
 Hard unwanted objects made in the kidneys, stones can cause pain, bleeding, and urinary tract obstruction. Because stone surgery often infects the urinary system, and bacteria easily infect stones retained in the kidneys, infection follow stones like a shadow.
Hard unwanted objects made in the kidneys, stones can cause pain, bleeding, and urinary tract obstruction. Because stone surgery often infects the urinary system, and bacteria easily infect stones retained in the kidneys, infection follow stones like a shadow.
Stones surprise patients by their smallness, for all the trouble they cause, or by their largeness to think they passed through the urinary tract.
But small or large, many or few, stones provoke little love. Most who form them desire no more. Yet, left to themselves, stones recur. Over half of first time stone formers form another stone within 5 – 10 years. Once recurrent, stones form – on average – every 2 – 4 years.
So stone patients must pursue prevention and not imagine their disease will stop of itself.
Prevention consists in the search for causes and the administration of treatment. This site exists to guide both.
Crystals Make Stones Hard
Urine proteins molecules stick to tiny crystals and to each other as if designed to dispose of unwanted things. One can see in many morning urines tiny harmless crystal aggregates passed unknowingly and without harm.
In those predisposed, such protein crystal composites grow so large and numerous they can produce brief attacks of pain and bleeding but, being still too small to see on radiographs, escape detection. Such ‘crystal attacks’ are common in children with genetic hypercalciuria. Uric acid crystals can make a visible orange sludge or gravel.
When protein crystal composites grow grow big enough to obstruct the urinary tract and cause pain and we call them stones.
Very rarely urine organic molecules themselves make ‘soft’ stones that cause mild pain on passing.
Perhaps the true cause of stones hides in the chemistry of urine organic molecules, but for the moment these molecules are irrelevant to patients and their physicians. We do not know which ones most matter and about what is wrong with them that they permit stones we know essentially nothing.
So to prevent stones we work to prevent crystals. We search for causes of crystal formation, and act against them.
Stones are Crystal Artefacts
In human urine, calcium frequently crystallizes with oxalate and phosphate to produce the common calcium oxalate or calcium phosphate stones.
Other less common crystals form their own stones: Uric acid, a byproduct of nucleic acid metabolism; cystine, an amino acid that the genetic kidney tubule disease called cystinuria may liberate into urine in great excess; struvite, a crystal created by bacteria breakdown of urea, a normal urine constituent. Many drugs form crystals.
Because crystals can form independent of one another, many stones contain mixtures of them.
Like volcanic lava, an insect caught in amber, or the vague fossil tracings of some long lost species traced out in an otherwise indifferent rock, the crystals of a stone tell about a particular person with shocking precision and undeniable truth.
To find calcium oxalate crystals means such crystals were indeed once formed by that patient, and the same for all other crystals. Each crystal is a proof of past formation.
But unlike artefacts of a vanished age the proof in stones matters immediately, for in the person who made the stone those very same causes that once made its crystals may well yet operate and pose risk for more.
You might think such artefacts would attract the most intense interest and study. But no; stones are often discarded.
Stones Inform and Guide Prevention
Being as they are the artifacts and physical proof of past crystal formation, the crystals in stones guide all treatment. We can prevent stones only by preventing crystals. In any one patients the stones tell us what crystals we need to prevent. Otherwise than attend to the evidence written in stones we act in ignorance.
Stones are analysed by special laboratories
Specialized laboratories analyse stones at a moderate price.
One company has posted its prices. If you send the stone and pre-pay it is $40.00 with 2 photographs of the stone. Your doctor can get it for $35.00. This is only one of many companies that sell the service.
The report from any stone analysis laboratory is usually a single page that lists each type of crystal found in the stone and a rough approximation of the percentage of the stone each crystal accounts for.
The stones are powdered for the analysis. So a batch of stones will be cheap per stone but powdering of the batch will mix everything together; you get only an average. I would batch stones passed at one time. Analyse individually stones passed at different times because things change.
General measures can help prevent recurrence in people who have formed only one calcium stone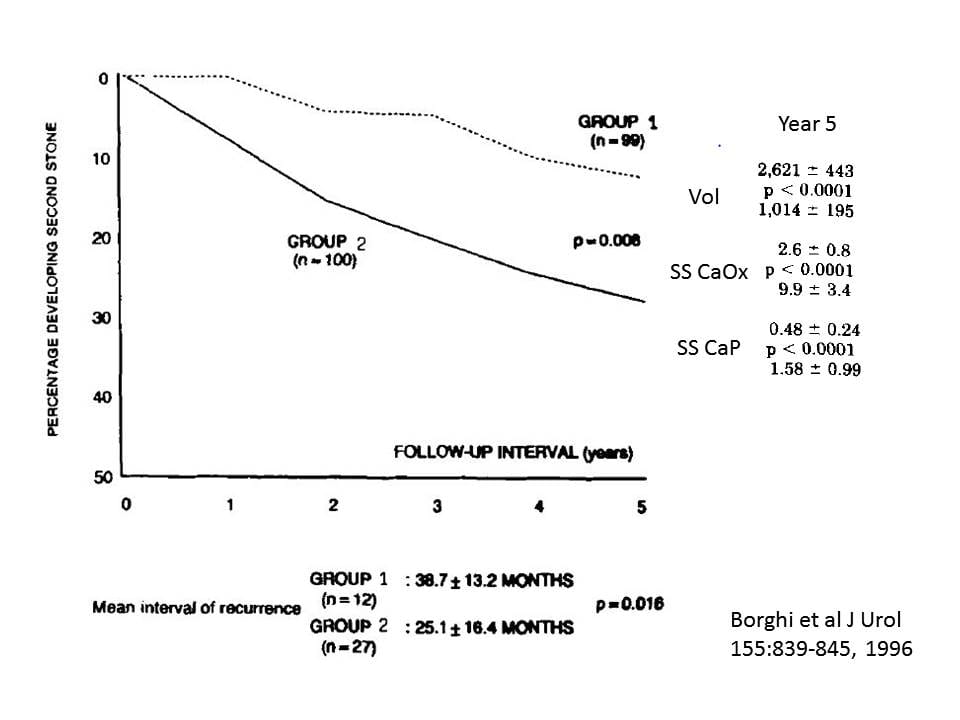
{kind=link}
Although people believe that high fluid intake will reduce stone formation, a detailed review of the literature found only one reliable trial to support that belief.
This figure from that one trial shows that formation of a new stone was delayed by high water intake in patients who had formed a single stone. After just one stone nearly 30% of people who did not increase their urine volume (Group 2, average 1 liter daily) had formed at least one more by 5 years whereas only 10% of those with a higher fluid intake (Group 2, 2.6 liters daily) did so.
As expected urine supersaturation fell with higher volume – 2.6 vs. 9.9 and 0.48 vs. 1.58, treated vs. controls, CaOx and CaP SS respectively. A fall of supersaturation would reduce the free energy of crystal formation and that could explain the fall in new stone formation.
But it is hard to do everything with just fluids. The day is long and various. We sleep by night. People forget. Crystals never sleep. Crystals never forget. In a trial, with prompting from nurses, people will maintain a high urine flow, but how about the usual situation? You want fluids. But you also want whatever treatment aims most precisely at the crystals you form. That means you need to know what those crystals are. And to find out what the crystals are the stones must be analysed.
Crystal specific treatment is far better than general measures for patients with more than one calcium stone
The patients in the water trial had formed only one stone each, so far as could be told, and only 25% of those who did not raise their urine volumes (Group 2) had another stone in five years. Among people who have formed at least several stones, 60% in the control groups of trials that tested specific treatments formed at least one more stone within 3 years. By contrast only 15 – 20% of those receiving specific treatments formed another stone during the same interval. These control patients all raised their urine volumes. None had average volumes so low as the 1 liter/day in the control group for this trial.
High water intake may well be ideal for those who have formed only one stone, but the large numbers of patients who have formed more than one stone will predictably form more stones at much higher rates and benefit greatly from treatments that focus on their specific stone crystal.
Dr. Coe
People are wanting to know what can you do about cystine stones? Some stoners are making a lot of them and having lots of procedures. They are tired of being sick.
Trish
Hi Trish, They have every reason to want to know, and I should bestir myself more. We have a brief introduction by Anna Zisman, but certainly there is more to say. You have put the matter high up on my list and I will try harder! Regards, Fred Coe
Please gibe me details of clinical significance of stone analysis, especially Calcium oxalate stones. Also suggest where I can get full details. Thanks
Sanjeev Mehta
Hi Dr Mehta, There is a good article on stone composition; another on problems with analysis. I have one on frequency of analysis: My most recent article is on the idiopathic calcium oxalate stone former and is all about the importance of analysis. I will be doing more articles on the stone forming phenotypes which will add about stone composition. Regards, Fred Coe
Very useful information about Urolithiasis
Dear Dr. Coe.
Are most kidney stones somehow attached to the wall of the kidney? If so is it quite a strong bond?
In my mind, I would think they must be attached, since if the stones are unattached and floating, most stones would come out through the ureter, while they are still small (i.e. they wouldn’t sit there and grow bigger).
Also what are the densities of the stones compared to the density of urine? I would imagine that the stone density is higher than that of urine. Does that mean that if a stone has formed in a location that is lower than the opening to the ureter, such a stone would never come out on its own, and would just sink to the bottom of the kidney? (this would only be true if stones are not attached to the wall of the kidney)
Thanks
Nihal
Hi Nihil, Here is a video on how stones form. Crystal densities are higher than water. The urinary tract contracts, so gravity plays little role. Regards, Fred Coe
Dear Dr. Coe,
That was a very informative video. Thanks!.. I still have a couple of questions.
So from the video, I learned that the stones are attached to the kidney wall (I saw the mark left on the kidney wall left by the surgeon after stone removal in the video). I would think that that implies a considerable force is needed (a force equivalent to the force needed to break the stone) to dislodge the stone. But we know that people pass stones on their own all the time. So how do stones dislodge on their own? Is excessive movement such as running enough to dislodge a stone from the kidney wall?
Also you said above “the urinary tract contracts”. Does that mean that the kidney contracts every so often to squeeze the urine out of the kidney?
Thanks
Hi Nihal, The tissues separate the stone from its base – the cells are alive. The urinary tract is the renal pelvis and ureter, not the kidney. Regards, Fred Coe
Dear Dr. Coe,
It’s been a month after my sugery,
as per result sent to US it says that my stone type is
100% Carbonate Dahllite Apatite
I have read your article but couldn’t find exact answer.
Looking forward.
Regards,
Hi Marion, Thank you for asking. The fancy name is just calcium phosphate as hydroxyapatite – with admixed carbonates. In the article it is calcium phosphate stones. Your presumed phenotype is here. Be sure to get a full evaluation for cause, and then proper treatment, Phosphate stones can grow rapidly and large in some people. Regards, Fred Coe
Dr. Coe
I was diagnosed with stones on Tuesday. I am on blood thinner (Effient) Started bleeding in urine last night.
Hopefullt the stone is moving
just now a black piece came out into strainer but it seems a little soft so I am thinking it is coagulated blood.
How do I know if tht was stone?
I have been 9 months on thinner and am supposed to go 1 year.
Should I get off or will bleeding stop?
thanks
Hi Rob, blood thinners and stones and bleeding is a complicated situation. If you think you passed a stone, get it analysed to find out. If you are bleeding clots can feel just like stones – so are you sure there are stones and that they are the cause of bleeding. This is one for your urologist who needs to ascertain the cause of the bleeding. Right now that is the problem. I am afraid that I cannot add much from here. Regards, Fred Coe
Hello Dr Coe
The 5 mm stone has moved to the “sphincter” just before the bladder
the pain is tolerable. I went off the blood thinners but am back on. How long can/should I wait for it to pass and any tips how to get it that last 1/4 inch into the bladder?
I do not look forward to laser etc.. NYTimes did an article that says big chance of a problem
thanks in advance
Hi Rob, You can wait so long as the kidney is not obstructed. This is a situation in which your personal surgeon is the only person who can make an intelligent decision. Boston, as I said in my personal email to you, is filled with excellent physicians, so I am very confident. Regards, Fred Coe
Hi Dr. Coe,
I am a chronic former of calcium oxalate stones. In late 2015, I had shockwave therapy twice to breakup a 10mm stone in the UPJ left kidney. Just recently, I had laser lithotripsy to remove a 5mm stone near the bladder, a 1cm stone in the UPJ, and a 1.2cm staghorn stone at the bottom of my right kidney (along w/multiple stones of smaller sizes). My CT scans shows I have multiple stones of 4mm or less in my left kidney. Between these procedures, I’ve passed multiple smaller stones. What causes people like myself to develop so many stones so frequently and what can be done to stop the formation? I’m on a low oxalate diet, try to consume water to make 2L of urine per day (very hard to do), and take potassium citrate (540 mg).
Thank you..
Hi Theresa, Here is a way to think about your stone forming and how to stop it. An oxalate list and fluids are never enough. Take a look and see if it helps. Regards, Fred Coe
I have produced a stone first on the right kidney early this year that is soft in nature, and so big it won’t pass. through the tube. I’m a 60 year old male with prior history of stones. Nor any prior family history. It formed and then shut the tube off. Two days later my kidney shut down and by then I had gone septic from infection. Then three months later the left side did the same thing. Back to the hospital for treatment for blood infection for a week of antibiotics. Both times I went to surgery for a stint to open up the tube and allow urine to flow so they could treat the blood infection and then once the Infection is cleared up then they go back in and laser the stone, bust it up , and put in a second stint for a week or so to allow kidney to function normal then pull it. This are very soft, crumbley material. I have been drinking water with a large amount of lemon juice in it for about 8 years now and wondered if it could be related to what is going on
Hi Edward, Of highest importance, what is the stone material made of? I would worry it is struvite or uric acid. You need urgent means to prevent more, as sepsis is horribly dangerous. Regards, Fred Coe
Hello,
I have a history of calculi in both kidneys, first diagnosed at age 19, lithotripsy on the right kidney at age 21 after evaluation of a calcium oxalate stone that passed, a few infections treated in the next few years and no more trouble for over a decade. No trouble meant I more or less forgot about diet and fluid intake and now at age 38 my last tomography shows numerous stones in both kidneys, all small and dense – the largest in the upper third of the left kidney is 5 x 4 mm 1200 UH, all others are smaller than 4mm.
My urologist says nothing can be done except drink a lot of water and new exams every year to control. I am looking for another specialist and came to your very informative website. I was surprised to learn a higher calcium intake is recommended. I haven`t noticed other stones passing so I am not sure if it is possible to evaluate their formation. What are other recommendations?
Thank you!
Although I am fine for now, I worry about the impact of theses stones in kidney function later. My urologist was reticent when I asked what would happen in my 80s if I don`t treat these calculi.
Also, my urine exams show normal levels of oxalate, uric acid and all other elements.
Hi Liege, if you are forming new stones, and your present levels in the urine are not abnormal, think carefully about conditions of work life or other factors that might have causes new stones and yet escape the samples of urines you collected; they are one day clips out of a lifelong movie, and therefore easily fooled. Regards, Fred Coe
Hi Liege, what your urologist said is not complete. Here is a good starting place for a prevention plan. One treats the whole patient – stones imply other disease risks. High calcium, low sodium diet is how we always proceed – this article needs to be read after the other two. Regards, Fred Coe
hi,, Dr.
which madison is better for kidney stones,
i have booths kidny stone(less Than 5.5mm)
& i take more madison also .
Hi Jagat, It is not so easy to choose a treatment; you need to know what the stones are and why they form. Take a look here, for a good start. Regards, Fred Coe
Hello Dr. Coe,
I am a PA in a urology practice. I have a patient , a woman , 47yo. Most recent CT scan shows numerous stones in both kidneys. And yet her 24 hour urine results while not quite perfect are as follows: urine vol = 2.76L ; SS CaOx =1.25; urine Ca = 70 ; Oxalate = 25; citrate = 758; SS CaP = 0.18; pH = 5.975; SS UA = 0.44; UA = 0.565; urine Na = 175; P24 = 0.960. Her stones are CaOx monohydrate. What am I not seeing ?
Michael Connell
Hi Michael, Her present urine would not have produced stones. I suspect in her history you will find periods in which urine chemistries would have been most abnormal. Regards, Fred
Hi Doctor,
For the past 3 years I have experienced episodes that occur seemingly ever 3-4 months, they started when I was 19, and I have been to multiple different urologists, given samples of these “stones” to be tested, and have gotten no results, in fact, the last one said he hasn’t really seen anything like this.
When this occurs, I pee out upwards of 20 small mushy stones that when I pick up and rub my fingers over, they dissolve. Some can get as big as a pencil eraser, some are very small. Each time I have this as mentioned above, I will pass over 20, and I quickly drink lots of water to flush my system and then it’s over. They are typically white or very light yellow in color.
The first doctor I went to for this 3 years ago, ruled it as a UTI and I was treated for that. It did not stop occurring so I continued to schedule appointments (which takes months to get in). I had an ultrasound done about a year and a half ago which came up empty. In April 2019 I had a scan done with iodine which also showed nothing. I was able to present a sample in my urine to one of the doctors but when he tested it, he stated that it just fell apart like they typically do when enough pressure is applied. Do you have any advice or thoughts on what this could be and what my next steps should be? I am currently at a loss after the last visit.
Thank you so much in advance, I hope you see this
Hi Matt, So called ‘Matrix stones’ are well described. This link to page one of a J Urol article described what you found. They usually suggest infection so perhaps your physicians should check for that. In some cases these are lightly mineralized and reflect stone crystal formation but the crystal part is too slight to sense. ANalysis by infrared spectroscopy – the common commercial stone method – may yield the crystal. 24 hour urine testing is in order to see if your urine harbors stone risk factors. Regards, Fred Coe
Hi Matt,
Did you ever figure out what this was? I am dealing with a similar issue.
Thanks
Hi I have been experiencing recurrent upper uti symptoms after starting topirimate for migraine prevention. Uss kidneys are ok but I’m concerned I may have developed kidney sludge. I have stopped the topirimate. Should this clear itself?
Hi Emma, Topiramate causes stones by producing a form of renal tubular acidosis. The crystals are phosphates, and you are wise to stop it. Your physicians may wish to obtain a low dose CT to see if there are stones in the kidneys. Ultrasound is much less sensitive. Other migraine drugs can be like this one, so be careful. Regards, Fred Coe
I’ve had a calcium oscillate stone in the past, Now the stones Im passing are soft, some are pink some look like blood clots, but they look more like tissue, Dr. said caused by infection but I dont have infection, From what I’m reading they may be matrix stones? I dont know if Im getting enough information from my Dr.
Hi Paul, I would be guided by your physician. If infection is causing clots or loss of tissue it is a serious infection, and we must rely on her/him to fix it. If you are not infected, that would imply an error of your physician, unlikely but also very important and pointing to a need for some additional medical help. Regards, Fred Coe
Hello. I just received an analysis back of a “stone”. They said it was organic material and were not sure what it was. I will be having surgery soon since I have several large stones in both kidneys. Any idea what organic material may be?
My doctor will discuss it with me at my next appointment. But until then, what are your thoughts?
Hi Lori Ann, Not rarely a stone will form with so little crystal that all you can find in a routine analysis is the matrix protein that holds the stone crystals together. I suspect other stones will eventually show the stone. Alternative possibilities is a blood clot, tissue from the kidney. Regards, Fred Coe
Hi I have a question,
In august of 2020 I had a neg-coag staph infection, was given cipro for 5 days and the symptoms never fully went away. Currently I have pelvic pain and pressure, lower back pain and aching during and after peeing along with a weak stream. Two days ago I passed a soft yellow stone with mild pain. I have done some research and it seems it could be a struvite stone? I am still in pain since though. Urine tests show no infection. Thank you for your help in advance
Hi Emily, Have the stone analyzed. If it is struvite you need special handling to prevent more problems. The 24 hour urine can help, struvite forms in urine that is very alkaline (high pH) and also has a lot of ammonia in it. Regards, Fred Coe
Hi Dr Coe! I have to say I nerded out with your paragraph “You might think such artefacts would attract the most intense interest and study. But no; stones are often discarded.”
I agree! I think they are so fascinating! Some downright beautiful! I had a whole collection saved but sadly a doctor wanted it and My whole collection, that I was only proud of, was wiped out. It’s ok… I’m rebuilding! I believe I get uric acid stones. Anyway I passed one today, not even terribly big, but it took 3-4 days. I was looking at it under one of my kids microscopes (awful quality but enough to assist in satisfying my curiosity). I’m pretty shocked at what I saw with only 10-20x magnification. I saw the normal crystalline formations but also what look like (and I apologize because it’s kinda gross) roots or insect legs. Like other organic matter under a microscope it had translucent qualities with bits inside the root/leg structures. I thought to look up if maybe parasites or something could pass as part of a stone but cannot find anything that would support that hypothesis. My slide and microscope aren’t sterile and I wasn’t overly particular in handling it from the screened funnel to some toilet paper to the slide. And I have been taking the urinary analgesic that makes your urine Easter egg dye orange. But these things don’t appear to be from contamination, they appear to be partially enveloped in the stone with random bits poking out of the crystals here and there. Also they were stationary. Nothing moving or wiggling. They were not uniform in shape and size either.
Have you ever come across something like this or do you have any insight what it might be? As gross as it may be, and maybe a smidge concerning, I really am interested in learning what it might be. I’m fascinated because it goes against the expectations I have of urinary waste and stones in general. Thanks for taking the time to answer questions for me and the others, it’s very considerate and I appreciate it.
Dear Sarah, If you make uric acid stones, you can stop them from forming. That will ruin your collecting but stop any pain and – I might say – dangers from the stones. Under any microscope stones are lovely, being crystals; their shapes like the stars make us think of things, too, so we can see in them our dreams, and our fantasies. As for you, stop the stones by reading the article and doing what is says. Thanks for a wonderful post, Fred
You note that “Very rarely urine organic molecules themselves make ‘soft’ stones that cause mild pain on passing.” My 23 year old daughter has episodic kidney pain. When the pain gets worse, she will pass debris in her urine–that sometimes looks like sand, or sometimes consists of larger matter. This can be quite painful. Two times her stones have been sent away for analysis; both times the result was “100% organic matter–blood and tissue.” One stone was measured within each sample and they were: 4.0mm x 6.0mm x1.00 mm weight 1.0 mg, and 1.5mm x 2.0mm x 1.5mm weight 17mg. Her urologist was very dismissive that she could be in pain and said he could not help her, as he found no structural reasons for her pain. Her nephrologist is sympathetic but doesn’t suggest any treatment plan. What could be causing these painful stone-like debris of organic matter, and what additional tests or other avenues should her doctor consider?
Hi MH, Protein stones can be painful, passing blood clots down a ureter is not without pain, too. Almost certainly, given her age, these protein aggregates are being formed around crystals. I would advise sending the samples to Litholink where stone analysis is very refined (I founded Litholink but have no financial interests in it. There will be crystals, and these can be prevented. Regards, Fred Coe