 Kidney stones form at the tips of the renal papilla, and what forms them is the functions of the kidneys as driven by the needs of systemic homeostasis – maintenance of constant and normal blood levels despite wide variations in intakes.
Kidney stones form at the tips of the renal papilla, and what forms them is the functions of the kidneys as driven by the needs of systemic homeostasis – maintenance of constant and normal blood levels despite wide variations in intakes.
Stones themselves, obstruction from their passage, and consequences of infection and surgery all can damage kidneys. Multiple studies have linked stone forming with kidney disease, usually mild but sometimes serious.
Kidney disease is detected mainly by tests of glomerular filtration.
Even more, the very formation of stones depends in a way on the high filtration and subsequent reabsorption of critical materials like calcium.
Given this anyone with kidney stones needs to know what filtration is, how physicians measure it, and how filtration measurements allow us to dissect out what is really causing stones.
All this is what I have put into this article. It is long, as my articles often are, but very informative.
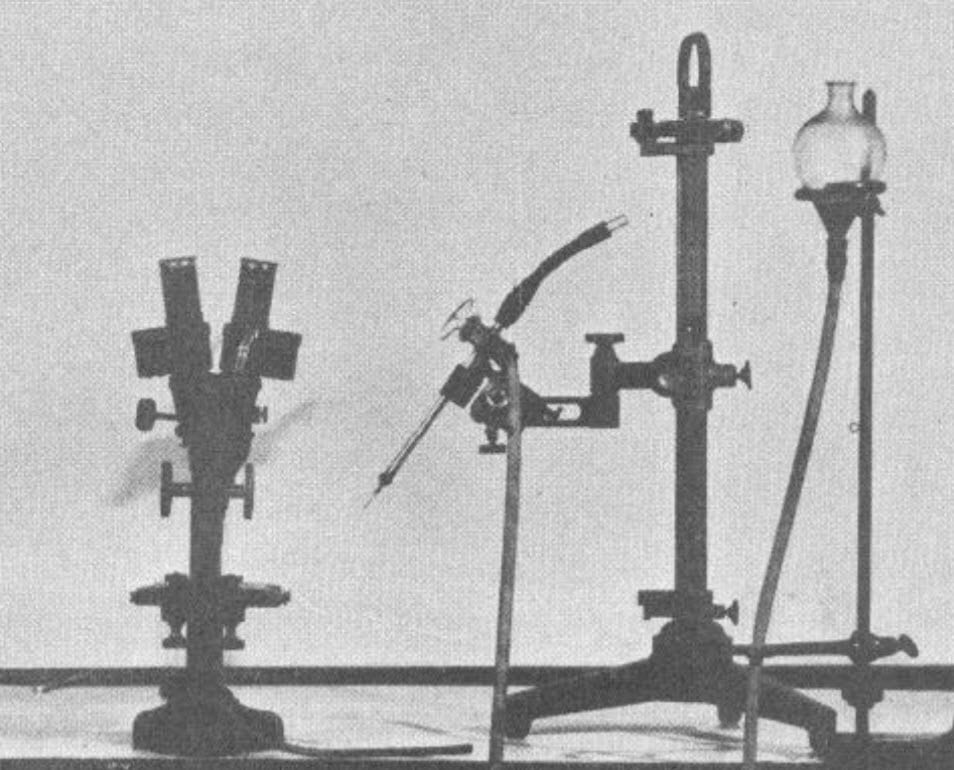
The featured photograph shows the first equipment for micropuncture of kidneys, the technique that literally made it possible to know how it worked. The reference is to a review that gives PDF links to various ancient articles.
High Filtration Fosters Stones
Materials Enter the Nephron at Plasma Concentrations
To make the common calcium oxalate stones kidneys must do the work of supersaturating tubule fluid into urine. That work begins with filtration that provides the tubules with the raw material for such final urine. At the same time, kidneys must excrete materials at rates demanded by systemic needs. Because filtration merely provides these at their concentrations in the blood plasma, kidneys often must reabsorb a large fraction back into the blood or in some cases actively secrete materials from blood into the tubules to enrich urine with them and enhance their removal from the body. Calcium illustrates the former, oxalate the latter.
Some materials, like calcium, are bound to molecules too large for filtration – like proteins. They indeed enter the nephron by filtration but at the plasma concentration of the unbound fraction. To get this so called ‘ultrafilterable’ concentration, one makes an ultrafiltrate of plasma in the laboratory and measures the concentration in that filtrate. Calcium, magnesium, and phosphate are stone related molecules that require this step.
Filtration and Urine Volume are Independent
Filtration rate, being the very basis of kidney function, is regulated by the needs of the entire organ. But the body determines through many sensors and regulators how much water must be lost per minute, per hour, per day in the final urine. In fact, water itself is filtered in vast excess of final urine excretion. So the concentration of filtered materials can be potentially immense.
Let us say, as a common example, one liter of water need be lost in the urine in a day, and the kidneys filter 100 liters in that day. If so, 99% of filtered water must be reabsorbed – a hundred fold concentration of the filtrate. Were none of the filtered stone forming materials – calcium, oxalate, phosphate, uric acid, and the like simply filtered and passed through, they would be concentrated 100 fold, each. That would lead to catastrophic crystallization.
In fact, most of these are extensively reabsorbed back into the blood. This reduces their urine concentrations down from the 100 fold baseline set by water regulation and glomerular filtration. If all these reabsorptions and urine water loss were kept the same and filtration raised to 150 liters per day – the actual mean value among normal people – their baseline concentrations sans reabsorptions would be 150 fold increased. Contrariwise, if filtration were 75 liters per day, their baseline before reabsorption would be only 75 fold.
So the higher the filtration, the greater the stringency imposed on reabsorptions to maintain acceptable supersaturations in the face of demands for water conservation. This is structural. It means that control of reabsorption of key materials like calcium and citrate critically determine stone risk.
Secretion is Into A Large Volume
Oxalate is the only stone risk material secreted. Secretion means that filtration is not the only one way in to the tubules and the urine. Kidneys can actively move oxalate from blood into the tubule fluid and ultimately the urine or, in some cases, reabsorb filtered oxalate back into the blood. Where it comes in from secretion, high filtration makes things safe – crystals will not form in the early parts of the kidneys. But as water is removed back into the blood even slight excesses of secretion, or reductions of reabsorption, can raise stone risk a lot.
About Evolution
Do I believe for a moment that evolution would not act to balance reabsorptions and secretions against filtration rate? Not for a moment.
In evolutionary time, renal and urinary crystallizations must lower the fitness of the species and lead to change or extinction.
Because the physical laws that govern crystallization are prebiological and unalterable, evolution must always work around them to achieve fitness of organisms to changing environments. Obviously, therefore, the higher the fractional reabsorption of water demanded by the overall evolution of the kidney and the water stringencies imposed over evolutionary time by the environment, the higher must be fractional reabsorption of crystallizing materials. For oxalate, which is secreted, plasma level and secretion must reach a homologous kind of equilibrium.
Where Things Are
I cannot speak about how kidneys work unless you have some idea of where things are – the parts and pieces out of which evolution fettled the amazing complexity of this organ. Although filtration is our present topic, it is part of the whole nephron that I sketch out here by way of orientation.
Parts of Kidneys
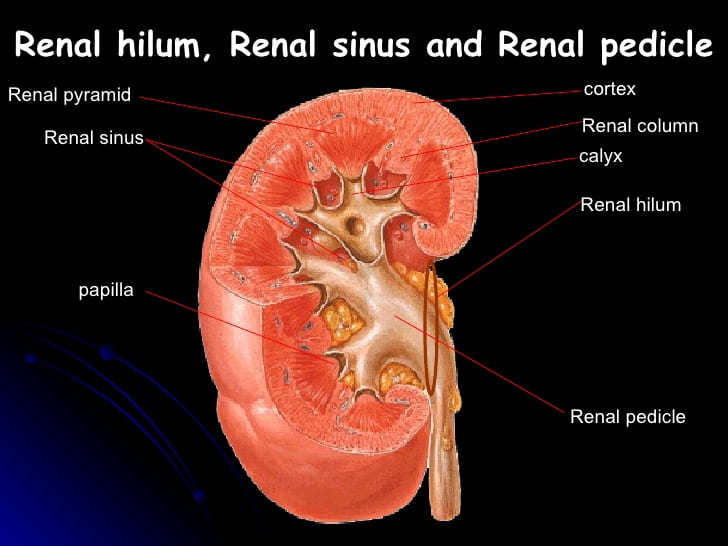
This cutaway drawing gives us what we need in common.
The thick cortex, like the rind of an orange, covers over the organ. Inside lie the pyramids that narrow down to their pale tips – the papilla. The collecting system looks like what it is – funnels that collect from the papillary tips and join together to form the renal pelvis (called pedicle here). That large pelvis drains through the ureter. Where the funnels cover over the papilla they form a flower like shape for which they are named calyx or calyces, the sepals of a flower.
The renal columns are just extensions of the cortex that wrap around the pyramids. If the picture makes you think that a whole kidney is made of individual units each with its pyramid wrapped in cortex and drained by its calyx, keep that thought. You are right.
Where Stones Form
Stones form right at the papillary tips, and so are inside the calyces. When they break off, they simply move through their calyx into the large pelvis and then into the muscular and more narrow ureter where they commonly obstruct and cause the miseries for which stones have become famous over long stretches of historical time. Stones can obstruct the channel from the papillary tip to the pelvis and cause pain and internal obstruction of one renal unit.
What Makes the Cortex and Pyramids
Here is one pyramid with its overlying cortex. Just as a kidney is made up of its pyramid / cortex units, each units is made up of individual nephrons. They run from the cortex down to the papilla, and their functions create stones.
Glomeruli
The arcuate arteries and veins separate the cortex from the medulla. They give rise to upward directed (interlobular) arteries whose blood supplies the glomerular filters.
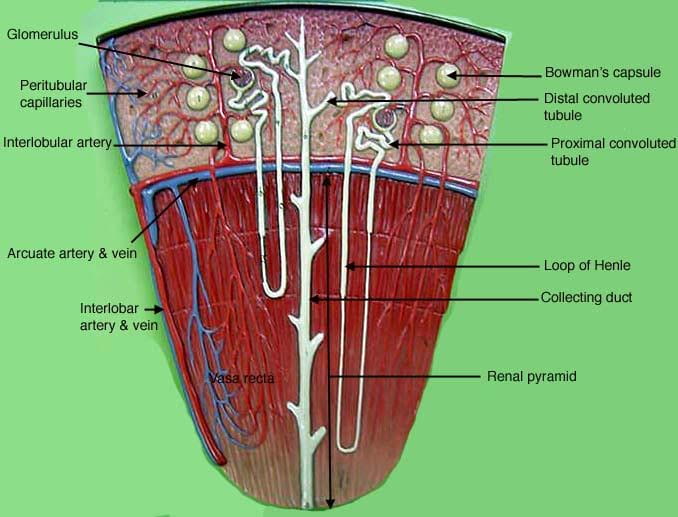
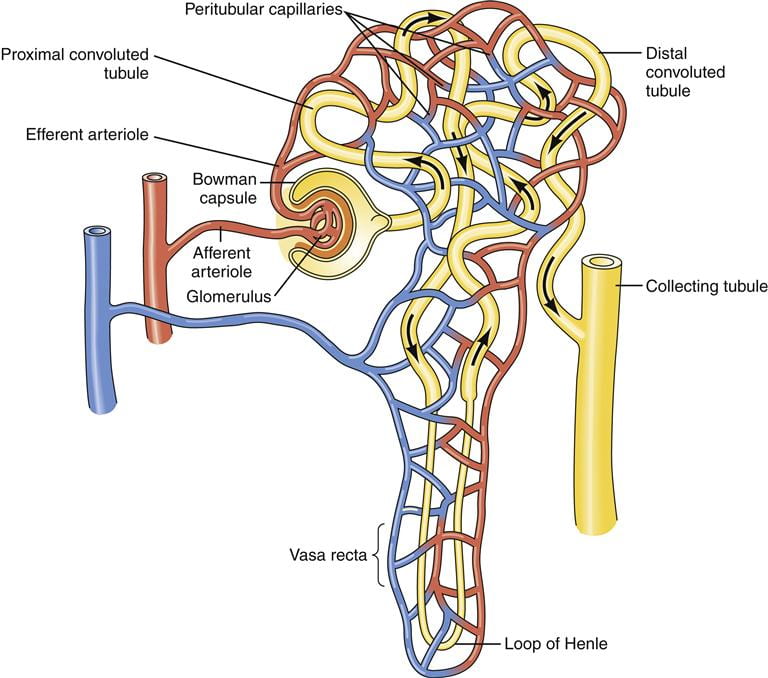
The orange rind cortex contains the glomerular filters shown here as balls. They lie, like oranges on their tree, upon upright ‘interlobular’ arteries whose side branches feed each one its supply of arterial blood. These side branches, the afferent or inward directed arterioles, feed a capillary tuft inside each glomerulus. Through the thin walls of these capillaries, pressure from the work of the heart filters water, salts, and small organic molecules out of the blood.
The blood leaves the capillaries in the efferent (outward directed) arteriole, and that blood bathes the tubules of the nephrons to sustain their lives. To do this, the vessel divides into a network of thin walled capillaries to serve the cells, and these gather back into small veins that coalesce like streams to form interlobular veins that drain into the arcuate veins.
Two cutaways show the capillaries within round cups that each drain the filtrate into the tubule the glomerulus belongs to. The tubules then process this filtrate into the final urine. Each adult human kidney contains about one million nephrons, each with its own glomerular filter.
Proximal Tubules
The earliest part is called the proximal – near to – segment, and, being convoluted has the name ‘proximal convoluted tubule’. It continues like a complex road into a straight portion often called the straight segment or, confusingly at first, the S3 segment. The S1 and S2 segments make up the convolution and are distinguished by molecular details.
Loops of Henle
Cortical Nephrons
The leftmost glomerulus hangs higher up on its tree. Its straight segment goes down part way into the medulla then gives way to a short thin segment called the thin descending limb of Henle’s loop -Henle first described it. After executing a hairpin turn, the tubule runs back up as the thick ascending limb (of Henle’s loop) that lives partly in the medulla and partly in the cortex.
Juxtamedullary Nephrons
The right handed cutaway shows a glomerulus quite near to the junction of cortex and medulla. Its S3 segment descends into the medulla exactly as the cortical nephron did. You can see that they match. But its thin limb descends far down into the medulla, almost to the papilla. Therefore its ascending thin segment is also very long. Its thick ascending limb has most of its length in medulla, only a portion in the cortex. Obviously it is only these nephrons whose thin loops reach to where stones form.
Thick Ascending and Distal Convoluted Tubules
This thick ascending limb rises into the cortex and finds the afferent and efferent arterioles of its own glomerulus – you can see this in the illustrations of the cutaway glomerulae. This junction point of immense regulatory importance – the juxtaglomerular apparatus (JGA) – gives way to the so called distal convoluted tubule – distal meaning away. That terminates in the long stalk of the cortical collecting duct. The cortical collecting duct rides down through the whole medulla to terminate at the opening of the renal system at the tip of the papilla.
Collecting Ducts and Ducts of Bellini
Of course the drawing simplifies things a lot. Each nephron has its own cortical collecting duct portion and these coalesce into larger and larger funnels like rivulets form streams. At the papillary tips, the openings through which urine flows out number perhaps 20 or so, which means that many terminal ducts – of Bellini. Given about 10 papillae, a kidney of one million nephrons drains via 20 x 10 or 200 or so Bellini ducts (BD), or 5000 nephrons per duct.
So kidney stones, our objects of intent, form at an ultimate strategic location – on the papilla tips just where the BD drain the final urine out into the collecting system. In the papilla we can find only the collecting ducts, BD, and thin loops from the juxtamedullary nephrons. And, of course, the blood vessels that permit these cells to stay alive.
Medullary Vessels
 I have already said that the tubules in the cortex get their blood from capillaries fed by the efferent arterioles. The medullary tubules are arranged in strong vertical arrays, and their capillaries are fed by the straight inward directed vasa recta. These branch off the efferent arterioles of the juxtamedullary glomerulae.
I have already said that the tubules in the cortex get their blood from capillaries fed by the efferent arterioles. The medullary tubules are arranged in strong vertical arrays, and their capillaries are fed by the straight inward directed vasa recta. These branch off the efferent arterioles of the juxtamedullary glomerulae.
In other words those glomerulae nearest the medulla service the blood supply of the medulla through their efferent arterioles. The descending vasa racta are therefore arteriolar – tiny terminal portions of the arterial tree. They feed the capillary network in the medulla and papilla. The capillaries gather themselves together into the ascending vasa recta – veins, not arterioles, and these drain back into the arcuate veins.
Here in this picture, a glomerulus near the medulla gives off its efferent arteriole. Some of its branches feed the capillaries in the cortex around its tubules. A main twig drives down into the medulla as the descending vasa racta. All along its length it gives off tiny feeders to the medullary capillaries that gather together again to form the venous ascending vasa recta.
Of enormous importance, the capillaries lie near and surround the thin limbs of the loop of Henle. This will matter in forming a concentrated urine that is so essential for creation of kidney stones.
Glomerular Structure
 Here is beginning, the glomerulus, where all things start.
Here is beginning, the glomerulus, where all things start.
The Vessels
Lets look again at this mighty life sustaining structure. Each kidney has about one million of them, each the head of its own nephron. The afferent arteriole is drawn with thick bands of smooth muscle around it, as these regulate the flow and pressure let into the capillaries. The efferent is drawn thinner, but it, too, can contract to create back pressure in the capillaries.
JGA
Where the thick ascending limb rejoins its own glomerulus special cells form making a triangular wedge bordered by the two arterioles and the cells of the limb. This whole region is the juxtaglomerular apparatus (JGA). We need to leave this wonderful device for another time.
Capillaries
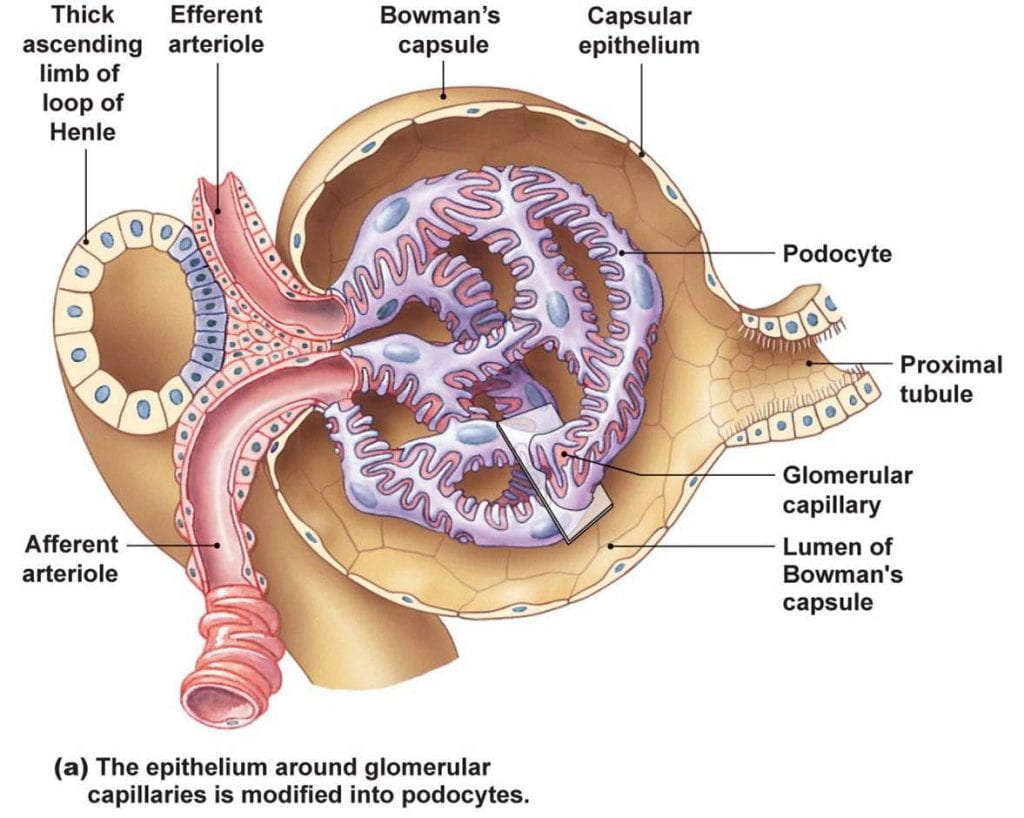
Their chamber’s (Bowman’s Capsule) walls invest the capillaries as if they grew into – invaginated into – what was originally a round ball opening into the proximal tubule. Imagine that you pushed your finger into the side of a partly filled balloon. The rubber surrounds your finger but your finger is outside the balloon.
Here, instead, the very walls give way to form a single layer of cells – podocytes – so fluid filtered through the capillary walls can get between the cells into Bowman’s capsule and thence into the bore of the proximal tubule. As if built by a magician the outer walls of the capsule gradually alter to become the lining cells of the proximal tubule. How this happens does look like a magic trick. Here is a nice YouTube with music and a great vision of how it happens. Here is a more serious but sketchy version.
In between the loops of capillaries lie cells not shown here. Called the mesangial cells they tether the loops together. They can contract, and as they do so they squeeze the loops reducing their surface for filtration. Where these cells contact the capillaries filtration cannot occur, so filtrate does not go into the mesangial space but into Bowman’s capsule and from there into the proximal tubule.
Let’s Turn Filtration On
I have shown you the magnificent and powerful looking glomerulus. Lets open up the valves, turn on the heart, and see how it works.
The Pressures
This sample of the many graphs one can find on the net and in books shows the main forces that affect filtration. I chose it because it illustrates a common tissue capillary (left panel) and a glomerular cappilary (right panel). All measurements are from animals – rats, dogs, etc. One cannot measure glomerular pressures in humans.
Bowman’s Space
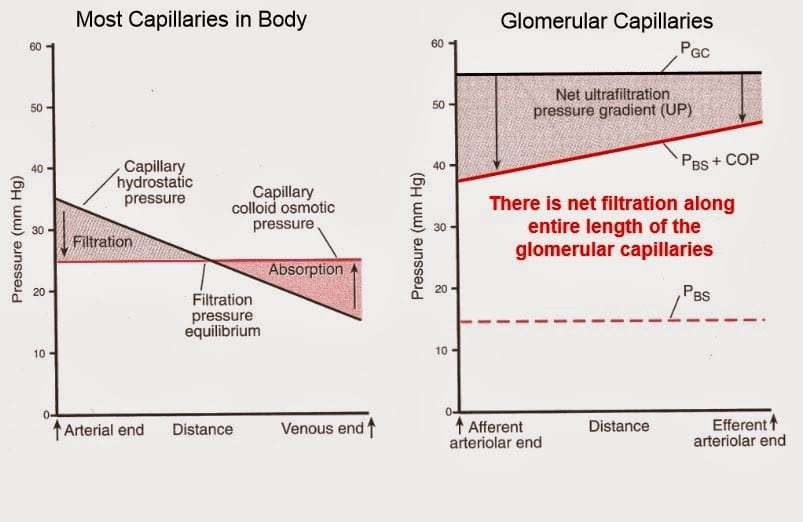
As filtrate accumulates in Bowman’s space (right panel) pressure rises to force fluid into the proximal tubule and all the way through the whole length of the nephron. Remember, only the force from filtration moves the fluid along. This back pressure, which reflects the work of forcing filtrate through the nephron, bucks out the net filtration pressure because it is outside the capillary.
Capillary Hydraulic Pressure
Pressure inside the cappilary, P(GC), is about 55 mmHg. Losses along the capillary are so small one can more or less draw them as constant. Remember, the pressure inside is the result of the pressure coming in from the afferent arteriole and the back resistance from the efferent arteriole. So the balance between the two arterioles can actively control the pressure inside the capillary. Because the pressure inside the Bowman’s space, P(BS), is about 15 mmHg, the net pressure across the capillary for filtration would be 55 – 15 or 40 mmHg.
Capillary Osmotic Pressure
The system has no air in it, so filtration is from the blood in the capillaries out into the filtrate that remains in contact with and wets the outside of the capillaries. The capillaries retain the blood albumin and other large molecules. These molecules exert a force on water so that water will be drawn inward from the filtrate – that is essentially protein free – back into the blood. That ‘oncotic’ or osmotic force from large molecules counters the hydraulic force. As filtration progresses, the concentration of the large molecules increases, so the capillary osmotic pressure, (COP), rises.
Net Filtration Pressure
The pressure differential across the capillary and podocytes drives filtration. Obviously this is the capillary hydraulic pressure minus the sum of P(OC) + P(BS). At the inflow it is about 55 – 38 or 17 mmHg. At the end of this highly stylized drawing it is about 55 – 44 or 11 mmHg.
One can easily understand that flow will matter a lot. If flow goes down and pressures remain the same, P(OC) will rise more rapidly because initial filtration is the same as at higher flows but filtration is from a smaller flowing volume. This can reduce the area between P(GC) and P(BS) + P(OC) even to the point that filtration ceases before the end of the capillary. Contrariwise, if flows go up filtration will go up for the same reasons – P(OC) will rise more slowly.
Systemic Common Capillaries
Filtration equilibrium, a point of no net filtration, is the rule for capillaries apart from the glomerulus.
Look at the left hand panel of the figure. Throughout the body, fluid leaves capillaries into the tissues and then, as one moves along the capillary length P(OC) rises enough that filtration gives place to reabsorption. This washes the space around capillaries by day and by night so nutrients flow outward to cells and their waste produces sweep up into the capillaries that bear them eway to the lungs and kidneys and liver where they leave the body or change their chemical natures.
So glomerulae are merely specialized versions of the common capillary. They work at higher pressures. They have valves to control their inlets and outlets, their walls are supported by podocytes. Their loops are tethered by mesangial cells. And their filtrate does not go back into the blood but into the tubules that regulate exactly what will go back and what go forward out of the body.
Let’s Regulate Filtration
Afferent Arteriole – Rex regum
As I consider all of the regulating powers for filtration, this one locus seems to be most powerful of all. So I say it is, although disputes with peers about such a generalization can become endless, and even disagreeable.
It Adapts to Keep Flow Constant
Like all arterioles, but better, the AA dilates when pressure falls reducing tension in its walls. Likewise when pressure rises it contracts. This so called ‘intrinsic autoregulation’ keeps glomerular capillary flow and pressure more or less constant over a range of pressures and flows delivered to the kidneys by the heart.
 It Makes A Powerful Hormone
It Makes A Powerful Hormone
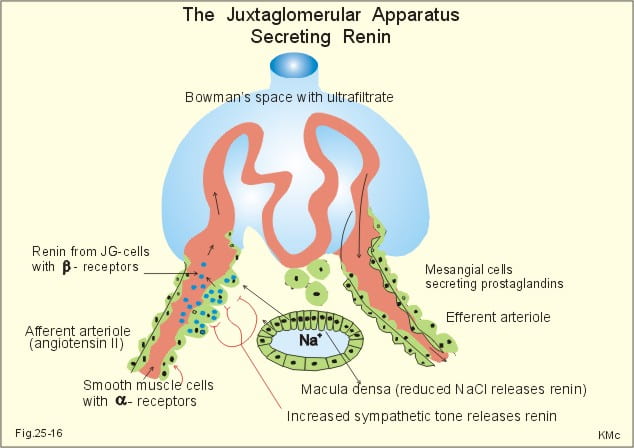
The AA cells produce renin, an enzyme that cleaves a prohormone, angiotensin 1, to its active form, so called angiotensin 2 (A2). This active hormone, A2, signals the efferent arteriole to constrict, but does not affect the AA. More: the AA releases renin when it dilates because of falling flows and pressures – when its wall tension goes down.
This simple stock illustration sketches out the main features. Some smooth muscles of the AA – juxtaglomerular cells – produce and store renin in granules that they can release when they dilate. The A2 travels to the efferent arteriole that has receptors and can respond to A2 by contracting.
The diagram has the A2 flowing from the afferent to the efferent arteriole but that is probably not the case. The real story is too big for now, so let’s just say it gets there.
Sympathetic nerve traffic and catecholamines released as part of stress reactions also cause renin release but constrict the AA. The renin release helps maintain filtration despite AA constriction. (To my colleagues: Just a bit later on I reference the modern version of all this that I postpone at this point as too complex and detailed for general readers.)
Tubulo-glomerular feedback
Finally, remember how the thick ascending limb comes back to its glomerulus to form the JGA? When less sodium chloride gets to that part of the nephron – downstream delivery goes down – the cells stimulate renin release so that EA constriction can raise filtration.
It Keeps Filtration Constant Under Stress
The final result is a dual regulation. When renal inflow falls, the AA dilates and via renin and A2 constrict the EA. This latter keeps the pressure up in the capillary. So by its own intrinsic autoregulation and by its control of local (inside the glomerulus) A2 production, the AA can keep filtration reasonably constant over quite a range of systemic blood pressures and cardiac outputs of blood.
Likewise it transponds stress reactions with sympathetic activity – flight or fight – into EA constriction so filtration can stay constant even as AA constrict. Finally it permits so called tubulo-glomerular feedback from the JGA so a fall in downstream sodium chloride delivery can trigger off more filtration.
Stone Obstruction
One such stress is obstruction from a stone. In another article Mike Borofsky and I detail what happens to filtration pressures and GFR as a stone obstructs the kidney. Regulation mechanisms for filtration all come into play, and one might want to re-read that article after this one.
This is a Very Simplified Overview
The real sources and regulation of A2, how it works in the kidneys, where it is made in the kidneys, how it can get into the circulation, all that, is a massive story. Likewise the mechanisms of filtration itself and tubuloglomerular feedback.
For fairness to the more ambitious or technically trained, here are some reasonable introductions to where things are. My favorite reviews are by mathematical modelers. I call them meta analysts with brains. They pull together what pathways are thought to work along with lists of the key transfer constants, model them with correct mathematics, and see if things match to reality.
Here are two about angiotensin 2: Part One Part two
Here is a brilliant author on filtration itself: Modeling glomerular filtration.
For relaxation: A lovely pictorial review running at a distinctly lower voltage but with terrific diagrams.
For the more pensive moments: A rather old fluent review going back to antiquity authored by one of the great figures in renal physiology.
How To Measure Glomerular Filtration
Creatinine – An Imperfect Universal Marker
There is a chemical called creatinine that muscles make in their normal course of being. Like almost all small molecules, kidneys filter it. In the diagram, I have simplified the magnificence of the glomerulus to a mere red tube. Blood flows in at Qi and leaves at a lower flow Qo. The difference (Qf) is glomerular filtration rate (GFR) – rate because we are speaking about amounts per unit time.
The long cylinder at right angles to the red glomerulus is the whole nephron. I show urine leaving at the bottom and filtrate coming in at the top. I have reduced the kidneys to two tubes for this present purpose.
The picture promises a link to an excellent review – here is the link. It is none other than the wonderful historical review from before.
The Arithmetic of GFR
Creatinine Clearance
Creatinine must enter the nephron at a rate of GFR x Pcr, where Pcr is the plasma creatinine concentration (amount per volume) and GFR is volume per time. Nothing else can be.
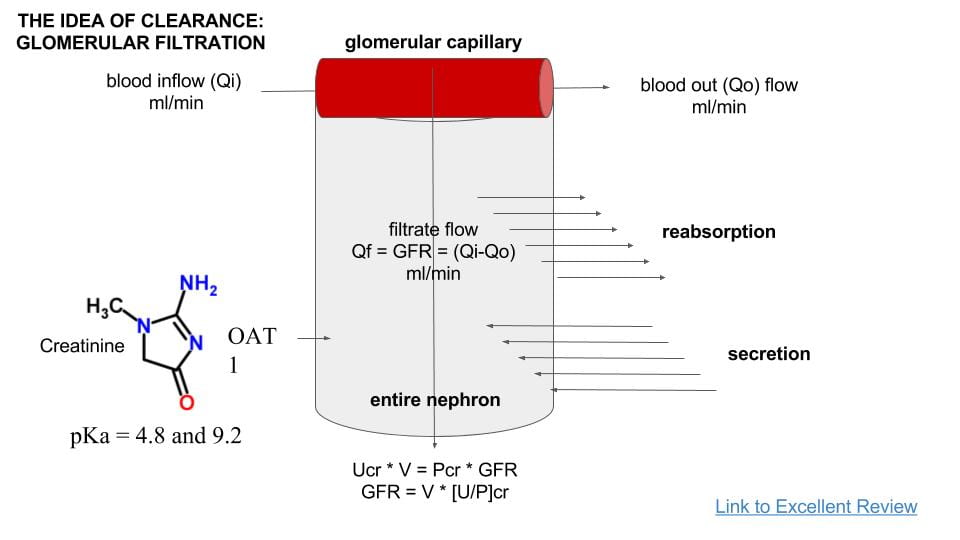
I show the tubules as able to reabsorb materials from the filtrate, or secrete materials from blood into the flowing filtrate. This is how the nephron transforms filtrate into the final urine. For creatinine, reabsorption is null – does not occur. It is secreted, however, by a transporter named organic acid transporter 1 (OAT 1) but that amount is relatively small compared to filtration in normal people. Because it is small, we neglect it and say that the total amount of creatinine leaving in the final urine is simply GFR x PCr – in other words precisely the amount that entered at the top by filtration leaves at the bottom in the urine.
If we call UCr the urine concentration of creatinine (amount per volume), and V the urine flow rate (volume per time), the amount (amount per time) leaving is UCr x V. That must equal GFR x PCr. To get GFR we simply rearrange: GFR = UCr x V/PCr – the rate of urine loss divided by the plasma concentration. Because secretion deviates this calculated value from true GFR, we should call it something else. That else is best named creatinine clearance, or CCr.
True GFR – Inulin Clearance
Inulin is a large carbohydrate polymer that lacks the one defect of creatinine. After filtration the nephron cells neither reabsorb it back into the blood nor secrete it from blood into the tubule fluid. It passes as through a glass tube. So the clearance of inulin is GFR.
 Given this perfect marker, how bad a marker is creatinine?
Given this perfect marker, how bad a marker is creatinine?
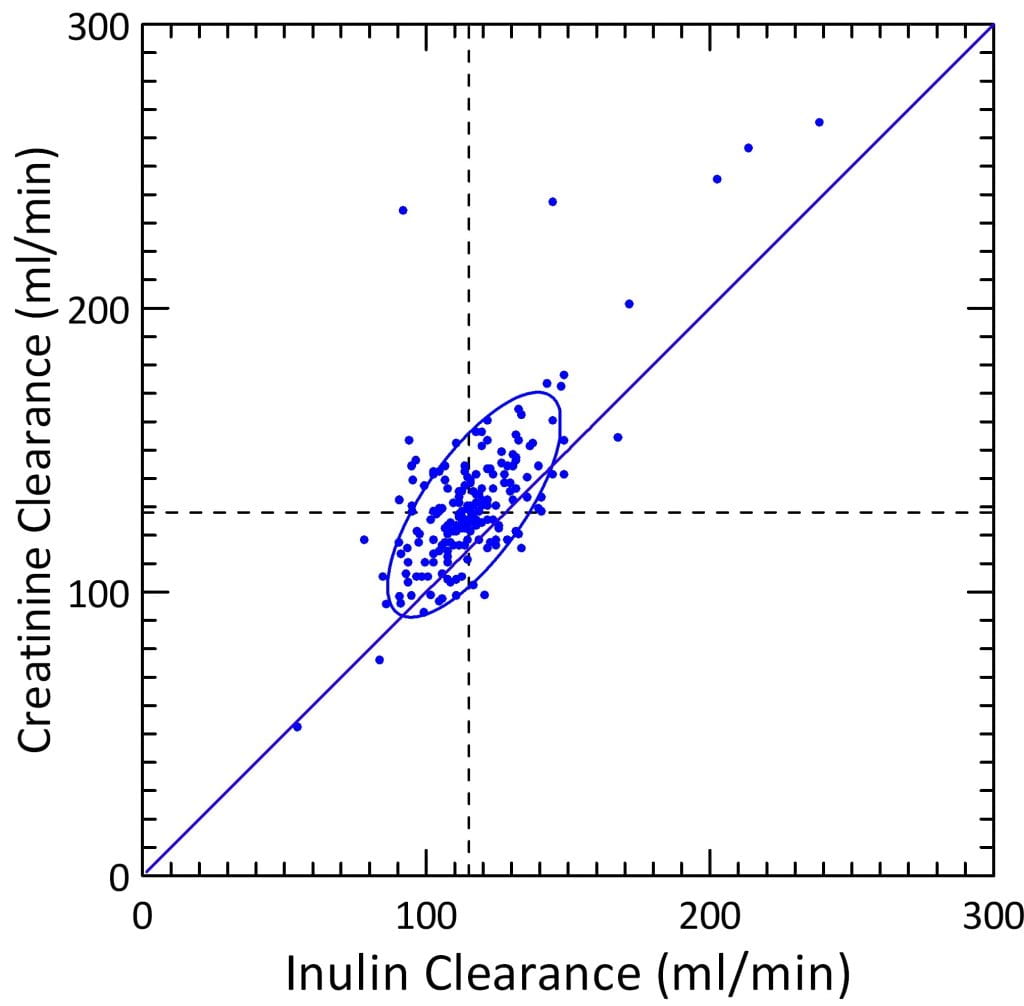
Jacob Lemann, a great scientist and a close friend, left behind at his death the lab books of his experiments. We had the good fortune to get copies made, page by page. From these we copied out multiple instances where he measured both inulin and creatinine clearances. I made this graph to compare them.
First, take a look at the axes. GFR values are in hundreds of ml/min. Five ml fill a teaspoon, 15 ml fill a tablespoon, 30 ml is a shot of whiskey. The two kidneys can filter a lot out of blood every minute, enough to fill 3 – 4 shot glasses, or more.
The diagonal line marks a one to one correspondence. Most of the points lie above it. This reflects the secretion of creatinine by OAT-1. CCr overestimates GFR. But CCr moves in parallel with the true GFR and therefore is useful.
The dashed reference lines lie at the medians for inulin and creatinine clearance (112 and 128 ml/min). As an estimate, therefore, CCr overestimates CIn by about 128/112 or 11%. That overestimate from secretion is clearly due to a constant secretion acting as the intercept of the linear regression of CCr on Cin.
Quantitatively, the regression coefficient for CCr on CIn is 0.882, the intercept 26.8 (ml/min). But the adjusted squared multiple R is only 0.565 because of variability, so these are approximate estimates.
Serum Creatinine
CCr is the urine creatinine loss divided by the serum creatinine concentration: CCr = Ucr x V/Pcr. Therefore, by simple rearrangement: pCr = UCr x V/CCr. So serum creatinine varies upward as GFR (estimated by CCr) falls.
Practically, physicians order only serum creatinine to measure kidney function – imperfect indeed. A timed urine collection would be expensive and cumbersome. Because the amount of creatinine lost in the urine varies with muscle mass – muscle makes it -, serum creatinine and CCr may vary together but only with a lot of scatter from variation of urine creatinine.
Secretion also varies from person to person. Look back at the graph above. Many points fall right along the line of identity. The one far off to the right is no doubt an error.
But despite these variabilities, in any one patient physicians have long used a mathematical trick to track changes in kidney function. Because CCr = (1/PCr) x UCr x V – the inverse of SCr times the urine creatinine excretion – if you plot 1/SCr against time, you get a reasonable sense of how things are going. Urine creatinine excretion in any one person is likely to stay reasonably constant over time.
eGFR
To get a better estimate, serum creatinine was compared to true clearances in reasonably large populations and the best fit calculated using regression techniques. This gives estimated GFR, or eGFR. This highly derived index presently dominates medical practice, so in real life when physicians speak of reduced kidney function they mean reduced eGFR.
The most widely used equation is this one:
eGFR = 141 × min (Scr /κ, 1)α × max(Scr /κ, 1)-1.209 × 0.993Age × 1.018 [if female] × 1.159 [if black]
Scr is serum creatinine in mg/dL,
κ is 0.7 for females and 0.9 for males (these are the mean serum creatinine values by sex),
α is -0.329 for females and -0.411 for males,
min indicates the minimum of Scr /κ or 1, and
max indicates the maximum of Scr /κ or 1.
Called the CKD – EPI equation, this calculation drives present day laboratory reporting and medical practice. Here is an official statement about the use of this estimating equation.
Note the terms min (Scr /κ, 1)α × max(Scr /κ, 1)-1.209 mean serum creatinine is inverted (1/serum creatinine with some arithmetic clutter). Anything exponentiated to a minus means it is inverted (α is negative). This inversion reflects the primal fact that GFR =(1/SCr) x UCr x V. It means this fancy equation is nothing more than an elaboration of very ancient practice of tracking kidney function by plotting 1/PCr against time.
Why Do We Care?
Stones may injure kidneys as they obstruct. Surgery may injure kidneys. Kidneys can be lost. So kidney stone patients can lose kidney function. Estimating equations are a clue. If coupled with blood, the 24 hour kidney stone testing will show true creatinine clearance. But that, though in one way more exact than CKD – EPI, overestimates true GFR in another – creatinine secretion. Most of the time all of the measures will coincide well enough for routine care. Definitive measurements like inulin clearance are not clinically feasible.
Low Sodium Diet
Low sodium diet is a main feature of kidney stone prevention because it lowers urine calcium. So how does filtration behave when diet sodium goes down?
Blood Volume will Fall
I showed you elsewhere that if diet sodium goes down kidney losses continue at the higher level for several days. As a result some sodium is lost from the body. Almost all of that loss is from the fluid outside the cells, and normal cell function requires that sodium concentration stays constant at 140 mEq/l. Therefore, loss of sodium is loss of fluid. We all know we lose weight if we cut down our salt intake.
Less fluid volume includes less blood volume, so the volume pumped by the heart will go down. Blood pressure tends to go down, as well. This should lower GFR.
Renal Vessels Compensate
 The afferent arterioles can sense the reduced wall tension, and will release renin, so A2 increases and the EA constricts. Flow through the AA will fall as blood flow and pressures fall in the renal arteries, but the fall is somewhat mitigated because the AA will dilate as part of its intrinsic autoregulation. As a result, filtration will remain higher than it would otherwise have been.
The afferent arterioles can sense the reduced wall tension, and will release renin, so A2 increases and the EA constricts. Flow through the AA will fall as blood flow and pressures fall in the renal arteries, but the fall is somewhat mitigated because the AA will dilate as part of its intrinsic autoregulation. As a result, filtration will remain higher than it would otherwise have been.
Any fall in GFR will reduce sodium chloride delivery to the JGA. This will in turn increase signalling to increase renin and therefore A1 release so the EA will constrict more so as to maintain glomerular capillary pressure and GFR.
But the overall effect is to constrict blood flow and one might imagine glomerular filtration will tend to fall.
Filtration Rate Falls
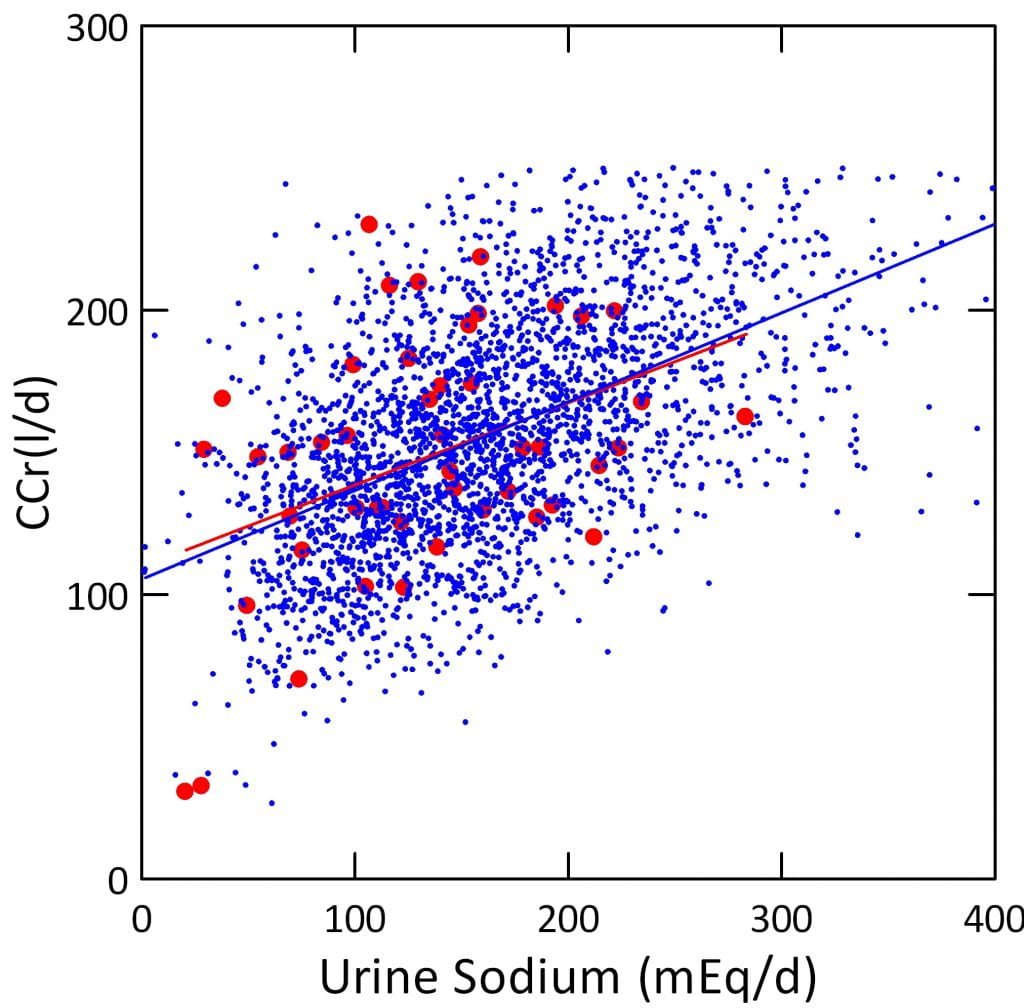
Here are data from large numbers of stone formers – blue, and normal people – red. As the 24 hour urine sodium falls, a good measure of diet sodium intake, CCr falls. The scatter around the regression lines dramatizes the complexity and variability of the system.
Alas, the graph includes potential confounders. Big people eat more of everything, and filter more, too. Men and women may differ. This could exaggerate the correlation. Perhaps, even, produce it as a mere artefact.
But if I use simple multivariable regression analysis to account for the effects of weight – very large – and sex, very tiny, sodium remains a powerful correlate of CCr. For every 100 mEq/d of urine sodium change, CCr will change by 20.2 l/d.
Because low sodium diet lowers filtration through normal regulating systems it causes no harm. Kidneys are designed to regulate filtration in response to such variables as diet sodium intake. This means, for example, that a rise in serum creatinine or fall in eGFR with low sodium intake need to not alarm physicians or patients. However, I should mention that in patients with significant kidney disease, or those with other systemic diseases, low sodium diet requires careful medical monitoring.
Filtration Fraction Rises
Apart from its absolute value, filtration will differ intrinsically from that with high sodium diet. With low diet sodium, a higher fraction of capillary hydraulic pressures arises from outflow vessel constriction that offsets a lower blood flow. So the fraction of the blood flowing though that is filtered will go up. Put another way, filtration is higher for the blood flow. The result is an increase in the protein concentration of the blood leaving in the efferent arteriole.
Later on, when we connect the glomerulus to its tubule, that difference will matter.
Fall in eGFR or CCr with Low Sodium Diet is Usually Harmless
I said this already, but need to repeat myself.
Because physicians often measure serum creatinine as part of common test panels, and because laboratories present eGFR by law, your physician may tell you your kidney function has fallen when you have significantly lowered your salt intake. Of course, it may have fallen for other reasons. So remember this: When you lower diet sodium intake appreciably always get a new 24 hour urine to show the change in urine sodium – which reflects your diet intake – and get it with a fasting blood sample. One expects a fall in CCr of about 20 l/day (~15 ml/minute) for every 100 mEq/day fall in urine sodium. A larger fall, or a fall sans a lower urine sodium, may reflect some other reason for it such as obstruction. So caution is always required.
Creatinine Values in Stone Formers
We have long measured serum creatinine and 24 hour creatinine clearances in stone formers. Along the way we measured it in normal people who happened by.
The Kind of Plotting
The plot here is called a p-plot. The measured values run along the horizontal axis. They are plotted against the normal distribution function on the vertical axis. That function describes random and independent measurements. The plot centers the mean at 0 along the y axis, and shows all points above and below the mean in units of standard deviation (SD). Because 1 SD includes about 68% of points and 2 about 95%, you can label any one point in terms of its being central or uncommon.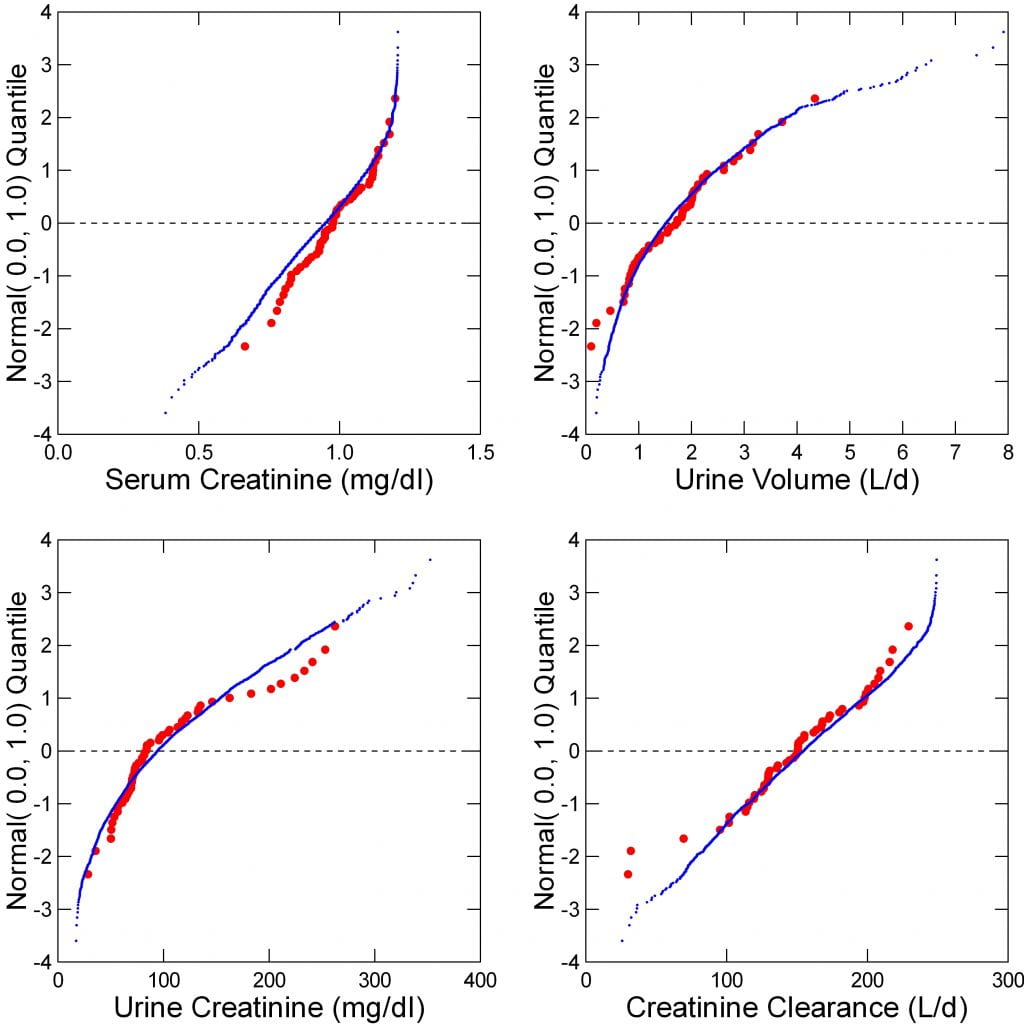
A straight line means the data indeed follow the normal curve. A curved line means they do not. Each line (patients blue) is made of individual points that are so numerous they appear as a solid line. Red points – normals – are bigger because fewer.
Components of Creatinine Clearance
Serum Creatinine
The graph is straight part way, meaning the values are sort of normally distributed. I plotted men and women together. Remember that normal means for women and men are 0.7 and 0.9. Look for your values, and see where you fit. Note the a right hand tail of values above the mean; these may be either people with large amounts of muscle – high creatinine production – or reduced kidney function.
Urine Volume
Highly curved, this is no normal distribution. Notice how normals and patients are much the same. You know your 24 hour volumes from your kidney stone 24 hour tests. See where you fit. The mean – at 0 – is just below 2 liters/day. Stone risk begins below 2 liters/day.
Urine Creatinine Concentration
Urine creatinine concentration shows how much water kidneys have extracted from the filtrate. Look at the two horizontal axes for serum and urine – one graph is placed above the other. Both show mg/dl, or mg per 100 ml of serum or urine. Serum is about 0.5 to 1.5 mg/dl, urine about 25 to 300 mg/dl. Do you need a more dramatic glimpse of how kidneys make stones? To raise the creatinine concentration from 1 to 90 mg/dl means to leave behind only 1/90 or 1.11 percent of the water. That is what kidneys do. And in doing it, they can supersaturate urine greatly.
Creatinine Clearance
A near perfect straight line. Biological traits, like height, are that way. However crooked the components, the final kidney function is normally distributed. It ranges from 50 to 250 liters/day (35 to 177 ml/min).
What do those numbers mean? The creatinine in the urine had to come from that many liters of filtrate to make up what is in the urine. If you neglect secretion for a moment, it means kidneys pour that much filtrate into the proximal tubules of their nephrons every day. The urine volume is about 2 liters on average, the filtration about 150 liters, so of the 150 liters 2 remain, or 1.33%.
Look at your own values from your 24 hour tests.
Also, note the left hand tail of low values. Of course some are very small people, perhaps some children. But also, some are stone formers with kidney disease. All of these data are from our own patients. I have already pointed out that kidney stone formers can develop kidney disease, and that some of our own patients have done so. The low CCr values are indeed from those very people.
The Meaning Of GFR
Kidneys Clear From the Plasma
How much plasma do you have in your body?
I’ll tell you. About 3 liters. In fact, the average woman has less than that.
It is from these 3 liters that kidneys filter their 150 liters daily. So the 3 liters of plasma are filtered over and over again – 150/3 or 50 times a day. Of course, most filtrate is taken back, so the plasma volume stays constant. You might think the whole process is silly – filter it, and put it back in.
For the experts, here is a review of all plasma volume measurements up to 1995 – the latest I could find.
But ‘taken back’ is not simple. Some molecules are taken back only partly, some not at all. Some almost entirely. The kidney cells that line the nephron control this for each molecule. That selection of what is to go and what is to stay determines innumerable blood concentrations. It is the very quintessence of what it means to be a kidney.
Filtration itself is just about water, however, so what does it matter that 99% of filtered water is taken back? It is that the water is taken back but what was in that water and destined for removal was not equally taken back. To the extent that water is taken back and crystallizing salts are taken back less than enough, kidneys will make crystals.
In that simple phrase lies much of calcium stone formation.
The Mill Dam Again
Think about the pool behind the mill dam.
Into it pour waste runoff from the land – like waste products from metabolism. Suppose the pool is 3 liters, and 150 liters flow through it every day. Clear. Suppose the opposite, 150 liters of pool and the flow 3 liters per day. Stagnant, a mess. Thus do kidneys clear blood plasma of what needs to wash away. Rinsed through the magical filters of the nephron 50 times a day, plasma sparkles and shines in perfection and clarity of being, made new minute by minute that the cells of the body may bathe perpetually in their private, pristine, and elemental sea.
The ratio of the volume (3 liters of plasma) to the filtration of plasma (150 liters/day) has the units of liters/liters/day, or 1/day. So the average time to remove what may be coming in is 3/150 or 0.02 days. Days have 1440 minutes, so it is 28.8 minutes of average dwell time. Things that enter blood that need removal for health and are removed simply by filtration have an average dwell time of 28 minutes. Not bad.
At one half of that 150 l/d (75 l/d the dwell time for filtered and unreabsorbed materials is double or 56 minutes. That clearance, 53 ml/min in the conventional units, is called Stage 3 chronic kidney disease, but people with it are essentially well. At one quarter, or 37.5 l/d, conventional clearance is 26 ml/min. This is called stage 4 kidney disease and people are patently ill. Dwell time is twice again as long or 112 minutes. In fact, because CCr overestimates true GFR, actual dwell times are perhaps higher by the 20% or so of the overestimate.
Of course, materials like sodium, and calcium that are mostly reabsorbed and not lost in the urine dwell much longer. This helps to maintain very stable blood levels.
The Extracellular Fluid Volume
I can hear my colleagues – Wait, Wait! The total fluid outside cells, the extracellular volume is much more vast. Kidneys remove stuff from all of it!
Indeed. It – that whole vastness – is like the vastness that drains, silts, and runs into the mill pool, and the river, too. Likewise, I did not say dwell times concerned the hugeness of the extracellular fluid, either.
Of course not. Why should I.
It – the whose vastness – is the source bed for what comes into the blood plasma. But kidneys remove only from the blood plasma, our mill pool.
I know the cells bathe in the entire extracellular pool. That pool is their ‘private, pristine, and elemental sea’. But it remains so because what feeds it, and what it drains into, the plasma, sparkles like diamond, shines with a pure and perfect light.
Look back – I did not say where the ‘sea’ was – too hard all at once: ‘Success in circuit lies’.
The Link to Kidney Stones
I said at the beginning that high filtration helps produce kidney stones but never elaborated on the idea. Here is what I meant.
CCr is a Product of Two Terms
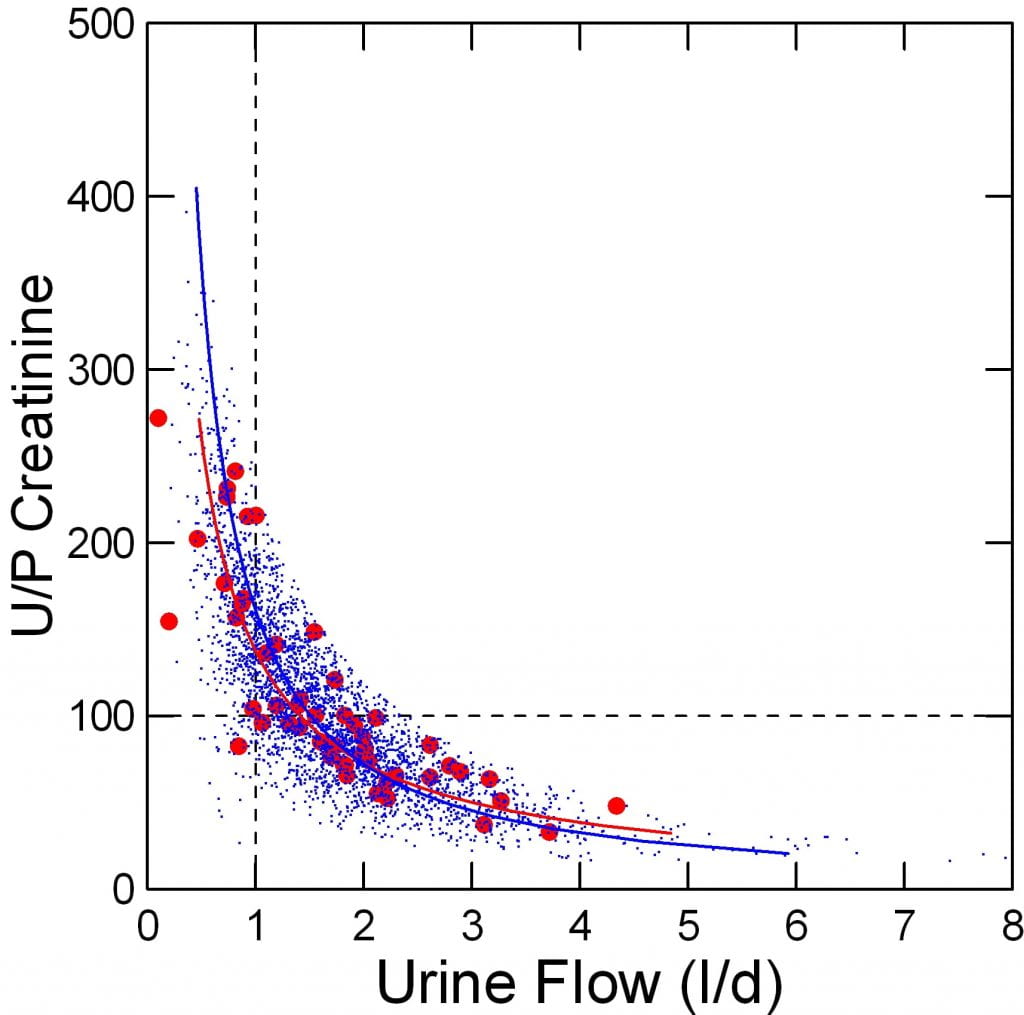
The clearance equation for creatinine – or anything else for that matter – is GFR = V x Ucr/PCr. This has two terms in it. Volume flow (V) and the ratio of creatinine in urine to that of blood. Take a look at the graph to the right. It plots that ratio against urine flow rate in liters/day.
The two terms of the clearance equation obviously move inversely to each other. As the volume flow (V) falls, the U/P ratio of creatinine (which has no units being the ratio of two concentrations) rises.
The vertical dashed line corresponding to one liter of urine per day crosses the curves that fit the normal and stone patient points at about 150 U/P ratio. So the average GFR at 1 liter per day of urine flow is 150 liters per day. That is the same as where the p plot for CCr crossed 0 – the mean value. Take a look back at the lower left hand p plot.
Also remember, these are not theoretical lines; the blue and red points are each a single blood and urine pair from a patient or normal. The tightness and resolution of the bands simply reflects the cohesion of the clearance function.
The U/P Creatinine Ratio Marks Water Reabsorption
Molecules Filtered and Not Reabsorbed
Because the U/P ratio gives the CCr at a urine volume of one liter per day, if your GFR is 75 l/d instead of 150 l/d, your U/P value at one liter is 75, not 150. The degree to which filtrate is concentrated at one liter per day is half, but all things being otherwise equal, urine concentrations of all substances filtered and not reabsorbed will be the same as at a U/P of 150.
This is because if only filtered, the plasma concentration will double as the GFR falls by half. But unless the supply of molecules falls or rises – metabolism, diet – the urine concentration at one liter must be unchanged to maintain excretion. The U/P ratio falls because the plasma concentration doubles.
Effects of Reabsorption
This is not what happens to things that matter to us, like calcium and citrate. After filtration, tubular cells reabsorb a very high fraction back into the blood. The reabsorption process – the mill dam – helps keeps plasma concentrations relatively constant despite changes in filtration.
With respect to urine excretion, if reabsorption stays the same as a fraction of what is filtered, the supersaturation at one liter per day of urine will be lower by half if GFR falls by half. That is because the the amount lost in the urine will be lower by half. Concentration can stay up only if the fraction reabsorbed goes down.
Conversely, at any GFR, even small changes in the fraction reabsorbed can change urine concentrations quite a lot because of leverage: the extreme concentration of the original filtrate as it turns into urine makes reabsorption crucial to prevent high urine concentrations.
Effects of Secretion
Because secreted and filtered, oxalate behaves differently from calcium and citrate. It is a potential toxin because it can combine with calcium in blood to form crystals that can damage tissues. Secretion keeps its plasma concentration very low yet maintain excretion to match GI uptake and metabolic production. Even so evolutionary pressures must have honed secretion to maintain excretion yet avoid unwanted crystallization in kidneys. Fitness depends on water conservation that does not damage either kidneys or internal organs. Organisms had to fit around the unalterable and prebiological laws oxalate crystallization follows.
Urine Calcium
Given all this, what actually happens to something really important to stone formation, like calcium?
 Urine Calcium Concentration Follows Water Extraction
Urine Calcium Concentration Follows Water Extraction
We expect the urine calcium concentration to parallel the U/P creatinine. The latter marks water extraction, so calcium will be concentrated.
It is, but with much scatter. The scatter must arise from variation in the amount of calcium reaching the final urine. That in turn reflects reabsorption and amount filtered.
Stone Formers Reabsorb Less Filtered Calcium
Because the red points from normals lie below the blue points for patients, you can tell immediately that patients reabsorb less filtered calcium than normal. Formal studies of this have proven it is correct, and due to idiopathic hypercalciuria.
The effect that falling GFR has upon urine calcium concentration and therefore stone risk therefore depends, in principle, on three things: Urine volume (thence the U/P ratio; calcium reabsorption after filtration back into the plasma; the GFR itself.
But this is theoretical. It is true that urine calcium loss actually depends on the level of GFR?
 Urine Calcium Excretion Falls with CCr
Urine Calcium Excretion Falls with CCr
Unadjusted Data
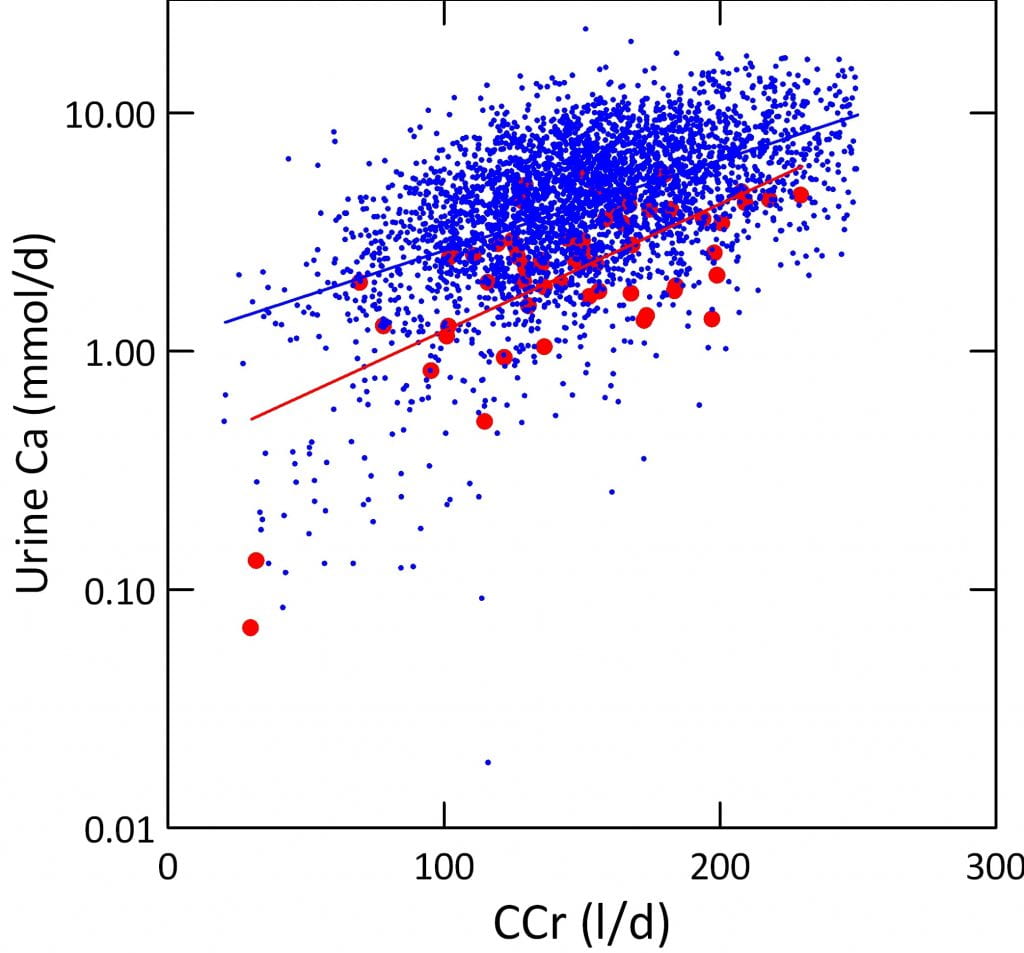
At least our observations using CCr certainly show it does. The right hand graph plots the urine calcium loss on the vertical axis against the CCr on the horizontal axis. Points from patients lie above those from normals, because of lower calcium reabsorption.
Urine calcium excretion and CCr correlate strongly.
Note the calcium axis is logged because it varies over 4 fold range from as low as 0.02 mmol/d to a high of over 10 mmol/d.
Adjusted for Sex and Weight
But, you may ask, is this graph perhaps misleading? Big people have higher CCr and also higher calcium intake and losses. Are we just looking at size? At sex?
No. In a simple general linear regression model, almost all of the effect on urine calcium is CCr. Body weight had a slight effect, as did sex. Adjustment for weight and sex together have almost no effect on the final result. For every 10 l/d ( change in CCr, urine calcium changes by 0.32 mmol.
What This Means
Given that stone risk varies powerfully with urine calcium excretion, a lower GFR that lowers calcium excretion must lower stone risk unless it led to a reduced urine flow rate. But I will show in other articles that urine flow rate is controlled separately from GFR to such an extent that no changes in GFR above levels of severe kidney failure have any effect on it. So even mild kidney disease may reduce calcium stone risk, and significant kidney disease may well abolish at least the calcium mediated component of risk.
Oxalate
Effects of Water Extraction
Being secreted from blood into tubule fluid oxalate concentration could stay very high even as GFR falls. I say this to make clear that calcium and oxalate are handled differently and that generalizations about effects of falling GFR may not always apply depending on the main problems causing stones.
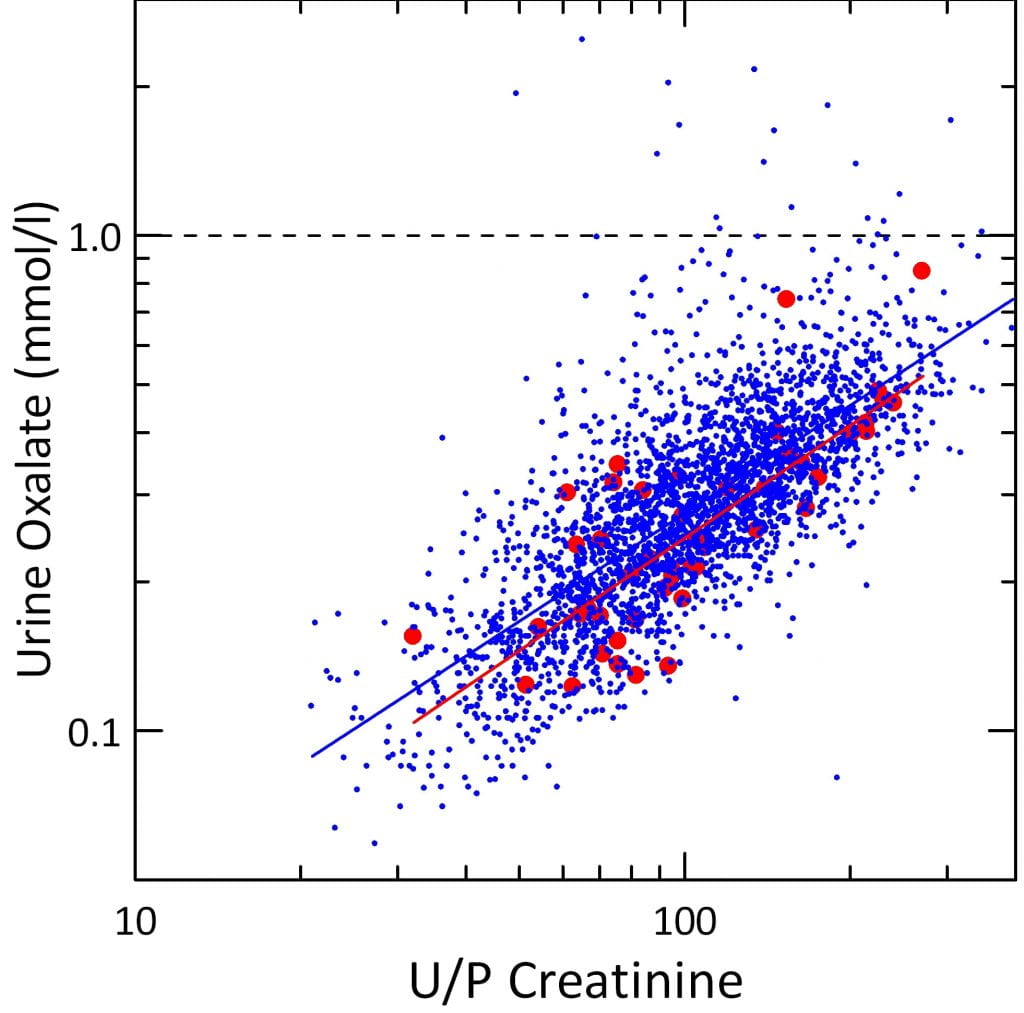
As expected urine oxalate concentration falls with falling U/P creatinine. The scatter about the regression is very tight and normals overlap with stone formers much unlike the higher values for calcium in stone formers.
The lesser scatter may reflect a more simple and regular control of oxalate secretion and reabsorption compared to the biologically more elaborate regulation of calcium. That is just my speculation.
 Effects of Falling CCr
Effects of Falling CCr
Unadjusted Data
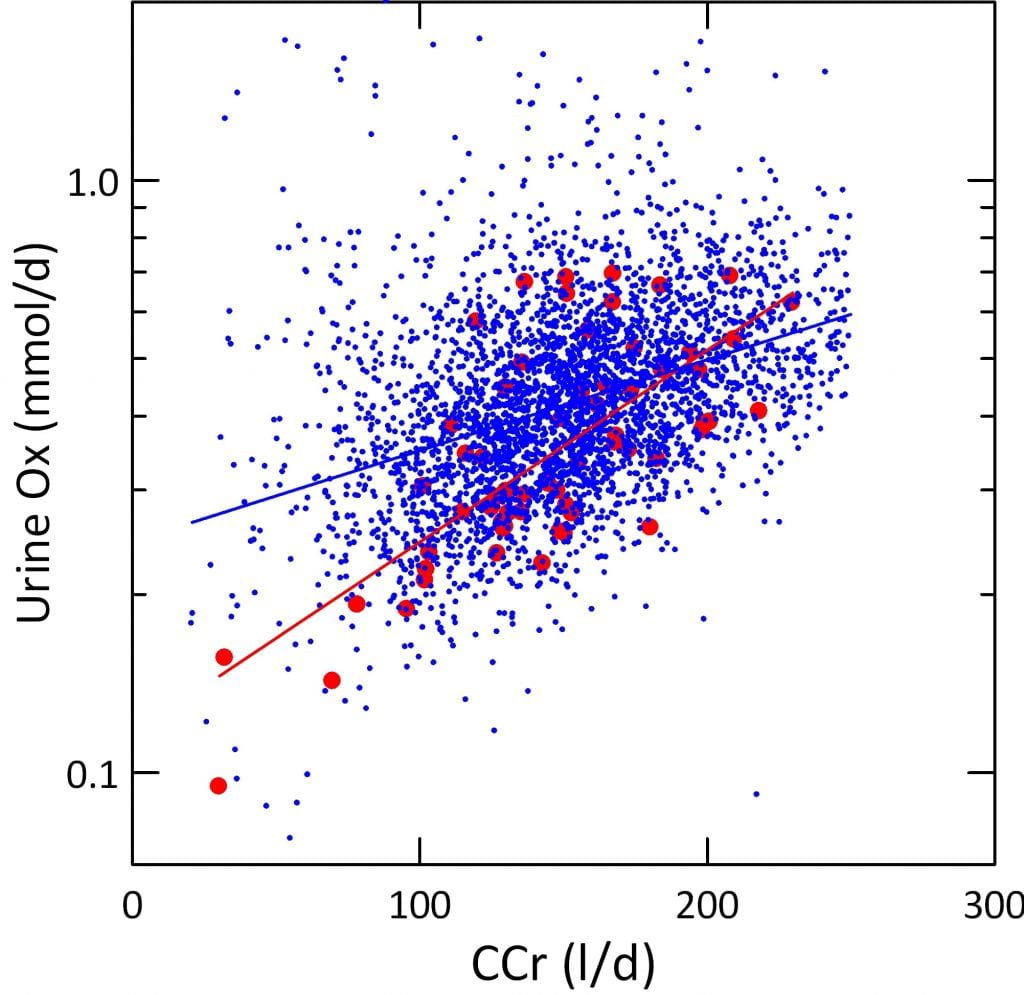
Because it is filtered, like calcium, one might expect oxalate excretion to fall as CCr falls. On the other hand, because it is secreted by kidney cells from plasma into the tubule fluid after filtration has occurred, secretion might ‘make up’ for the loss of filtration so urine oxalate excretion remains unchanged.
Our observations show the former is true. With progressively lower CCr values we find correspondingly lower urine oxalate excretion rates. The data are more scattered than for calcium, but in fact the downward regression is highly significant for both the normals and the patients.
By comparison with calcium, urine oxalate losses are more than 10 times lower. They span a smaller range mostly within one log, not four. Also note that the red normal points overlay the blue patient points showing that overall tubule handling (mix of secretion and reabsorption) do not differ.
Adjusted for Sex and Weight
Modeled as I did for urine calcium, urine oxalate depends strongly on CCr. But weight was a much larger factor. For comparison, the F values for CCr and weight were 107 and 70 for oxalate vs. 953 and 9 for calcium. As for calcium, sex was very minor in effect.
What This Means
FIltration affects urine oxalate significantly, but size, and therefore food intake and metabolic production matter much more as a proportion of the total effect for oxalate than for calcium. Perhaps this is partly because secretion plays a role.
Where Does the Extra Oxalate Go?
Unlike calcium that has in bone a vast repository, oxalate has nowhere to go if it is not excreted in the urine. Even if one says it simply stays in the plasma, that would not do. The higher plasma level would increase the amount filtered. So we must presume that either as CCr falls the liver produces less oxalate, or less is absorbed from food.
This is not the place to discuss the matter, but this note serves notice that more complexity lies below the surface here.
So What?
I said at the beginning that a high filtration rate promotes kidney stone formation and I meant to support that idea with such data as I have in stock. High filtration means that a lot of calcium and oxalate, as examples, are filtered. The one is extensively reabsorbed. The other is secreted so excretion can exceed filtration. For calcium this means that protection against stones depends upon reabsorption. Even the simple observations I showed you indicate that stone formers reabsorb calcium less than normals do. For oxalate, the total amount excreted does not differ between patients and normals. But like calcium the amount excreted falls with falling GFR.
Last Words About Glomerular Filtration
We can form stones because we filter vastly more water and small molecules than we excrete and in the process ask our kidneys to concentrate salts into a greatly reduced fluid volume compared to their original state in the blood plasma. How filtration works, and how physicians measure it matter greatly to patients who form stones. Stone formation can lead to kidney disease, usually mild but sometimes significant. Kidney disease consists most essentially in loss of filtration.
On another level, the urine risk factors for stones are produced by kidneys, and in every case their production is driven by filtration followed by elaborate kidney tubule manipulation of that filtrate. To understand filtration is the key to understanding how kidney produce the urinary stone forming milieu. We treat patients to prevent stones precisely by altering tubule function concerning the main stone risk factors. This cannot be understood in ignorance of filtration.
So filtration is the very source – literal source – of kidney function, and its main life sustaining property.
I have been a patient in the past, not one of your best I am sure. I have dropped my weight to approx 215-225.
I was lost approx 40plus pds in the past 16 months largely to diet and exercise. I did lose most weight while on a protein diet ( which problem is not good?) I used GNC Lean after reading the book “8 Week Blood Surger Diet” maintaining 800 cal per day, but I quit because of reading your articles. My question, because with my kidney stone issues I am thinking I am possibly over-dosing on using the GNC protein shake .
Hi Joseph, Protein loading raises urine calcium and stone risk. So in general you are better off with food. Protein loads also tax kidneys raising filtration rate above normal. Regards, Fred Coe
Is a high protein low carb diet safe for the kidneys if protein is obtained from food such as meat, eggs, and nuts and protein is NOT obtained from protein shakes, protein bars, or protein powder?
Hi Terri, Low carb diets are not dangerous if protein intake stays about 1 gm /kg/day. The problem with no carbs – no starches – is that protein intakes get very high. The sugar that causes trouble is refined sugar which is half fructose. Absent that, a more balanced diet with some starches and fats for calories is better than doing everything with protein. Regards, Fred Coe
It’s still not clear to me how hypercalciuria damages the nephron …?
Hi William, Hypercalciuria does not injure nephrons directly but only because of stones, tubule plugging or perhaps plaque formation. Regards, Fred Coe
I had three stones removed from my right ureter this morning by a urologist. A cat scan with contrast from several weeks ago showed four stones but somehow one of the stones slipped through the ureter wall, the doctor tells me, and will remain wherever it is doing no harm, the doctor tells me. I did pre-op where they took an x-ray of my lungs, did a blood test and an ekg. I was told these were necessary because of my age, 68. The blood work showed that the potassium was high (i’m afraid I don’t have the exact results at this moment). It’s my impression that i’ve had high potassium for decades. Could high potassium have any relation to kidney stones? This is the second time i’ve had kidney stones. The first time, 2011, a cat scan revealed one in my right ureter and it exited on its own. I was in a lot of pain back then but thought it was muscle pain. This time, not much pain but other symptoms: urgency to pee was a big one.
Hi Any, I do not understand where the stone went, but if it went through the ureter wall, that sounds like the wall was perforated. Perhaps your physician can clarify that. As for high potassium in the blood, I cannot say much because you do not give a lot of information. Is your kidney function low? Do you take drugs that raise potassium? Are your stones uric acid – sometimes they associate with high serum potassium. You might take this up with your physician, or let me have more information. Regards, Fred Coe
I am curious about where excess oxalate goes and how it’s handled when it is not excreted. You mentioned that this is not the place to go into detail, but I have “oxalate issues” and am curious to know more about this in your highly detailed and thorough way of explaining things. I unfortunately enjoy a high oxalate diet in addition to having SNPs that promote endogenous oxalate production. I have not experienced a kidney stone (yet), thankfully — that I know of, though I am having transient pains that have prompted me to look online. My eGFR based on creatinine just came back at 69, indicating a slight decrease in filtration. Looking back over the past few years, I now see that I have values in the slightly decreased category as a pattern. (I have normal BP, 24.7 BMI, and A1C of 4.7. My serum creatinine was flagged as high, at 1.0mg/dL. My cholesterol is running high as I am on a ketogenic diet. My total cholesterol is 231 with HDL-C of 75. I am also a “severe hyper absorber” of sterols — if any of this makes a difference.)
Hi Sarah, 1.0 is, technically speaking, higher than normal. Have you measured 24 hour urine oxalate? Is it high?? Ketones can increase serum creatinine by reducing creatinine secretion, so your actual clearance may be higher than you think. My best article on oxalate is here. Regards, Fred Coe
I have had fluid retention swelling in my legs for the past year. I am a 41 year old female. I am normal weight, exercise regularly and have low blood pressure. The only kidney risk factor I have is a grandmother that died of Diabetes. I had my first kidney Stone yesterday. I passed it in the emergency room. In looking at my labwork my GFR was 68 down from 108 18 months ago. Does the kidney Stone affect this result? Is that my true number? Should I be retested?
Thank You!
Hi Jessica, Very possibly passing the stone lowered your kidney function a bit. Have your physician check it in a week or two. Likewise when you are fine from the stone event, he/she might want to check another routine urinalysis. Be sure and get evaluated as to the cause of your stones, so there are no more unnecessary new ones long term. Fluid retention during the day is not rare, and usually benign and reflects some vein disease, or perhaps too high a sodium intake. I would urge you avoid diuretics for it, as one can accomodate to the drugs and it is hard to stop them in some cases. Regards, Fred Coe
Thank You so much for the quick reply!
I have a history of stones. Last eGFR in November, 2018 was 91.7. (58 years old). Latest eGFR is 78.3. Still have stone in lower lobe of kidney. Is this drop in eGFR dangerously significant?
Hi Marie, A drop like that is worrisome. Your physicians need to understand what happened and what can be done. Possibly a stone has obstructed one kidney, this can happen without pain. There are many other possibilities. Be sure your physicians figure things out and protect you against kidney loss. Regards, Fred Coe
Hi,could you please help?.i have a 9mm kidney stone and have had a stent fitted and I’m due an operation to remove the stone in 4 weeks time.at the time my stent was fitted my GFR was 45 and the morning after it recovered to 61 then 10 days later it rose to 66.i have now had another blood test after two weeks and it is 65!…do you think once they remove the stent and kidney stone that my GFR should rise further to a better result?.my GFR was measured three years ago and was 83 before I had kidney stone trouble.
I appreciate your help.
Kind regards,
Scott.
Hi Scott, I presume obstruction from the stone had lowered the function of one kidney and as draining improves function will increase – as you seem to be seeing. I would expect that when everything is over your function should return to baseline. Regards, Fred Coe
Thank you for your article. 3 weeks ago, very suddenly I experienced excruciating pain for which I went to the ER. They said I had a 5mm stone in a ureter. My GFR that day was 33. (A year before it was 65). My creatinine was 1.53. I was discharged and 3 days later I had the stone surgically removed and my GFR pre-op was 40, creatinine was 1.8. I had 30mg protein in my urine. 12 days later I had my GFR tested again. It was 42. Creatinine was 1.32. Is there any chance my GFR will increase, did it get tested too soon? I can’t understand why if problem was in one kidney why the function would drop so low, wouldn’t the other kidney still function? Thank you.
Hi Kathy, Your story is a bit confusion but I suspect the stone reduced the function of one kidney markedly. The other one will not compensate completely for many months, so your kidney function fell in half – or even more than that. But your eGFR was only marginal a year before, so perhaps you have some modest reduction (you do not give your age) common with age. If you are young, then perhaps there is an underlying kidney problem. I do not have enough information to go beyond this. But your physicians need to figure out exactly what your kidney status is. This article is pretty good as an introduction. Regards, Fred Coe
I am a 31 year old, healthy active female. No pre-existing health issues. About a year and a half ago I started noticing swelling in lower legs which has progressed to a generalized edema, even trace pitting at times (forehead in AM, legs in PM). All vascular, cardiac and other studies normal. I went to GP Feb 2019 and GFR was 69. Returned in August with GFR of 64, 30 mg/dL protein in urine, 1+ Ca oxalate in urine…GP said it was dehydration and not concerned. Due to worsening edema (although very slight), went to new PCP last week and GFR is 89 with BUN and creatinine upper limits of normal. She is referring to nephrologist. My question is, vascular study/MRI showed slight calcification of iliac artery. With this in mind, protein in urine, ca oxalate in urine and GFR <90, could all of this be caused by underlying stone issues? GFR is low for my age but trending up despite edema continuing. If it is a stone/increased calcification tendencies, can GFR improve above 90 if stone resolves?
Thanks for your help. My nursing brain is in overdrive while I wait for this nephrology referral to go through.
Hi Chantelle, I gather you have unexplained edema, some variable reduction of GFR and 300 mg/l of urine protein. The crystals probably are not related to the edema. In advance of your nephrology visit I would obtain a 24 hour urine for protein and creatinine, or at least a spot sample for protein albumin and creatinine because your nephrologist will want that. I am not sure – from this distance – if you have organic disease, apart from the protein in the absence of blood. I note that urine was very concentrated so the spot urine I suggest, or a 24 hour urine, will be critical to clarify matters. I gather your blood pressure is normal. I would be unsurprised if you end up being normal with just some variable labs, so please do not fret too much in advance. Regards, Fred Coe
Can multiple stones of varying sizes lower GFR? If removed, can some GFR be regained?
Hi David, Yes. If they obstruct, removal will certainly improve function in most cases. Stone formers are abnormally prone to reduced kidney function, and not all the reasons are clear. If you have reduced kidney function and stones, be careful to get a physician who is skilled in kidney disease and stone disease- a complex corner of medicine. These types are usually in medical schools. Regards, Fred Coe
Thank you for an excellent article!!! Just got home with a 6mm stone stuck in my right kidney. Got a stent in and need to follow-up. Was concerned about the high (1.39 mg/dL) creatinine level and low (54.54) calculated GFR. Values were taken before the stent was placed (in the middle of the whole painful misery). Thank to your article – I understand now that things should be better now (with the stent in) and possibly get even better after the stone removal (assuming all goes well).
Excellently explained with details clearly showing mechanism, logic and reasoning of why things happen!
I live in Boston otherwise I’d come to be your patient and say THANK YOU! 🙂
Cristian (48years old)
Hi Cristian, The obstruction will lower function on that side and raise serum creatinine. I would expect things to become normal when the stent is removed.
Thank you for sharing your extensive knowledge with us! At 80 years of age my mother has just reached stage 4 CKD due to recent uncontrollable HTN. I have been forming oxalate kidney stones since I was 25. I am now 55 years old. For some reason I am unable to pass any stones larger than 4mm. I currently have a 5 mm in my right kidney pole which the urologist wants to continue to watch since it is not causing much pain, only occasional discomfort. My question is: Is CKD inherited, and with my continuous formation of stones do I have also have a high likely hood of getting CKD? I would like to donate one of my kidneys to my mother but I’m sure that is probably out of the question with my kidney stone disease.
Hi Dana, I am sorry for so late an answer – this question got lost. A few forms of CKD are inherited, as are causes of stones and of both. The more likely facts here is vascular disease in your mother. Your question is very important and I cannot answer it lacking detailed information about your mother and yourself. I strongly suggest you bring the matter to your physician who does have the proper information and can be sure about any special care you might need. Regards, and apologies for lateness, Fred Coe
A question. I am 72 year old female and have a long history of stones living in both kidneys. Currently 4 in the left and two in the right. They were first picked up during investigations for gall stones at least 20 years ago. Had 4 unsuccessful lithotripsy treatments. Over the years I’ve had one removed and passed one that I know of. Don’t know what type of stone was removed but I think my family doctor could find out , Frequently have symptoms of UTI but cultures often come back negative. Makes it hard to get treatment. On one occasion I grew Morganella. My current issue is getting my blood pressure down. Family doctor has changed my diuretic but it’s still high. Home testing averages 140/80 pulse rate 80’s. Could these stones in my kidneys be contributing to this? I have a Urologist who orders a KUB yearly “to keep an eye on my stones “. Contact is over the phone. He’s never seen me or ordered a 24 hour collection. Thank you so much. I found your article helpful even though I skimmed through parts. I’m a retired nurse and back in the 1980’s worked in Urology clinics
Hi Geraldine, Yes. Stones and their surgeries can raise blood pressure. Here is my take on lowering BP in stone formers.You need to know the kind of stone – some are caused by infection.With procedures and stones a proper evaluation is the right thing. Best, Fred Coe