKING TO F’UP AFTER ONE MONTH WITH USG & URINE RM REPORT.SO,SIR I WANT TO KNOW THAT WHAT IS THE REASON OF HYPERCALCURIA OCCURED IN BABY EVEN WE ALWAYS GIVE THE DOSE OF VITAMIN D3 & CALCUIM SYRUP AS SUGGESTED BY OUR PED.DOCTOR & ALSO WANT TO, KNOW THAT WHAT IS CHANCES OF NORMALIZE OF THIS HYPERCALCURIA WITH ABOVE TREATMENT.IT IS DENGERS DISEASE OR NOT?
Hi Jakshay, Of course this is a very serious problem. Hypercalciuria can occur in infants. I doubt vitamin D is the reason, and would suspect idiopathic hypercalciuria or another genetic cause. Also be wary about urine oxalate, as primary hyperoxaluria can be present. This is so complex and I am so far away I can only urge your peds nephrologist be very careful about diagnosis and consider genetic testing as well as urine testing. There are a lot of stones! I would be remiss in saying more. Regards, Fred Coe
Dear Dr Coe,
I require acetazolamide for treatment for a neurological problem. After 1 year at 500mg per day I passed a kidney stone. CT showed one small remaining stone in the other kidney. A 24hr urine test revealed very low citrate of 39 mg/day. Most everything else was in the green zone except for low urine volume, and somewhat elevated calcium oxalate, brushite and sodium urate. My urologist put me on potassium citrate 15MEQ 3xday plus >2.5l of water per day. After 3 months, another 24 hour urine test was done. It showed citrate raised to 122 mg/day but oxalate urine went from 35 to 75mg/day, uric acid urine went from 732 to 956 mg/day, PH urine went from 6 to 7.4. My Dr was concerned that these numbers didn’t seem accurate so he said wait a year, have another test and lets wee what happens. 9 months later I pass another stone (literally one year to the day from the original stone passing). CT showed 4 stones remaining in left kidney (2 medium sized, 2 small) and 2 small in the right. I recently had another 24 hour test and I am awaiting the results. It seems that the citrate treatment has accelerated the stone formation instead of reducing it. I fear these are CaP stones that are forming due to the high urine PH. My question is, if we take as a given that I can’t stop taking acetazolamide (I really can’t function without it), what would be the best way to manage this situation? Should I take more Potassium Citrate to raise urine citrate higher, or will that make things even worse for forming CaP stones? I searched hard for literature describing how to manage stones for patients on acetazolamide but I could not find anything useful. If you have any references for this it would be greatly appreciated.
Best regards, Paul
Hi Paul, You pose quite a problem. Of course, the drug causes perpetual delivery of alkali downstream into the terminal nephrons, so pH is high and SS calcium phosphate likewise. As serum potassium falls – as usual- or even not, and serum bicarbonate falls, urine citrate falls and will remain low. Potassium citrate cannot help because the extra bicarbonate from metabolism of citrate simply moves into the urine raising pH and worsening CaP SS. The rise in oxalate does not seem germane, the rise of pH is expected. I would not pursue more alkali. Very low sodium intake might reduce distal bicarbonate delivery and potassium chloride would repair the potassium deficiency that almost always occurs with the drug. Of course, your neurologist might be asked for a more imaginative alternative – surely by now a new drug has come along. Regards, Fred Coe
Dear Dr. Coe,
I will definitely investigate alternative treatment, although it appears that in Neurology, there is not a good understanding of why certain drugs work, which makes finding alternatives difficult, particularly if the consequences of the drug not working are severe.
Prior to taking taking Potassium Citrate my urine PH was 6.0, is this considered high?
You note that you would not pursue more alkali, but do I understand correctly that you would eliminate the current level of potassium citrate supplementation?
There is a slow release version of acetazolamide that I am not taking. Would you expect any reduction in stone formation by using the slow release version? i.e. is it only the average PH that really matters, or is it better to avoid high swings from larger punctuated medication doses?
How helpful is increased fluid intake in this situation? In the first year of treatment, which produced only two quite small stones, I had very low urine volume (~1.3l/24hr) and did not control Sodium intake particularly well. It seems that at a minimum I could make an impact on stone formation relative to that first year by maintaining the high urine volume i have now and reducing sodium. Does this make sense?
Thanks so much for your help.
Regards, Paul
Hi Paul, Higher volume could help, and perhaps low sodium diet but that would require multiple 24 hour urines to monitor. Potassium citrate will not help well because it adds more bicarbonate. Potassium chloride might be helpful in case the drug has caused potassium depletion. Slow release etc might help, but I have no experience with it. So we are left with lots of water and low sodium. About this, with the drug blood sodium could fall, so have your physicians informed so they can monitor it. The best would be another drug. Regards, Fred Coe
I have read several articles, summarizing studies that indicate calcium supplementation increases stone formation, while increased dietary calcium reduces stone formation. My perception is that there is a missing piece in all these articles: None of them indicate whether the calcium supplement used in the study was carbonate, citrate, or something else.
After reading the article above, which explains that citrate is very good at blocking crystal formation, I wonder whether there is an appreciable difference between supplementing with calcium citrate versus calcium carbonate. Is it possible that calcium citrate could be beneficial as both a citrate source and a calcium source, reducing stone formation? Or is some other, overriding effect involved that causes an increase in stone formation even when a calcium citrate supplement is used?
Thanks in advance for any wisdom you may be able to bestow!
Hi Roger, A perceptive reader! Calcium with meals that contain oxalate blocks oxalate uptake. So food calcium – that tends to be with meals – is effectively reducing urine oxalate. Supplements often miss meals – taken in the morning or at random, so oxalate is not blocked. Calcium supplements tend to rapid absorption vs with meals, too, making spikes. We need a trial perhaps, of supplements with or between meals, but alas I know of none. As for citrate, the citrate creates bicarbonate and that can raise urine citrate, citrate is a good anti stone material. So perhaps it is a better supplement, although most calcium supplements have alkali so I am not so sure. Regards, Fred Coe
Many thanks for your reply.
It makes sense to me that if a calcium supplement is not taken with meals it won’t be effective. If no advice is being given to supplement with meals, then it sounds like that may be the real reason that calcium supplements perform poorly – rather than that there is something superior about food calcium sources.
Hi ROger, to me that is an astute analysis. Regards, Fred
Hi Dr. Coe,
I was a recent participant in one of Jill’s courses. You might recall my “impressive” (not in a good way) sodium number from my first Litholink tests: 327. Thought you would like to know that on my follow up test my sodium came back at 77 🙂 They tested twice to be sure there wasn’t a mistake at the lab 😀 Unfortunately, on my follow up results my citrate has gone from around 400 down to 292 and my pH is down to 5.322. I’ve read about the pills that could help my citrate number – potassium citrate. My question: Is there a direct correlation between the potassium that we eat and the citrate number on the test? I continue to work with Jill and I know the next part of my journey is to get more fruits and vegetables in more regularly. If I can do this, will it have a direct effect on my citrate number?
Hi Adrienne, I do remember and you did very well. More fruits and veggies sounds good to me. See how far they can take you and then make up the rest with some supplements. But do it in that order. Best, Fred Coe
I had a kidney stone removed on March 23, 2017. It was 10% calcium oxalate and 90% uric acid. Two weeks ago I has a urinalysis as part of a yearly checkup at my FP’s office. My urine PH was 5.5. Six months ago it was 6.0.
I have been taking Losartan Potassium (50mg) for high blood pressure since June 3, 2015. I recently read and article https://www.ncbi.nlm.nih.gov/pubmed/9010643 that stated “Losartan potassium increases uric acid secretion and lowers plasma uric acid levels, which may be of benefit when losartan potassium is combined with a thiazide diuretic, but which may otherwise lead to uric acid stone formation and possibly to nephropathy.”
Would you please comment on whether this drug could be responsible for my kidney stones? Thank you.
Hi Mark, No Losartan does not ever cause uric acid stones. The review article writer lacks knowledge. ON first use losartan can cause a brief outpouring of uric acid, but bicarbonate comes out with it, so uric acid cannot form. In fact I did the work showing this. Given you form 90% uric acid stones I doubt your 24 hour urine pH was 6; spot urines are not reliable. Be sure and get several 24 hour urines to be sure of your pH and other risk factors. You can read it yourself. Here is my main uric acid article. Alkali is for you. Enough to raise urine pH above 6 in the 24 hour urine. Regards, Fred Coe
I am a chronic suffer of kidney stones. I have been taking potassium citrate for years and have had success with minimal kidney stone growth and when I do pass them they are much smaller. But my potassium levels have been going up. What citrate alternatives are there that don’t contain potassium?
Hi Cindy, I wonder why your potassium is rising. Usual causes are drugs – ACE ARB etc. Others are diabetes or kidney disease. If these are causes, one can maintain urine citrate with fruits and veggies – five servings daily will provide about 4500 mg of potassium. Another question; if serum potassium is rising what is the urine potassium? Regards, Fred Coe
Hi Dr. Coe,
I have been suffering from kidney stones for 10 years, I am 25. My last 24 hour urine came back with 2.36 volume, 421 calcium, SS Cap 3.89, urine pH 6.753, and Urine Uric Acid being at 0.924. I make calcium oxalate stones. My doctor told me to drink lemon juice to lower My pH. I am seeing that lemon juice actually raises pH. What should I do to prevent my stones? I had my parathyroid checked, it was fine. Thanks, J.D.
Hi J.D., You have marked hypercalciuria and an alkaline urine. I am surprised that your stones do not contain appreciable amounts of calcium phosphate as well as calcium oxalate. Lemon juice or any fruit concentrate will indeed raise urine pH, as you have found out. The only proper approach for you is to be sure you know exactly what is wrong. Do you have simple idiopathic hypercalciuria, primary hyperparathyroidism – PTH is not enough, or what. Here is a good approach. Check it out and be sure about each step. Then, treatment will become clearer. Regards, Fred Coe
Hi: I am a frequent kidney stone sufferer since I was in my mid 20’s, I am now 49. I have been diagnosed with an over abundance of bile salts since my gallbladder was taken out 6 years ago and have had terrible diarrhea since then. This was causing me to not absorb any nutrients. The doctor told me to start taking Calcium Carbonate 600 mg with 800 mg of D3 added. This has worked wonders for the bile salts and has given me my life back over the course of 1 1/2 months of using it, but since then, I have passed at least 2 black stones in my urine. I HAVE to take the calcium carb/d3 supplements for the bile salts, so what are my options for the kidney stones that will not affect the calcium carb/d3 that I need for the bile salts? Please Help!!!!
Hi Cheri, The D3 is not the problem, it is the calcium. But, if you take it will your meals it should not cause stones. Try this: get 24 hour urine stone risk analysis – your physician can arrange – when you are using the calcium with your larger meals. If your urine calcium is still high lowering diet sodium will lower the calcium. Mention this to your physician and see what she/he says. Regards, Fred Coe
Do you have any information or advice for a carrier of Lesch-Nyhan’s Syndrome (HPRT1 Genetic mutation) regarding kidney stone formation, or other issues that carriers may have?
Hi Theresa, I do not have such information as I have not as yet attempted the genetic causes of stones. But I will make some effort to find out. Regards, Fred Coe
Dr. Coe, is there a over the counter item that can be taken that can assist in eliminating the formation of Uric stones in the bladder. Thanks
Hi Gordon, Uric acid stones always yield to potassium citrate. But you presumably have prostatic disease with retention and that can promote other kinds of stones. Perhaps you might want that fixed. Your urologist know the proper dose of potassium citrate. The article also mentions a starting dose. Regards, Fred Coe
Dr Coe, I take on a daily basis 1) Simvastatin 40 mg, 2) Warfarin 5 mg, 3) Tamsulosin .4 mg, 4) Sotalol 80 mg, 5) Lisinopril 2.5 mg. Would any of these drugs or combination of cause my body to produce Uric Stones? I pass a few small stones occasionally and urination is sometimes less than ideal. Thanks
Hi Gordon, These are not causes of your stones. Low urine pH and retention have produced them. Regards, Fred Coe
Dr. Coe is calcium citrate useful as a source of citrate to prevent calcium stones?
Hi Francisco, IN principle, but clumsy in that you have to balance both. Be sure potassium citrate is needed for your care – it is not necessarily so. Likewise, assess how much calcium you want from supplements. The extra calcium should be with your larger meals to block oxalate absorption. Rather a complex undertaking. Regards, Fred Coe
Any advantage of magnesium citrate vs potassium citrate vs postassium-magnesium citrate supplement in calcium oxalate stone formation? What would be the conversion factors from one to the other?
Thank you.
Hi Dr. Coe, and thanks for sharing your time and expertise so generously. So after having an ESWL for a Ca Oxalate stone with a 24 hr u baseline oxalate of 50mg/24hrs I started a restricted oxalate diet along with Ca Citrate 250mg with each meal. 6 weeks later the 24hr U Oxalate had dropped to 22mg/24 with a U Ca of 93 and Mag of 90mg/24hrs. I’m pleased but for the rather severe binding effect of the Ca Citrate despite dietary measures. I was wondering if substituting a dose of Mag Citrate perhaps 15cc of the 10mg/cc solution for one or perhaps 2 of the Ca Citrate doses might be a way of maintaining the benefits of the Citrate component and at least some of the Calcium component with an acceptable side effect burden? Thanks again.
Hi Stan, I am glad the calcium worked so well for oxalate. I do not know if magnesium will do it but why not try but then get another 24 hour test to be sure the oxalate is still low. Regards, Fred Coe
Hi Dr. Coe,
Could potassium citrate help in dissolving pancreatic stones or calcification of the pancreas? I have heard of using trimethadione, but that sounds risky and would require an off-label Rx.
Thank you for your time!
Hi Natasha, I know of no data supporting potassium citrate for pancreatic stones. Sorry, Regards, Fred Coe
Dr Coe
I have hypocitrauria with an increased PH and low magnesium on a 24 hr stone risk. It says I have high Brushite and high sodium urate in my urine presumably that’s what my stones are. Note: I have passed over 5 stones in the last 2 years and currently have 8 in my kidneys. 2 that measure 5mm and 2 that meas 3mm the rest are smaller. This all started during pregnancy and since I’ve have my daughter who is almost 2 years old. What is the best way to treat these stones and how to prevent them?
Thank you
Casey
Hi Casey, Lets begin with the actual stone analyses. You need to know, and since you passed 5 of them no doubt some have been analysed. I imagine they are indeed calcium phosphate, either brushite or hydroxyapatite. The high urine pH is part of the cause, usually high urine calcium is another part. The low magnesium is not obvious – often this is from diet issues, but I lack enough detail to help there. If all you have is low urine citrate and high pH, and urine calcium is normal, potassium citrate may help or not. It can raise urine pH and may or may not raise urine citrate. Are you forming more new stones or passing stones that formed while you were pregnant? Here, your physician has a main role. With all these ifs it is clear that there is not enough information for me to help much. Perhaps you might want to post more of it. Regards, Fred Coe
Thank you Dr. Coe for answering my post. I have never had a kidney stone analyzed because I have never caught one or saw one but have passed tissue and blood and had confirmed by doctors ultrasounds that I have indeed passed some. I do have a normal calcium urine result. I passed 2 while I was pregnant then passed 3 more right after I gave birth. Went to the urologist they scanned 5 in my kidneys. 6 months later they scanned 8 so I keep forming them and may still be passing some from being pregnant I don’t know. What is confusing me is the high sodium urate with brushite. It seems that treatment for these would contradict each other. Another note: Last few urine samples from primary care doctor results had a 6.5 PH so my PH has come down since my stone risk last year.
Thank you
Casey
Hi Casey, You are confused by the supersaturations; sodium urate and brushite saturations rise with pH, but this may have nothing to do with your stones. You cannot treat high urine pH, but you can lower urine calcium. Do you know your urine calcium and sodium excretions/day? Regards, Fred Coe
Calcium 107
Sodium
175
Brushite
2.01
Sodium urate
2.78
Hi Casey, your urine calcium is certainly low, so the high brushite SS must be from your high urine pH. I would mention to your physician that repletion of your magnesium – that is low – and simple potassium chloride might raise your urine citrate. It is simple and worth a try. Regards, Fred Coe
Thank you so much Dr Coe. I appreciate it and your work. Keep on being brilliant.
Calcium 106
Sodium 175
Brushite 2.01 (<2.00)
Sodium urate 2.78 (<2.00)
Hi Casey, I think I answered to this. The sodium urate SS is not relevant. That crystal is very rare. Regards, Fred Coe
Thank you your work. As I sit here getting up the courage to call the surgeon to begin the process of my 4th surgery for 99.4% calcium oxalate kidney stones, I found your page. I drink at least 1/2 gallon of water per day, eat a low carb diet favoring turkey, spinach, chicken, broccoli, cauliflower, beef, salads. I drink a turmeric/ginger tea regularly. I take 5 mg of lisinopril daily to combat the stones, and I pass usually 2 kidney stones per month… sometimes more and sometimes it seems like I haven’t had kidney stone related pain in a few months… can you please comment on adding insoluble fiber to my diet, and/or taking any type of supplement to help me pass them sooner before they get so big, or any other ideas will be greatly appreciated.
Hi Mark, since you form nearly pure calcium oxalate stones, treatment depends entirely on the 24 hour urine and blood testing. Here is a reasonable approach. The very worst approach is to assume or alter diet without information and a plan. Take a look and see if you have been fully evaluated. If not, get it done so prevention can work efficiently. Regards, Fred Coe
Dear Dr. Coe.
Many papers state against Potassium Citrate in patients with impaired renal function, but I haven’t found a cut point; so, what GFR level or KDIGO stage is safe for it?
Hello Doctor, Personally I have never seen hyperkalemia from potassium citrate in Stage 3, even 3b CKD. Stage 4 is a different matter, and I rarely have used it for such patients. Uric acid stone formers often have stage 3 CKD and I have used it many times. One thing, though, I do a one week fasting renal panel just to be sure. For patients taking an ACE or ARB I start low and check in a week. Regards, Fred
I had a kidney stone surgically removed about a year ago. It was analyzed as 10% calcium oxalate and 90% uric acid. I’m having a tough time following both the low oxalate and low purine diet. Since the stone was only 10% oxalate can I ignore those food restrictions? Seems like I don’t have many food choices. I am drinking a good amount of Crystal Light lemon each day.
Thank you
Hi Mark, you do not need a low oxalate diet nor a low purine diet. You need alkali to raise your urine pH. Here are my articles on uric acid stones – your stone. For the 10% calcium oxalate part, I would simply begin by stopping the uric acid stones – that usually is enough. Treatment to get pH above 6 will always stop uric acid stones. Do it with your physician. Regards, Fred Coe
Thank you for your response. Would you recommend continuing the use of Crystal Light?
Hi Mark, Sure. It is alkali. Get a 24 hour urine and see if the pH is above 6; if not, add more alkali as potassium citrate. What matters is the urine pH. You do not want sodium alkali – will not do as well for you. Regards, Fred Coe
I have calcium oxalate stones. I live in the UK. If there a citrate pill I can purchase OTC?
Hi David, The OTC pills are smaller than Rx pills so you need to take a lot of them. A single Rx pill is 1080 mg of the potassium citrate whereas the common OTC variety are around 200 or so – same units. But, be sure you should use this agent. Get an evaluation as to the cause of your stones. Here is a good article on that subject. Regards, Fred Coe
My doctor wanrs me to take potassium citrate for kidney stone prevention. They no longer make the crystal packets that dissolve in waster and I can not swallow the pills. They stick in my throat and cause severe choking I think there are liquid forms but my doctor is not familiar with them. Can you tell my if Effer-K or K-Lyte are good for kidney stone prevention
Hi Dian, Effer K is fine, K lyte is potassium chloride and will not work. Regards, Fred Coe
Dr. Coe:
Thank you for your helpful website and dedication. I had two general preventative questions for you. One is regarding potassium supplementation. I am desirous of meeting the daily potassium intake levels of 4,000 mgs.; however, I am also trying to lose some weight with general lower carbohydrate dieting and other modifications. As a result I am having difficulty reaching that level thru diet alone. I was confused about the optimum potassium supplement to consider taking to assist my intake level. Potassium alone, potassium citrate, magnesium citrate, magnesium potassium citrate, etc., and so on? Can you offer guidance as to type and amount?
Also, for general stone prevention, I wanted to know if I should limit or monitor daily phosphorous intake levels? Is there a daily limit as part of your kidney stone diet guidance? Thank you.
Hi Bill, Fruits and veggies are rather low in calories, so I wonder why the problem. They do have sugars, but most are slowly absorbed. I would try to get the potassium from the recommended 5 servings/d of these foods. Phosphate excess arises almost only from cola drinks – personally I would always shun them. Regards, Fred Coe
76 yr. old white male in excellent health. Very active (run, golf (walk), table tennis). Only med is .075 levothyroxine daily. However, form very painful uric acid stone every year or so. Current ph is 5.0, Take about 2 tablespoon’s organic 100% lemon juice (not from concentrate) in cold water almost daily at urologist’s suggestion. No meds recommended. Creatinine is 1.35. Vitamin D level low but now taking two OTC pills daily to increase. I try to drink a lot of water but not enough. Would you please offer advice. Worry about kidney stones. Thank you, so much.
Hi David, You are inadequately treated; urine pH needs to be above 6. The lemon juice is not right, you need potassium citrate 40 – 60 mEq/day and 24 hour urine monitoring to reach your goal. Vitamin D is not relevant to uric acid stones. Recurrent uric acid stone is never necessary. Regards, Fred Coe
Passed 2 CaOx stones (2more in kidney being watched) Initial 24 hr urine showed low citrate 355,ph 5.5. All else normal. Started on Potassium Citrate 10meq Bid. F/u labs showed K+ 5.7 and told to stop med. K+ returned to normal. Repeat 24hr now showed Citrate 271 , ph 5.9. If I can’t tolerate Pot. Citrate how else can I raise that level ? Have tried to increase fruit/veggie intake and drink Crystal light daily. Other suggestions appreciated. Thank you !
Hi Tina, I am surprised your serum potassium rose so with 20 mEq of potassium citrate. Did you possibly take it just before the blood draw? If so, the higher reading is misleading as serum potassium normal values are fasting. In your 24 hour urine what was your potassium excretion? As for crystal light a liter is equivalent to the two potassium citrate pills, so if your serum potassium does not rise with it then the prior value was spurious. Regards, Fred Coe
I am a 58-yr old woman who has had tiny kidney stones that have not prevented problems. However, after experiencing gross hematuria and pain in June 2017, I was told I had a 8mm stone and went in for ureterscopy. The procedure left me with a 2 cm bladder rupture on the extraperitonal dome, which was repaired. A month later I was diagnosed with a bladder stone that was attached to the bladder rupture site and it was removed. Stone composition was 90% CA hydrogen phosphate composition. I was put on potassium citrate pills for month but the calcified matter came back and they were discontinued. Completed a 24 hr urine test in April and was told to drink more citrate. Second stone matter was removed in April but calcified matter returned. Just had laparscopic surgery to re-repair bladder site and remove calcified matter. I am convinced that bladder is healed until I start any activity such as jogging and then I bleed from bladder and white matter forms. So confused on whether I should be taking citrate or not. My doctors have never experienced a case similar to mine. Desperate as I have had 5 surgeries in the past year for this same issue.
Hi Gretchen, From this note I see the stones are calcium hydrogen phosphate and I suspect that is calcium monohydrogen phosphate – or brushite. A prior note mentions high urine calcium, and I suspect that is idiopathic hypercalciuria. Potassium citrate is not ideal, and I would advise your physicians focus on the high urine calcium. Is it indeed idiopathic or caused by a systemic disease like primary hyperparathyroidism? You need a full evaluation for cause and definitive treatment to stop the crystals. Regards, Fred Coe
Does taking calcium citrate help reduce the incidence / formation of kidney stones?
Hi Randy, All the trial evidence is in the article you commented on. I think it works. I made another summary of the trials here, and perhaps you will find it clearer. Regards, Fred Coe
Would you expect introvenious citrate (used as anticoagulant in plasma donation) to have the same results as citrate salts taken orally?
My assumption is it would bind to calcium in the blood all the same.
,T
Hi T, Yes, but only for the few hours of the infusion and then gone away. Citrate will indeed bind to blood and if infused into someone at too high a rate has risks of lowering calcium and causing tetany. Of course in a blood donation it only goes into the container. Regards, Fred Coe
Have passed multiple uric acid stones (three tested) six, this year so far, eight last year. (Yes, I have a log), 1-4 mm. Aside from the first two (one on each side) which put me in the ER, most pass without too much pain, but the last one did get lodged in the penis for two days. Can’t take allopurinol – allergic. Now doctor wants me to take Uloric, but insurance won’t cover. Test results are normal. (PH>5). Made lemonade from real lemon juice (2tbs/day with Splenda) but haven’t used in last three weeks. Still had stones while taking. Any recommendation? Do take BP meds that may lead to dehydration.
Hi Vince, uric acid stones ARE low urine pH; it is one to one, so you need alkali.I presume the >5 value you mention is from a 24 hour urine; this should be a real number, and one needs a value of 6 for safety. If the number you quote is from a urinalysis, it is without value for stone prevention. Allopurinol cannot prevent uric acid stones, only raising urine pH to 6 on a 24 hour basis. Routine potassium citrate 10 mEq capsules 2 – 3 twice a day are so specific for uric acid stones almost all insurance plans will cover it if the case is made. Because this is exact treatment that always works, get it for yourself as soon as possible. Here is a better uric acid stone article. Regards, Fred Coe
Hi Vince, I answered this and I presume this is a duplicate. Regards, Fred Coe
Had 2 kidney transplants, last was March 2017. Chronic kidney stone former. Ca oxalate and IJ bypass 42 years ago. What can help me save this kidney? I am a CRNA and see a urologist and transplant nephrologist. Taking but B BID and potassium Citrate 90 mEq per day as well as Ca citrate 6 tabs per day. Trying to do low oxalate diet. Is there anything else I can do to help myself?
Hi Cindy, You have a long standing and old bypass, and I gather have lost your native kidneys and a prior transplant. Undoubtedly this has been from excessive oxalate itself arising from the bypass. If I am right the only way to save this new organ is to remove the bypass. As this is very serious, I would bring my note to the attention of your physicians. Presumably they already know anything I can say, and perhaps you have some other reasons for kidney loss. But bariatric surgery, especially the old bypass procedures, can be very dangerous. Regards, Fred Coe
I have a long history of Calcium Oxalate Kidney Stones on both sides for over 30yrs. Over the years I’ve tried various dietary changes, including low-oxalate, potassium citrate tabs, and drinking lots of water yet I continue to make stones.
Early on I had several attacks that required cysto basket removal procedures.
For the next 10yrs, I was being treated with several preventive ESWL procedures occurring in 6mos-3yr intervals and which allowed me to pass small stones on my own without pain.
The past 10yrs I’ve gone to a different urologist with concern of possible collateral damage to other organs by continuing periodic ESWL procedures and uses cysto laser lithotripsy instead.
Until recently, I did not require intervention since around 2006 and attribute that to the increase of Potassium Citrate 2x/day and increasing my water intake. However in July I needed to have laser lithotripsy for a stone on the left side deemed too large to pass on my own. I’m also being monitored for more stones on my right side and will need to decide at a follow-up exam if more intervention is needed. The urologist has recommended that I drink my water with pure lemon juice and have being doing so since the laser procedure. I am hopeful this could prevent the growth of the existing stones and preventing new ones, but I’m skeptical given everything else I’ve tried.
I am very concerned about having another laser surgery because it requires general anesthesia and I had a very lengthy and debilitating reaction to the combination of anesthesia and pain meds. For several weeks my symptoms included, much weakness, difficulty focusing, lightheadedness, difficulty taking a full breath, and all this and more alternately coming in waves. I had several tests post surgery to rule out any serious issues and did not take the opipds and benzos for more than a couple of days so it seems the anesthesia may have been the cause.
If intervention is needed for the existing stones, I may decide to go back to having ESWL done because of sedation instead of general, but obviously my main question is how to prevent these stones in the first place?
Hi Al, SWL is not ideal but perhaps the anaesthesiologists involved could contrive an approach for you that causes less debility. As for prevention, lemon juice is a silly thing – no trial, merely a way to add citrate that could be added with citrate itself and more reliably. But you are right altogether; prevention starts with comprehensive 24 hour and serum testing, and treatment follows what is found wrong. Here is a good article on the subject. Regards, Fred Coe
Hello, I was told by my doctor to take calcium citrate after every meal and snack. That seems excessive, I just want to make sure I’m not taking toooo much. Also, I read about Alkali and is that just an alkaline supplement to take additionally with calcium citrate? I reread a few times and I just wasn’t able to find the answer above. Thank you for your time!
Savannah
Hi Savannah, The article is about potassium citrate; calcium citrate is a form of calcium supplement that had alkali content but is intended to provide extra calcium. I am guessing you have calcium oxalate stones and high urine oxalate, and your physician is attempting to lower urine oxalate with increased diet calcium. That is a workable strategy. Possibly s/he intends treatment for bone disease. Either way, the calcium is the intent in use. You should discuss this with your physician. Regards, Fred Coe
My daughter has had kidney stones in both kidneys. In the last 5 months we have had 2 surgeries and was just informed that the
Third surgery in needed but they are not sure that they will be able to reach the stones.
Getting very concerned as to why we keep developing stones in the matter of weeks. I am beginning to think the doctors are lost for words. We did a 24 hour urine which showed her stones are made of calcium phosphate. She drinks 72 ounces of water a day which has created issues at school.
Asking for some advice … is there any meds we can go one ?
Hi Bev, 24 hour urines cannot disclose the kind of stones – you need to analyse the stones themselves. The urines help determine cause and focus treatment. I suspect her urine calcium and pH are high. The amounts of water show why monotherapies are not ideal. Just 2.5 liters of urine a day are enough and the other problems can be fixed as well so she relies on more than one treatment approach. Here is my favorite article on prevention. Regards, Fred Coe
I was put on Potassium citrate for uric acid stones (in the past I had calcium oxalate stones) I was very sick from the meds (very upset stomache which lasted weeks even after stopping the meds) They want me to try sodium bicarbonate now Can this help and do you recomnend? Thank you
Hi Donna, Sodium alkali work for uric acid stones but the sodium load can raise blood pressure. If your physician can deal with that, the approach is perfectly sound. Regards, Fred Coe
Hello Dr. Coe. I am 60 years old and have had kidney stone surgery treatments on three occasions once in a water bath 30 years ago, a shockwave procedure perhaps 3 years ago then most recently a treatment where a device was sent up inside my bladder and urethra to breakup and remove the stones last year 2017. I believe my stones have been calcium oxalate. An interesting thing occurred this year after I went in for a colonoscopy. After taking the preparation called Golitely a polypropylene glycol mixture. I was cleaned out and went for the colon test. A day or two after the test I started feeling kidney pain of perhaps 6 out of 10. I passed a small stone at home but then decided to go to emergency room and while I was waiting had a strong urge to pee. I then passed a 11mm then 9mm stones but only felt pressure upon the release…not tearing, scaring pain like was previous stone symptoms. Looking at the stones they appeared to be tan, smooth surfaced and shaped like footballs instead of crystalline and sharp. Could I have stumbled upon a way to “melt the surface of these stones” so they could be passed naturally without further surgery? Being a commercial helicopter pilot requiring annual physicals it is in my best interest to find a solution to my kidney stone issues if possible. I suppose the latest stones could have been Uric acid in nature also?
Thanks so much for your comments.
Hi George, I do not think so. The propylene glycol is not absorbed and would not be in the urine. It will not melt calcium stones. Get the new stone analysed to be sure what it is made of. Regards, Fred Coe
Hi Dr. Coe, I was wondering if you could give me your opinion.
I have been told that my citrate is low, I have done 3 urine collections is the past 12 months
after having a calcium oxalate stone.
1st collection:
Volume 2479ml
Oxalate 452 umol/24h
Citrate 0.5mmol/24h *L
Calcium: 6.06mmol/24h
2nd collection:
Volume 4000ml
Oxalate 678 umol/24h *H
Citrate 1.1mmol/24h
Calcium: Lab error
3rd collection:
Volume 2230ml
Oxalate 401 umol/24h
Citrate 0.9mmol/24h
Calcium: 8.31mmol/24h *H
Currently I am taking magnesium/potassium citrate (2 tablets a day)
each 1 contains:
1072mg potassium citrate
412mg magnesium citrate
=
15.8meq citrate
10.5meq potassium
5.3meq magnesium
My calcium went up on the last collection, however I have increased
dietary calcium (is this a concern?) my oxalate has lowered as a result though I think.
The citrate certainly keeps the PH of the urine very high when I check my urine with the dip strips
which I’m told will avoid urine to get too concentrated.
Many thanks
Regards
Ray
As per the citrate, do I necessarily need it judging by the results? If so, Is it safe at this dose and would it be safe
to take everyday, forever?
Blood magnesium and potassium were checked recently and
were fine.
* forgot to say, I started taking the citrate supplement after the 2nd collection, around 3 months before the
most recent (3rd collection),
Hi Ray, your urine citrate is indeed low, low enough to pose a statistically increased relative risk of stones. I gather these low citrate levels were found despite taking potassium citrate – I judge about 20 mEq/d. The urine pH is not mentioned but you find it high at home. I do not know enough about your case to say too much except that if your stones are calcium phosphate, and citrate raises urine pH and fails to raise urine citrate it may not be ideal to use it. Your urine calcium is indeed high. Perhaps your physician and you might want to be sure of an ideal diet and use meds over that base. Sometimes a better diet irons out your kind of problems, and allows for a clearer view of what more is needed. Regards, Fred Coe
Hi Dr. Coe, apologies for the delay in replying.
Yes, these citrate levels are despite the supplement containing both magnesium and k citrate.
My stones are calcium oxalate.
My intake of protein the day of the 24h urine was pretty high (100g+), so that might explain the calcium level
which until then has always been normal. I have my consumption now.
Below is the last set of results:
•Parathyroid Hormone (pmol/l) 17/01/2019 5.51
•Albumin 17/01/2019 48
•Calcium 17/01/2019 2.41 2.08-2.65 mmol/L
•Adjusted Calcium 17/01/2019 2.37
•Phosphate 17/01/2019 1.19 0.80-1.50 mmol/L
•Alkaline Phosphatase 17/01/2019 79 30-130 U/L
•Albumin 17/01/2019 48 35-50 g/L
•Total Bilirubin 17/01/2019 19 0-20 umol/L
•Alkaline Phosphatase 17/01/2019 79 30-130 U/L
•Alanine Transaminase 17/01/2019 38 7-40 U/L
•Magnesium 17/01/2019 0.88 0.70-1.00 mmol/L
•Serum Sodium 17/01/2019 141 133-146 mmol/L
•Serum Potassium 17/01/2019 4.4 3.5-5.3 mmol/L
•Serum Bicarbonate 17/01/2019 31* 22-29 mmol/L
•Serum Creatinine 17/01/2019 65 62-115 umol/L
•Estimated GFR 17/01/2019 >=90
•Colour UA, POC 17/01/2019 Light Yellow
•Clarity UA, POC 17/01/2019 Clear
•Glucose UA, POC 17/01/2019 NEG
•Bilirubin UA, POC 17/01/2019 Negative
•Ketones UA, POC 17/01/2019 NEG
•Spec Grav UA, POC 17/01/2019 1.015
•Blood UA, POC 17/01/2019 NEG
•pH UA, POC 17/01/2019 7.0 PH meter 6.13
•Protein UA, POC 17/01/2019 NEG
•Urobilinogen UA, POC 17/01/2019 3.2
•Nitrite UA, POC 17/01/2019 Negative
•Leukocytes UA, POC 17/01/2019 Negative
•Urine Oxalate:Creatinine Ratio 17/01/2019 40* <33 umol/mmol
•Urine Calcium 17/01/2019 2.72
•Urine Creatinine 17/01/2019 2.881
•Urine Calcium/Creatinine Ratio 17/01/2019 0.94 Should be less than 0.7
Suggest maintain normal calcium in diet, add effercit-K 2 tabs at lunchtime.
Thanks
Regards
Ray
Hi Ray, You give no new citrate so I suppose it was in the prior note. With very high protein intake citrate will fall and calcium will rise. I would never lower diet calcium, as oxalate will rise, and you have a skeleton. Here is a proper diet. As for the potassium citrate, I see nothing wrong with it. There are no other special abnormal values in your list as you yourself can see. Regards, Fred Coe
Thank you very much for the diet link and the info regarding the potassium citrate and protein.
Regards, Ray
Hi Dr. Coe,
Is there a difference between potassium citrate and other citrate such as magnesium citrate In helping with increasing urinary citrate levels ? Reason I ask is that I’m feeling a little bit anxious lately and I’m not sure whether it might be linked to my potassium citrate supplement. Alternatively i could try getting citrate from natural dietary sources. Many thanks , regards Ray
Hi Ray, Mg citrate has limited GI tolerance, and no special advantage. Fruits and veggies give you lots of potassium along with anions that are converted to bicarbonate like citrate is, and 5 servings a day can substitute for as much as 40 mEq of K citrate pills. None of the agents affect the brain, or cause anxiety. Regards, Fred Coe
I have 80% uric acid Stones 20% calcium oxalate. I have a 1.3 CM down in my left kidney lower pole. With heart and lung disease my doctor does not want me under general anesthesia. What is a safe way to get rid of the Stone. Thank you
Hi Mary, The uric acid stone will dissolve with alkali treatment to raise urine pH, so one possible route is just that – see if stone bulk decreases. Of course you need 24 hour urines to determine the dose of potassium citrate and also other stone risks related to the calcium oxalate – which will not dissolve but may grow if not managed. I do not know if spinal anaesthesia is effective for ureteroscopic stone removal, but that also seems an option. Regards, Fred Coe
What about Struvite stone with highly alkaline urine. Litholink test shows 24 hr urine citrate is low at 187 with urine pH 7.855. Will K-citrate be useful in this case?
Hi Amit, if your stones are struvite they are due to infection and K citrate will be of no help. Be sure about the stone analysis, and if possible send multiple stones. Everything depends on the stone composition in your case. Regards, Fred Coe
Hello dr.,
My urologist wants me to try to dissolve my uric acid kidney stone . It is 1.3 cm. He told me to take 15 meq of potassium citrate. This seems kind of low. Could you tell me what is the average dosage of potassium citrate to dissolve a stone of this size? Also what is the success rate? He says it’s less than 50%. Thank you
Hi Mary, It is seemingly a low dose. But one always does a followup 24 hour urine to see if the pH has risen to 6 or more. If it has, the uric acid can dissolve. What he/she means about 50% is that the stone is large and dissolves from its surface, so it is a slow process. As it dissolves, the stone may fragment, necessitating stone passage or possible surgery. But worth a try. For long term prevention, it is a necessity. Here is a better article for you. Regards, Fred Coe
My urologist is a doctor of very few words. We’re trying to dissolve a uric acid Stone in the lower pole of my kidney. He just did a 24-hour urine test and a blood test. The uric acid in my blood is normal however in the urine tests its high. How could blood uric acid be normal but urine uric acid be High? Thank you
Hi Mary, Uric acid stones form because urine is too acidic – pH to low. Blood uric acid can be normal, as can the amount of uric acid in the urine. SO treatment is to make the urine more alkaline. Here is a good article on the matter. The amount of uric acid in the urine is itself of little concern once the urine pH is raised above 6. I a quite sure your physician knows all this. Regards, Fred Coe
I had two calcium oxalate stones last year. Part of Dr’s recommendations was drinking lemon juice in water, and after reading on this site I understand why. Three questions: 1) This will inhibit stone formation/growth, but will it dissolve any existing fragments also? 2) Is there an optimal dilution of lemon juice to water, or is more always better on the lemon juice? 3) He stated always use fresh squeezed, not bottled – would you know why he would say that? Thanks!
Hi Karl, Honestly, citrate is citrate. If you ate the US recommended 5 servings a day of fruits and veggies you would get the same or more citrate. Lemons have a problem, being acid the juice can erode tooth enamel. As for fresh etc that is from my point of view without meaning. In fact, a reliable source of potassium citrate is an inexpensive diet beverage – Crystal Light. We tested citrate contents in a number of juices and it won. As for use of citrate, it is only valuable when 24 hour urine citrate is not already high. So 24 hour urine testing is a valuable preamble. Take a look at this article that reviews a more exacting treatment protocol that begins with diet and uses meds as an add on as needed. Regards, Fred Coe
Is there anything one could consume that might act as a surfactant to encourage any small stones that begin forming to loosen and be eliminated before they grow larger?
Hi Karl, Citrate is not a surfactant but does reduce crystal formation. I have no surfactant ideas. Sorry. Regards, Fred Coe