
 You have idiopathic calcium stones. That means much of this site applies to you and your disorder. But the many articles read without a guide or sequence can confuse. You would be best off reading here, and following links as they come up. Of course you are free to browse as you like, but if you want a guide, I am here. Pieter Brueghel II (The Younger) A Village Fair (Village festival in Honour of Saint Hubert and Saint Anthony) 1564/1638 (Mackelvie Trust Collection, Auckland Art Gallery Toi o Tāmaki, purchased 1961) shows a crowd, which is appropriate for this most common kind of stone former.
You have idiopathic calcium stones. That means much of this site applies to you and your disorder. But the many articles read without a guide or sequence can confuse. You would be best off reading here, and following links as they come up. Of course you are free to browse as you like, but if you want a guide, I am here. Pieter Brueghel II (The Younger) A Village Fair (Village festival in Honour of Saint Hubert and Saint Anthony) 1564/1638 (Mackelvie Trust Collection, Auckland Art Gallery Toi o Tāmaki, purchased 1961) shows a crowd, which is appropriate for this most common kind of stone former.
Begin Here
You should not use this chapter unless you have come to it by the right path. I assume you have, but if not I could mislead you. If you have not learned about the needs for personalized treatment (Chapter One), the rudiments of how stones form (Chapter Two), the proper way to evaluate your condition (Chapter Three) or how patients can be placed into their phenotypes (Chapter Four) go back. It is not enough to come to where you want to be, you must come by the right way to guard against mistakes. Even the most careful negotiator of the paths can go wrong. If you have done all that comes before this place, then go on.
What Traits Define You?
Of course, you certainly form calcium stones and a properly conducted search has disclosed no systemic diseases as a cause for them. Thence, idiopathic calcium stones. Family members often form stones – father, mother, sisters, brothers, or children. Being without obvious cause, stones cause alarm and confusion. Without a cause how can one prevent them?
There are Three Kinds Of You.
The most common is an idiopathic calcium oxalate stone former (ICSF). Start here, and read about your traits. The less common version is an idiopathic calcium phosphate stone former (IPSF). Least common is the brushite kind of calcium phosphate stone former (BRSF). Both are in this article, so I would read here. All three kinds were no doubt included in the trials of water, potassium citrate, and thiazide diuretics for stone prevention. I say this because when you read the trial articles many simply mention calcium stone formers. Also, stone analysis not rarely used chemical or optical means, not modern infrared spectroscopy less prone to error.
Urine Abnormalities Cause Your Stones
We Have Long Known This
Physicians observed decades ago that stone formers exhibit hypercalciuria, hyperoxaluria, hypocitraturia, low urine volume, and high urine pH. If you have not already encountered these terms, hyper and hypo mean above or below some proposed normal range. pH measures acidity or alkalinity. The physicians who observed these traits were clinical investigators, scientists. From their observation arose all of modern stone prevention. But practicing physicians in general do not use 24 hour urine samples in their work. They use spot samples, some urine provided by a patient for, as an example, urinalysis. While adequate for detecting blood or infection, such samples fail for stones. Urine levels of calcium, oxalate, citrate, volume and pH vary with meals, and from day to night.
Research Has Tightened the Link
Gary Curhan has proven a strong association between levels of urine calcium, oxalate, citrate, and volume and formation of 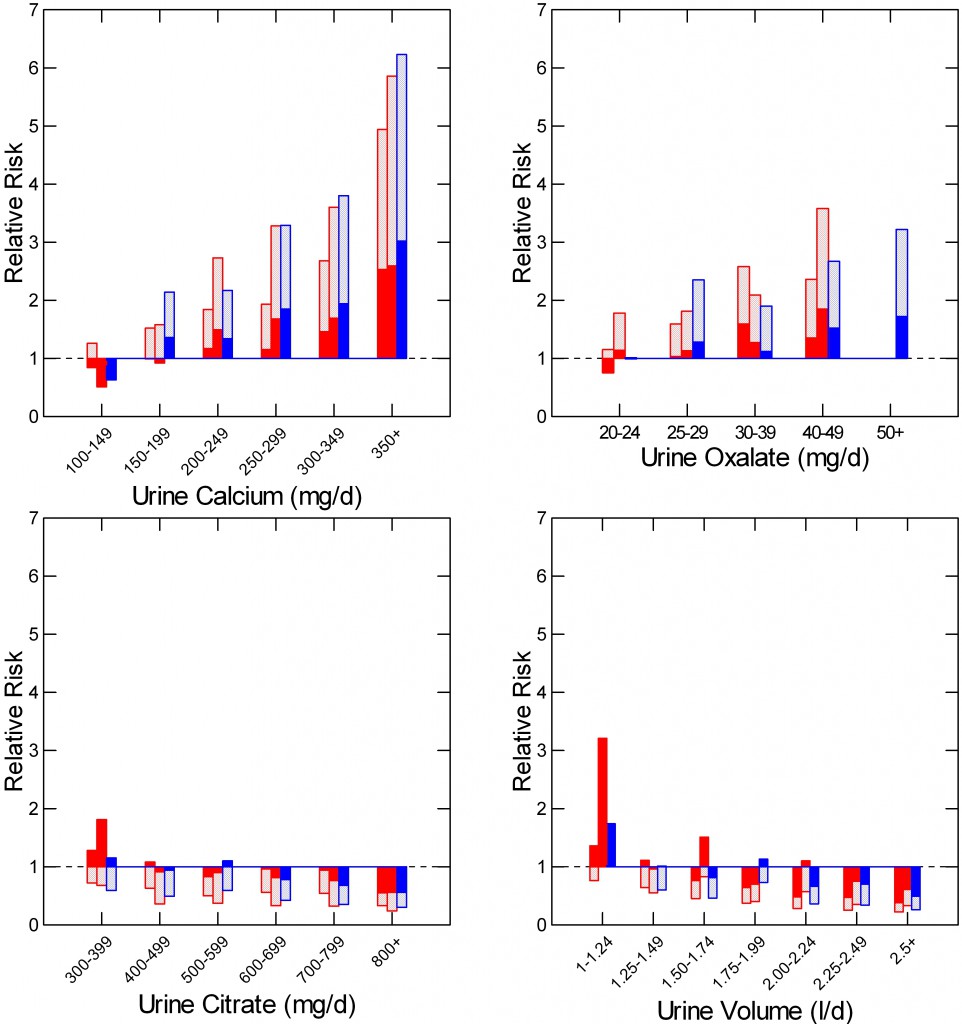 new stones. His work substitutes for the idea of hyper and hypo actual risk assessments for specific levels of these urine measurements. As the older notion of hypertension as a cause of stroke has evolved into graded risk ratios for stroke at different blood pressures, we can connect different urine calcium, or oxalate, or citrate, or volume levels to risk of stones. These risks act through supersaturation. Unfortunately Curhan has not provided the risk ratios for stones by supersaturation level – as yet.
new stones. His work substitutes for the idea of hyper and hypo actual risk assessments for specific levels of these urine measurements. As the older notion of hypertension as a cause of stroke has evolved into graded risk ratios for stroke at different blood pressures, we can connect different urine calcium, or oxalate, or citrate, or volume levels to risk of stones. These risks act through supersaturation. Unfortunately Curhan has not provided the risk ratios for stones by supersaturation level – as yet.
Urine Calcium
The the upper left panel shows urine calcium in 6 ranges in the common unit of mg/day. The height of the bars shows relative risk of becoming a stone former, while the bottom of the bars marks the lower 95th percentile. Then that bottom lies above 1 – no extra risk – risk of new stones is very likely present. The three bars show results for two groups of women (red) and one for men (blue). This work replaces the old idea of hypercalciuria as a threshold or cut point with the newer more fluent idea of a graded risk that begins at about 200 mg/d and rises proportionate to the amount of calcium lost.
Urine Oxalate
The upper right panel shows the same for urine oxalate excretion. Risk begins at about 25 mg/day. The magnitude of risk increase by calcium exceeds that for oxalate.
Urine Citrate
Being an inhibitor of crystallization and calcium binding, citrate lowers risk, so the graph reads upside down to the upper ones: Relative risk is safely below 1 (top of bars below the dashed line at 1) by 400 – 500 mg/day) and falls progressively with more urine citrate.
Urine Volume
Read like the citrate graph, increasing urine volume erases risk – tops of bars below 1) by 2 – 2.24 liters/day. For safety I like 2.5.
Urine pH
Though low pH fosters uric acid stones and high pH calcium phosphate stones Curhan found no clear relationship between pH and risk of becoming a stone former. I believe because pH values at both extremes pose risk a clear risk relationship because blurred.
Altering Risk Factors to Lower Supersaturation Prevents Stones
Your phenotype perfectly illustrates the relationship between drivers and the final pathway. Lacking systemic or kidney diseases as a cause of stones your final pathway is urine supersaturation, and the drivers the proven four risk factors – plus pH if your stones are calcium phosphate. They are modulated by fluids, diet, and medication to lower supersaturation in a way that is particular your specific pattern of abnormalities and pattern of lifestyle, diet, occupation and habits, as well as preferences. One article details the strategy for achieving synergistic use of fluids, diet, and medications in practice. I suggest you read it now.
Barriers to Urine Testing Can Delay or Obscure Diagnosis
Clinical Labs May Perform Urine Stone Risk Testing Poorly
Hospital laboratories and even major national laboratories perform 24 hour urine testing not only in a poor way but a way that discourages physicians from their use. Who will provide a container, instructions for a proper collection? How and by whom will these bulky heavy collections get to the laboratory? Blood concentrations vary over a small range being essential for life. Urine concentrations vary over 10 to 100 fold ranges. So laboratories find urine measurements cumbersome and often send them away to the small group of them that specialize.
Urine Stone Risk Reports Can Baffle Physicians
Most important, supersaturation is calculated from 12 urine measurements. A laboratory printout of 12 measurements, often concentrations and 24 hour excretions running down a long typed page – that kind of lab report baffles any reader. Worse yet, sequential measurements over time accumulate as clusters of these long typed pages. Effects of treatment, good or bad, hardly shine out.
People Dislike Collecting 24 Hour Urine Samples
Why not! Cumbersome, a nuisance. And the most important days to collect on invariably are the least convenient: At work, or when busy with children, or outside in summertime playing golf. Weekends seem ideal. What if all the abnormalities that caused your stones show up only at work? Blood tests are simple. A few minutes and done. Urine testing looks at life lived not into the walled garden of the body’s interior held constant throughout life by the vast unconquerable forces of life. It is this way. Unlike blood urine composition varies widely as the kidneys work to keep things in blood constant. And, as they do this, stones can form in them. You want to test when they are put to the hardest work your life imposes, not on Sunday when you read the newspaper.
Shun Random Remedies
Being so common, and without a named disease to cause your stones, you are the ideal target for homely advice, well and not well intentioned. Grandma may not know how to prevent your stones. If you read Chapter One you already know that ‘just drink a lot of water’ is mediocre advice, poor even. Many offer remedies with no known value but their own enrichment. Especially shun sudden impulses toward a quick home fix. Your odds are poor.
You Have Risk of Bone Disease
Because of idiopathic hypercalciuria and perhaps just your underlying stone disease your risk of fracture is above normal. This link goes to a broad article on the US diet and its ability to promote stones and bone disease. That article links to more basic articles on the ideal kidney stone diet. They make clear, as does the treatment article linked to in the preceding paragraph that diet is all important.
Articles on Diet and Fluids
Diet
This is not always the case for stone formers, and the diet and fluid problems you have are not the same as for, as an example, someone with bowel disease. In your case the one ideal diet matches the ideal diet for the whole of the US population. Think about that. No physician can scruple about such a diet. There is no reason to wait or decide. It is ideal. Read about it and use it. Many detailed articles concern aspects of diet. Here is a good reading list. Kidney Stone Diet: Science of the Kidney Stone Diet; Our Diet Promotes Stones and Bone Disease; The Kidney Stone Diet; How to Eat the Kidney Stone Diet Sodium and Calcium: How to eat a low sodium diet; How to Eat a Low Sodium High Calcium Diet Sugar: Science and the Politics of the Kidney Stone Diet Protein: Does Too Much Protein Increase Stones or Damage Bones?
The Special Problem of Oxalate
If your urine oxalate is high enough to be a stone risk, and you produce calcium oxalate stones lower it. But remember that high calcium intake will lower urine oxalate provided the calcium is eaten with the meals that contain oxalate. So what you need to do about oxalate depends upon what is found with a high calcium diet. In general you are best off avoiding the worst offenders with a goal of below 200 mg of oxalate. This means obsessive compulsive behavior about every morsel of oxalate containing food is not worthwhile. It detracts from the broad theme that all modalities of a good diet and proper fluids need to be together so no one issue needs be driven to its outer limits. How To Eat a Low Oxalate Diet Do You Need a Low Oxalate Diet?
Fluids
To say ‘drink, drink, drink’ seems madness to me. About 2.5 liters a day of urine volume is ample. Stone risk has fallen most of the way by 2.25 liters a day of urine volume. When all aspects of the diet are in place, that much fluid as you need in your climate and job to achieve such volumes is enough. Many varieties of fluid will work for stone prevention, so monotony is not necessary.
Thiazide Diuretics and Potassium Citrate Can Prevent Your Stones
Both have their trials. But how do we use them? When? I use them when diet and fluids fail to reduce supersaturation by at least half or if new stone form despite lowered supersaturation. But my approach has no support from a trial. Here are articles on thiazide and citrate Thiazide for stone prevention Potassium citrate for stone prevention Their integration with diet and fluids: Treatment of Idiopathic Calcium Stones. I already linked to this article but do so again as it is the most comprehensive.
How to Read About Your Condition
Go back to the top and begin reading the blue highlighted links in order. That is your best approach. They will take you where you need to go.
This is brilliant Dr. Fred Coe, I assume you will be publishing it in book form? I am wanting to print it and give it to my doctors. Or will this not be an acceptable thing to do now?
Thank you for all that you do. You are also a very poignant author that writes with a lot of spirit. Thank you for this. I think the last kidney stone book was published god knows when……best regards, Laura Bousada
Hi Laura, Thank you for saying so. I hope people benefit. You are right, my last kidney stone book was published years ago. I do have a huge multi author book coming out in the next year, but it is a medical text pure and simple. I had not thought of print publishing the guide book but when the remaining articles are finished perhaps that would be a good idea. Warm regards, Fred
I have found the depth and the science behind kidney stones and passing stones amazing. Hopefully I’ll never have another once I have the current one cleared up following the protocols you and Jill have outlined that apply to me.
You would be doing all of us a great favor if you did publish the guide book. I have had a lot of medical and health and dietary challenges in my life and documenting all this in print so I can properly study it and take notes relating to my situation has been time consuming to say the least. Many do not have the time or means or skill set to accomplish what I have and they need a print version. Please do!
Thanks, Christine, you are the third person to say this, so I guess I should think about it. I have a huge kidney stone book coming out – 1000 pages, for physicians, but this would be for patients. Ward regards, Fred
Question:
My 24 hour urine numbers are all in the normal range (oxalate 22, citrate 664, calcium 152) but urine volume was low (1588). Should I make dietary modifications or just focus on increasing fluids? I have passed one stone (100% calcium oxalate), have another one that the urologist feels isn’t going to budge, and have some sand-granule sized ones in the other kidney which have not changed over 2 years, but I’d also like them to not grow!
Hi Alison,
Drinking enough fluids will indeed help. Getting urine output to about 2.5 liters per day is helpful in stone prevention.
j