Kidney stone types

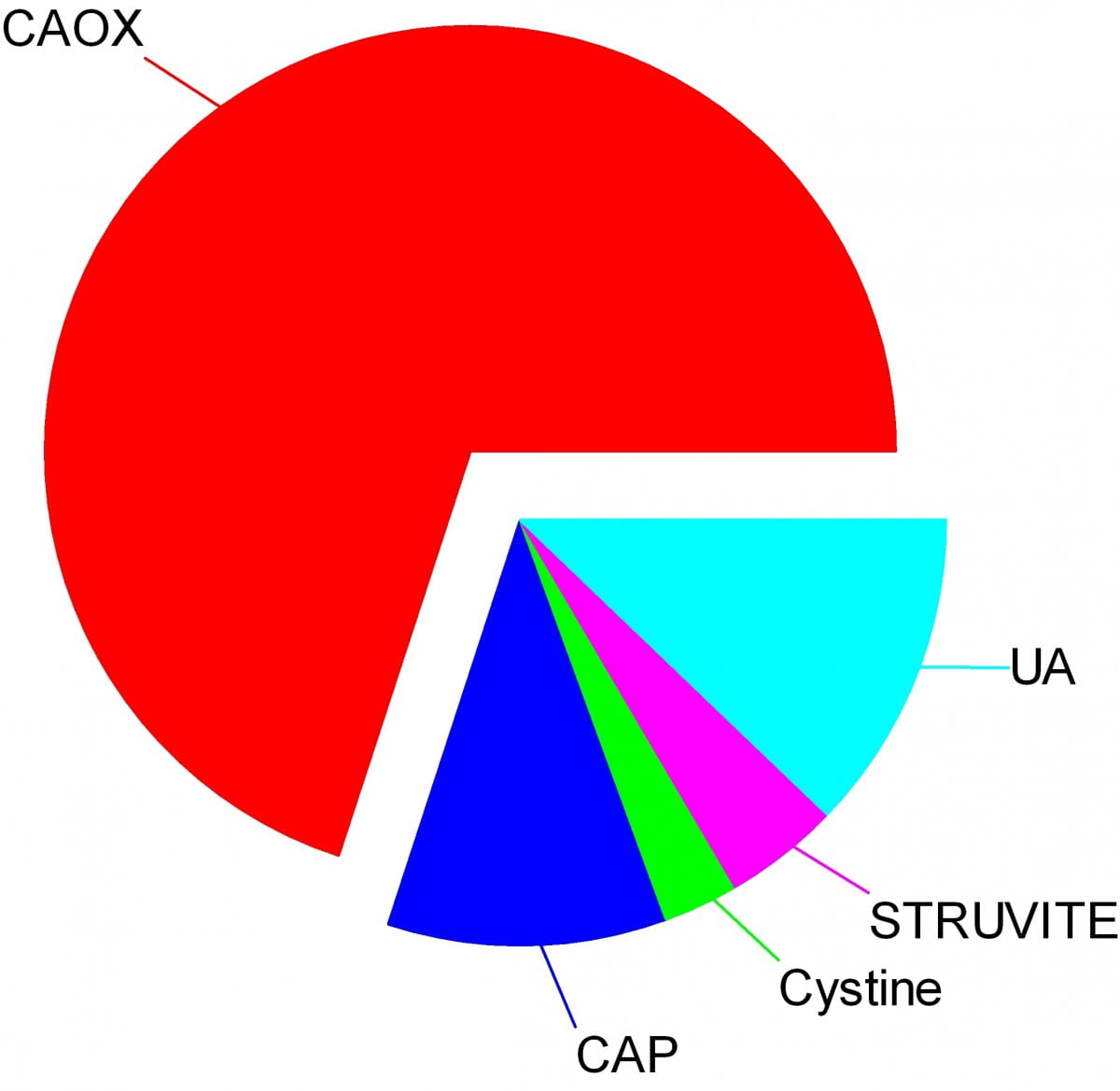
Crystals make stones and their names signify the kidney stone types. Here are the names of the crystals that make the stones: CAOX, Calcium Oxalate; CAP, Calcium phosphate; UA, Uric Acid; Cystine; Struvite.
The wedges on my pie chart show the relative abundances of stone types in our large population of stone forming patients. Calcium oxalate stones predominate by a wide margin in our clinic and in all others I know of.
The names, matter because the whole science of stone prevention focuses upon stone crystals. Each kidney stone crystal creates its own unique illness and requires specific treatment. That is why we name stones by the names of their crystals and why when stones are analysed the results are reported by these very same names.
Being a bold and rather large graphic, the featured picture does what I intended, brings the main facts into view as, at a circus, the great animals and the small animals circle the ring by way of an introduction. Come. I will show you all the common stones, like at a fashion show, or a circus parade. You can watch as they go by and remind yourself, or wonder, which ones might have been yours.
Here they are.
Which type do you have?
You might think your doctors know what stones you have formed, but don’t rely on it. People move, doctors move, health records are far from ‘all electronic’. That stone report from 4 years ago could lie in a dusty filing cabinet, your new doctors unaware it exists. Worse, it could hide in a dresser drawer and you forgot it you put it there. Perhaps even more worse, the stones might stay in that drawer, never analysed at all. Find the stones, find missing reports, urge analysis by your physicians. They can help you most if they know your stone analysis.
When they do not know, physicians can still mount prevention efforts but with less focus and probably less effect than when guided by a knowledge of the crystals. So always seek treatment. If a stone comes along the way, make every effort to get it analysed.
Why should you care to know all this?
Because you will conduct much of your own treatment, and over many years.
Since stones tend to recur, prevention requires treatment over long periods. These treatments work by altering urine chemistry in a direction that minimizes the risk of forming crystals. Such altering of urine chemistry requires control of fluid intake, lifestyle, and diet, and sometimes additional use of medications.
Just as the sailor who aims along a chosen track against the random, misdirecting, confusing sea and air maintains a constant way in proportion to that skill which comes from knowing the way of the boat, patients who aim to keep a certain kind of condition in their urine despite the demands and temptations of the world do so, I believe, in proportion to skills that come from knowing how their work and lives and foods affect their bodies, and how those crystals form which they so much desire to prevent.
Put another way, knowledge is power.
Why is this article so long?
I wanted to put all five main types of kidney stones. That makes a long story. But probably you will care to read about only your own type.
I should mention here, to save a lot of confusion, that stones often contain mixtures of crystals.
The pie chart refers to the most common crystals in a stone, for which the stone is usually named. Much of the time, minor crystal components are not crucial, but sometimes – to jump forward a bit – they are. Even a trace of struvite or cystine, for example, can have great diagnostic importance.
Calcium stones
Calcium Oxalate Crystals
In the great circle atop this page article, the calcium oxalate stone, being most common, occupies a lion’s share of the space. 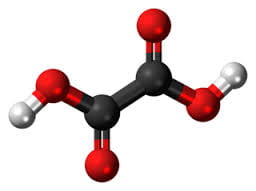
The calcium oxalate crystal forms when calcium combines with oxalic acid. Oxalic acid (at left), a dead end waste product that the kidneys remove, contains two carbon atoms (the large black spheres), four oxygen atoms, and two hydrogen atoms (silver).
At the acidity of urine, the positively charged hydrogens leave their negatively charged oxygens. As a result the oxalate molecule carries two negative charges. In the figure at right one negatively charged oxygen attracts the hydrogen of a nearby water molecule (H – O -H) while another attracts a positively charged calcium atom.
You can imagine how another oxalate ion (the name for a charged molecule in water) could attract the same calcium, or another calcium atom attract the bottom oxygen on the oxalate molecule so the chain extends and makes a crystal. You can see more about this in a video I made. Broadly speaking – though my more expert colleagues may bridle at such a simplification – the calcium atoms and oxalate molecules combine by the attraction of their opposite charges.
The calcium oxalate kidney stone comes in two varieties, calcium oxalate monohydrate and calcium oxalate dihydrate. The former are harder and therefore more resistant to fragmentation by lithotripsy. Likewise, the former appear more often when elevated levels of urine oxalate are present.
Calcium oxalate stone formers
From Systemic Diseases
Sometimes this kidney stone arises from a systemic cause, like bowel disease, primary hyperparathyroidism, or primary hyperoxaluria. Only physicians can establish that a known disease – like bowel disease – is the cause of stones. Only physicians can discover underlying primary hyperparathyroidism as a cause of stones. Patients cannot do much for themselves except provide as complete a medical record as possible.
Idiopathic
Most of the time this kidney stone arises simply from the interplay between inheritance, diet, and aspects of daily living. We call such patients idiopathic calcium oxalate stone formers, from Greek ἴδιος idios “one’s own” and πάθος pathos “suffering”.
Even though physicians discover the links between daily living and stone production, and select those changes that can prevent new stones, patients themselves must create and maintain those changes. I believe patients can so this in proportion to how well they understand what is needed, and why. When changes in daily life are not enough, physicians add medications, so even then patients remain active therapists for their own disease.
Stones usually form on kidney surfaces
About one million nephron units make up a normal adult kidney. The calcium oxalate kidney stone type does not grow in the tubules of the nephrons but ‘outside’ them, on the surfaces of the renal pelvis where final urine collects and drains through the ureter to the bladder. Here is a video that shows how they can form.
Calcium phosphate crystals
Phosphate ion and urine pH
Calcium phosphate stone crystals form when calcium atoms combine with phosphoric instead of oxalic acid and produce the calcium phosphate kidney stone.
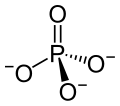 Phosphoric acid is simply a phosphorus atom (shown as the ‘P’ in the line drawing to the left) with 4 oxygen atoms bonded to it. One oxygen atom has two lines for its bond to phosphorus; this oxygen cannot provide any charge with which to bond calcium atoms to make a crystal. The other three have ordinary bonds that are shown by a line, and a dashed and solid arrow. These two arrows mean simply that the oxygens lie above and below the plane of the paper – so if you built the molecule with sticks and balls it would have a three dimensional shape.
Phosphoric acid is simply a phosphorus atom (shown as the ‘P’ in the line drawing to the left) with 4 oxygen atoms bonded to it. One oxygen atom has two lines for its bond to phosphorus; this oxygen cannot provide any charge with which to bond calcium atoms to make a crystal. The other three have ordinary bonds that are shown by a line, and a dashed and solid arrow. These two arrows mean simply that the oxygens lie above and below the plane of the paper – so if you built the molecule with sticks and balls it would have a three dimensional shape.
One of the three negatively charged oxygens never has a hydrogen on it in urine but only in exceedingly acidic solutions. A second charged oxygen is always occupied by a hydrogen atom in urine.
This makes the third oxygen, variably occupied by a hydrogen in urine, a tie breaker.
In a urine of average normal acidity (pH around 6), most of the tie breaker oxygens have their hydrogen leaving the phosphate ion only one negative charge. Not enough to make a crystal.
When the urine is abnormally alkaline (pH above 6.3 or 6.5), the variable oxygen becomes charged so the ion has two negative charges that can combine with calcium to make crystals. For this reason the calcium phosphate kidney stone tends to occur in people who produce a more alkaline urine than those who produce calcium oxalate kidney stones.
Brushite vs. hydroxyapatite
Much like calcium oxalate, calcium phosphate crystals begin simply as one to one pairings of doubly negative phosphate ions with doubly positive calcium atoms. This initial crystal is named brushite. Brushite, which is an equal mixture of calcium and phosphate ions, can convert to hydroxyapatite (HA), which has a more unbalanced proportion of calcium to phosphate. Hydroxyapatite crystals make bones hard.
Because less soluble than brushite, hydroxyapatite cannibalizes brushite. The organic molecules in urine modify this process.
Calcium Phosphate stone formers
From Systemic diseases
Primary hyperparathyroidism and renal tubular acidosis raise average urine alkalinity (higher urine pH) and foster calcium phosphate kidney stones. Many uncommon genetic diseases do the same.
Idiopathic
Idiopathic calcium phosphate stone formers share a common set of traits. Perhaps because urine contains far more phosphate than oxalate, they form more frequent and larger stones than idiopathic calcium oxalate stone formers. Often the stones originate as crystal plugs at the terminal ends of the kidney tubules. More crystals deposit over the end of the plug open to the urine, to make the final stone. Crystal plugs damage the cells that line the tubules and cause local scarring.
Uric acid stones
Uric acid crystals
Structure and charged sites
A breakdown product of DNA and RNA, uric acid forms crystals in abnormally acidic (low pH) urine. Obese and diabetic people, those with gout or kidney disease typically produce abnormally acid urine. I know how the urine becomes acid, but leave it for elsewhere on the site.
Uric acid, the molecule we are interested in here (shown to the far right), has two linked rings made of carbon atoms (they are at the angles where lines join), with  interposed nitrogen (N), oxygen (O), and hydrogen (H) atoms.
interposed nitrogen (N), oxygen (O), and hydrogen (H) atoms.
This molecule has only two charged sites, the nitrogen atoms at the bottoms of the rings. In urine of pH 6 or so, one nitrogen lacks its hydrogen and therefore carries a single negative charge. In more alkaline solutions both nitrogens lack hydrogens, but urine does not normally achieve such alkalinity (pH>8).
When urine pH is low (<5.5) and both nitrogens have their hydrogens, the molecule lacks any charged site, so water can no longer find a hold on the molecule. It crystallizes. It simply leaves the water as water droplets themselves form from the high and vaporous late afternoon clouds and fall from the air as the warm rains of springtime.
Relation to water
Water molecules are each a single oxygen atom (large ball) bonded with two hydrogen atoms (small balls) as in this picture from Wikipedia. The hydrogen side has a positive, the bare side of the oxygen a negative charge. So water molecules link to each other, 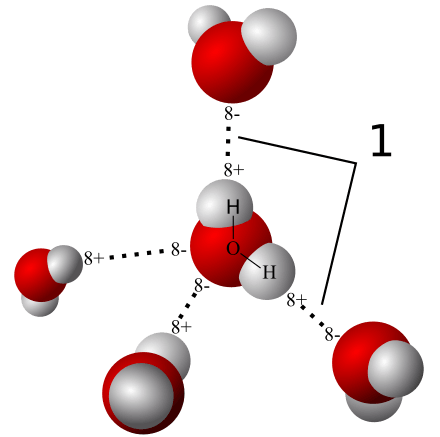 positives to negative surfaces, to make up the clear and seemingly continuous fluid we drink, swim in, and hold up umbrellas to keep off of us when it rains. They link by charge at angles, shown by the number ‘1’ so as to make up a three dimensional macrame.
positives to negative surfaces, to make up the clear and seemingly continuous fluid we drink, swim in, and hold up umbrellas to keep off of us when it rains. They link by charge at angles, shown by the number ‘1’ so as to make up a three dimensional macrame.
To be ‘in solution’ means to have some charge to which water molecules can link up with by attraction. Calcium atoms are positive and become surrounded by a shell of water molecules facing it with their bare negative surfaces. Oxalic and phosphoric acids have negative charges and are surrounded by water molecules pointing their positive or hydrogen sides to them.
Uric acid at neutral pH has its one negatively charged nitrogen water can grasp. But when pH falls, and neither nitrogen has any extra charge for water to bind with, how can the molecule remain among the water molecules? It cannot. The molecules stack into solid crystals and fall from solution.
Uric acid stone formers
The stones can be orange – red, large, and numerous
The stones can be red or orange because uric acid crystals absorb hemoglobin breakdown products that are red – orange pigments in urine. Sometimes uric acid crystals pass in urine as a red orange gravel.
Uric acid does not have to connect itself to some other atom or molecule to make a crystal, in the way that calcium must bond with oxalate or phosphate ions to make calcium oxalate or calcium phosphate crystals. When pH is low enough to extinguish its charge, uric acid can crystallize very fast, in seconds, and pass as an orange gravel in the urine. If retained, such crystals can grow rapidly into large stones. Because there is much more uric acid in urine than there is oxalic acid, uric acid stones can grow very large and rapidly. Some fill up the entire collecting system of the kidney.
Urine pH controls stone formation
But because the whole process depends almost completely on the acidity of the urine, uric acid stones are very easy to treat. Just a modest amount of supplemental alkali will make the urine of almost any patient alkaline enough that the hydrogen atoms are removed from the one crucial charged nitrogen. Water can bond there so uric acid remains in solution. Because so simple, treatment prevents stones with certainty. Relapse need never occur.
Mixed stones require special care
Unfortunately, however, stones commonly contain uric acid mixed with calcium oxalate. In this case, one needs to track down the cause of the calcium oxalate stones as well as make the urine alkaline enough to stop uric acid stones from forming. Calcium phosphate crystals mix with uric acid only rarely, because it takes a rather alkaline urine to remove the hydrogen atoms from phosphate so it has two negative charges and can bind efficiently with calcium atoms. At that higher pH, uric acid will have its charge site and remain in solution.
Struvite stones
Urea and the planet
Kidneys cannot make struvite. Bacteria make it. Not all bacteria, either. It takes bacteria that normally thrive in the soil, and they do it for ancient and compelling reasons. These bacteria produce the kidney stone named Struvite after Heinrich Christian Gottfried von Struve (1772–1851).
Animals deposit urea (at left) all over the planet when they urinate. Plants cannot use it.
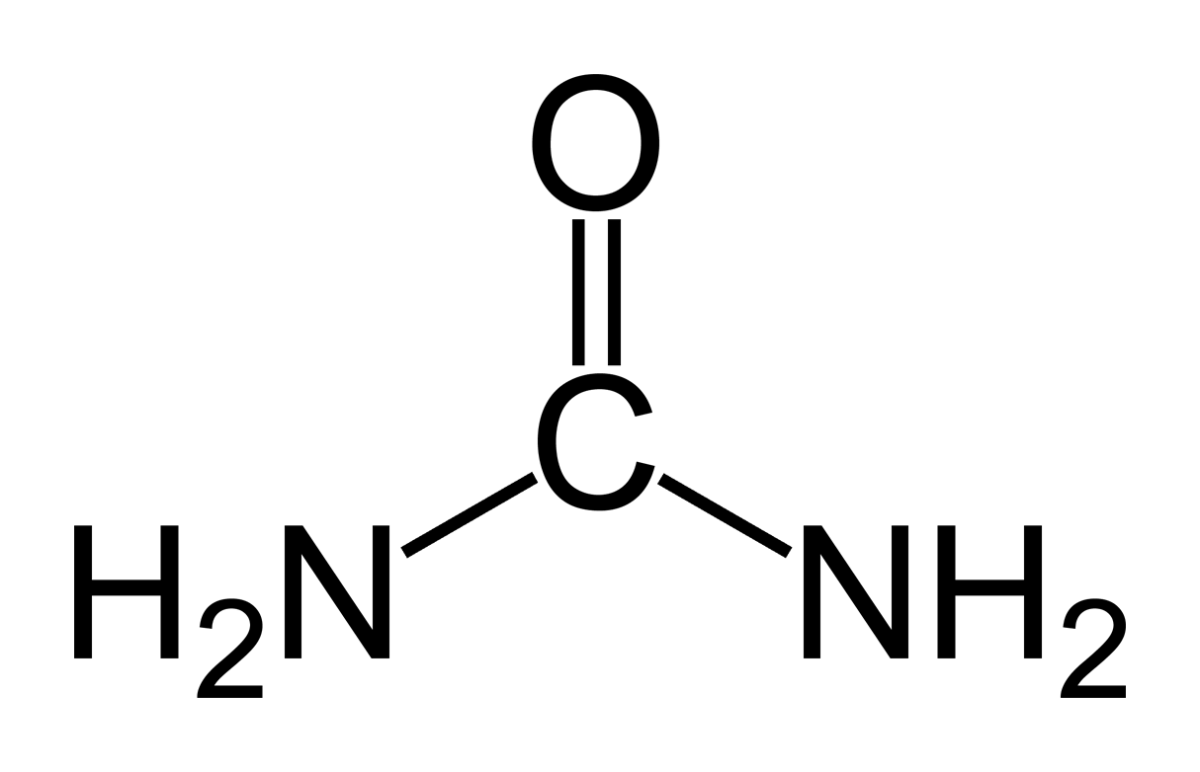 Like oxygen, nitrogen is an essential for life yet dangerous. It is integral to proteins, DNA and RNA. As these molecules are broken down and remade, some of their nitrogen slips by and can form poisonous compounds unless caught up in safe waste products. Of these, the main one, urea, contains 2 nitrogen atoms bound to a single carbon atom (‘C’ in the picture to your left).
Like oxygen, nitrogen is an essential for life yet dangerous. It is integral to proteins, DNA and RNA. As these molecules are broken down and remade, some of their nitrogen slips by and can form poisonous compounds unless caught up in safe waste products. Of these, the main one, urea, contains 2 nitrogen atoms bound to a single carbon atom (‘C’ in the picture to your left).
Uric acid contains 4 nitrogen atoms (look back at the picture of it). Birds and reptiles excrete most of their nitrogen as uric acid; mammals like us excrete nitrogen mainly as urea.
As the animals of the world urinate on the soil, their urea brings nitrogen to plant roots, but the plants cannot use it. They cannot release the nitrogens from the carbon atom that holds them. Those soil bacteria that make struvite crystals have an enzyme, called urease, that can release the nitrogen for plants to use as their nitrogen supply.
So, soil bacteria with urease maintain the nitrogen cycle of the earth.
Struvite crystals
As they release nitrogen from its carbon in urea, the nitrogen takes up a proton making ammonia (NH3). Ammonia is a powerful alkali and takes up another proton.
As it does so, the working bacteria surround themselves with spheres of very alkaline fluid enriched with ammonium ion (NH4) that carries one positive charge. Soil magnesium ( an atom with two positive charges) and phosphate sans all of its protons (an ion with three negative charges) spontaneously form their triple salt: three negative phosphate charges, two positive from magnesium, one positive from NH4).
The crystals anchor the bacteria and help create a porous nitrogen rich soul good for plants to grow in
The struvite kidney stone
Why they start
Because urine is filled with urea, soil bacteria that get into the urinary tract can break it down to ammonia and create struvite from the magnesium and phosphate urine always contains.
You might wonder how soil bacteria get into the urinary system.
Because we eat them, with foods that are not cooked, and they become part of the intestinal bacterial population from an early age. In us and around us, they find a way into the urinary system, especially in women whose shorter urethra makes entry easier. No matter how skillfully used, any instrument put into the bladder can carry our personal soil bacteria with it.
What they do
Because they live among molds and fungi, soil bacteria easily mount resistances to antibiotics, so antibiotics given for a urinary tract infection will tend to kill sensitive bacteria and select out those that can resist them.
Soil bacteria can produce struvite stones de novo, or infect calcium stones to produce a mixed stone. Either way, struvite stones are infected by their very nature. They can become huge. Their bacteria can injure the kidneys, even enter the bloodstream and cause sepsis.
Treatment is a mix of thoughtful surgery and selection of antibiotics after such surgery to kill bacteria that remain. If the stones are a mixture of struvite and calcium crystals, new calcium stones need to be prevented.
Cystine stones
Inherited kidney abnormality
 Lemon yellow with a sugary coating these form only in people who have an inherited kidney disorder called cystinuria.
Lemon yellow with a sugary coating these form only in people who have an inherited kidney disorder called cystinuria.
Although the kidneys function well, they permit abnormal amounts of four amino acids to enter the urine. Three do not matter that we know of. The fourth makes crystals and the cystine kidney stone type.
Cystine
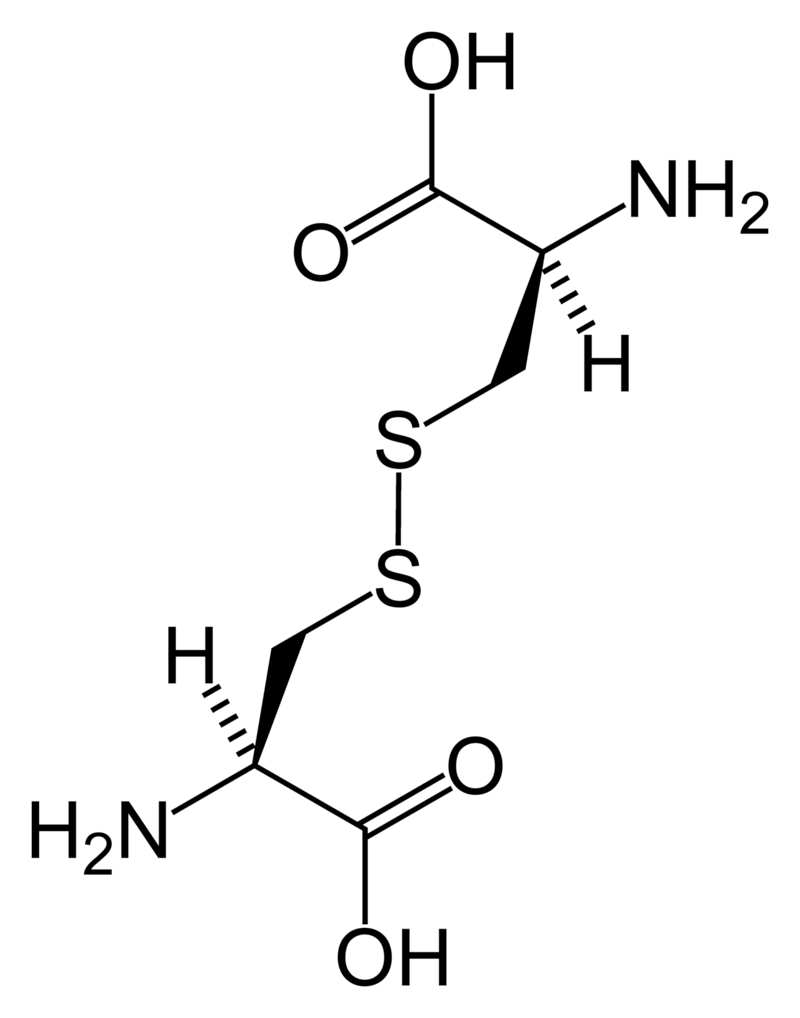
Cystine (left) forms through the coupling of two identical amino acids – called cysteine – through their sulfur atoms (‘S’ in the line drawing).
Each cysteine contains two carbon atoms – not shown except as corners – bonded together (shown by the single long line that connects the two corners) as in oxalic acid.
One carbon atom has 2 oxygens bonded to it; the other has one nitrogen (which makes it an amino – nitrogen containing – acid), a hydrogen atom, and a sulfur atom. As for phosphate, the dashed and solid arrows simply mean the hydrogens and sulfurs lie above and below the plane of the page and a stick model would have a three dimensional shape.
Cystine Crystals
Cysteine itself is very soluble because the sulfur atom has an appreciable negative charge.
But the big, long cystine molecule has very little charge because the sulfurs bind to each other. So, like uric acid, cystine loses intimacy with water molecules and simply leaves the solution as crystals. Also like uric acid, the process is fast.
Cystine stones
Because people with cystinuria lose large amounts of cystine in their urine stones readily grow large, and fast.
Stones probably form in the urine itself. But cystine crystals can plug the ends of kidney tubules, as calcium phosphate crystals do, causing cell damage.
Since cystinuria is an inherited disease, stones may begin in childhood.
Effective treatment always requires very large amounts of fluids to dilute the urine. The few effective drugs resemble cysteine. Their sulfur groups bond with cysteine to form a ‘mixed disulfide’ more soluble than cystine. But their side effects can limit use.
Rare stones
Here and there we find patients who make uncommon crystals and require very special care.
Uric acid, as an example, can form odd crystals such sodium or ammonium acid urate, especially in people with bowel disease and chronic diarrhea.
Anti-viral drugs can crystallize in urine and form stones only recognized for what they are through stone analysis.
Very rare disorders of metabolism can produce molecules which crystallize in the urine, for example 2-8 dihydroxyadenine.
Although it can take a while before the right answer emerges, stone analyses will put physicians on the right track for these special cases.
The end of a very long post
That’s my parade.
The common animals and the rarer animals have gone by, and you have glimpsed the main ones, big and small.
The one point is what it was at the beginning. Each kind of kidney stone has its own ways, and treatment requires we know which one you have.
Likewise, for whatever that one may be, it is good to know as much about it as you can know. For long term prevention of stones is hard to come by and ultimately what the patience and and consistency of patients themselves matters most.
If you don’t know which stones you have made, find out.
Track down old reports and pull them together.
Keep copies and send everything to the doctors who care for you.
Fred Coe MD
my MRI Report says its 1.5mm Cystine-Struvite stone.
Any explanation?
Hi Meski, Cystine is a very special kind of stone, so is struvite. I did not think MRI could do this kind of stone type estimates, and suspect you mean CT scan. A 1.5 mm stone is very small, and I frankly doubt the validity of the report. You should ask your personal physician if he/she is any more convinced than I am. Regards, Fred Coe
My stone analysis was 100% phosphate. Is this treatable?…
Hi Connie, They certainly are. Here is your type of stone former. You should expect excellent prevention outcomes with proper evaluation and treatment. Regards, Fred Coe
My stone analysis was 100% phosphate. Is this treatable?…
Hi Connie, They certainly are. Here is your type of stone former. You should expect excellent prevention outcomes with proper evaluation and treatment. Regards, Fred Coe
Just got my stone analysis report back. Calcium Oxalate Dihydrate (Weddellite) 50% Carbonate Apatite (Dahllite) 50%. What type of stone former does this make me? Thank you for your knowledge and time!
Hi Cynthia, it is a common stone often due to high urine calcium. Be sure and get properly evaluated as to its cause and seek prevention against more. Regards, Fred Coe
Just got my stone analysis report back. Calcium Oxalate Dihydrate (Weddellite) 50% Carbonate Apatite (Dahllite) 50%. What type of stone former does this make me? Thank you for your knowledge and time!
Hi Cynthia, it is a common stone often due to high urine calcium. Be sure and get properly evaluated as to its cause and seek prevention against more. Regards, Fred Coe
My dr. just looked at my stone and said “with out a doubt that’s a oxalate stone”. Should I just pay to have it tested myself (assuming I can do that)?
Hi Jennifer, I would certainly ask it be analysed. Your physician may well be right, but the analysis is not overly expensive, and will certainly disclose the full composition. I have a lot of personal experience and would not want to rely on my two eyes when I can get a more exact analysis easily and affordably. Regards, Fred Coe
My dr. just looked at my stone and said “with out a doubt that’s a oxalate stone”. Should I just pay to have it tested myself (assuming I can do that)?
Hi Jennifer, I would certainly ask it be analysed. Your physician may well be right, but the analysis is not overly expensive, and will certainly disclose the full composition. I have a lot of personal experience and would not want to rely on my two eyes when I can get a more exact analysis easily and affordably. Regards, Fred Coe
My current stone anayisis:
Ammonium acid urate 15%
Ca oxalate monohydrate 48%
Calcium phosphate 35%
Compared to 2018
Calcium phosphate 9%
Ca oxalate monohydrate 90%
Why such a change? I need a neurologist my urologist just keeps taking me in for procedures and this last one has had horrible complications
Autocorrect 🙁. NEPHROLOGIST
Hi Ryan, This progression to more phosphate is not rare and reflects a rise in urine pH. Check you your 24 hour urine samples and look for it. In other cases, urine pH is high right at the start – high is above 6.2 on a 24 hour basis. In any event the correct approach is prevention. Here is a good article I like for its detail work. See where you might fit into. Regards, Fred Coe
After disabled adult son, who is diagnosed with gout, complained of left flank pain, several renal ultrasounds show calcium stone on kidney. The next step was CT scans, a few over 6 months, which showed no stone. Would uric acid stones appear in US and not a CT? (Can’t do MRI due to ICD) Thank you!
Hi Cathy, CT scans are near 100% sensitive and selective for stones. Ultrasound is only about 55% sensitive and 60% selective. So I would believe the CT. Regards, Fred Coe
After disabled adult son, who is diagnosed with gout, complained of left flank pain, several renal ultrasounds show calcium stone on kidney. The next step was CT scans, a few over 6 months, which showed no stone. Would uric acid stones appear in US and not a CT? (Can’t do MRI due to ICD) Thank you!
Hi Cathy, CT scans are near 100% sensitive and selective for stones. Ultrasound is only about 55% sensitive and 60% selective. So I would believe the CT. Regards, Fred Coe
Thank you for the great article.
I’ve been in ongoing treatment for a 19mm stone and smaller fragments since mid June of this year. I’ll undergo a second lithotripsy in two days from now.
My stones are 1% calcium oxalate monohydrate, and 99% calcium phosphate (apatite). The shell is similar: 3% : 97%
My question is the my doctor said these are primarily caused from repeated UTIs, and I don’t see this in your explanation.
So I’m wondering whether he is thinking of a different type stone?
Or, does a UTI create the alkaline environment needed for the stones to form??
Many thanks!
Hi Maria, I doubt that your calcium phosphate stones are from infection. Infection produces struvite stones – magnesium ammonium phosphate. Most people with calcium phosphate stones are women, and have an alkaline urine and high urine calcium. Here is an article about them. You need blood and 24 hour testing to figure out what causes your stones, and then treatment to reverse those causes. Regards, Fred Coe
Thank you for the great article.
I’ve been in ongoing treatment for a 19mm stone and smaller fragments since mid June of this year. I’ll undergo a second lithotripsy in two days from now.
My stones are 1% calcium oxalate monohydrate, and 99% calcium phosphate (apatite). The shell is similar: 3% : 97%
My question is the my doctor said these are primarily caused from repeated UTIs, and I don’t see this in your explanation.
So I’m wondering whether he is thinking of a different type stone?
Or, does a UTI create the alkaline environment needed for the stones to form??
Many thanks!
Hi Maria, I doubt that your calcium phosphate stones are from infection. Infection produces struvite stones – magnesium ammonium phosphate. Most people with calcium phosphate stones are women, and have an alkaline urine and high urine calcium. Here is an article about them. You need blood and 24 hour testing to figure out what causes your stones, and then treatment to reverse those causes. Regards, Fred Coe
Thank you!
Hiii sir my impression is hydro uritoronephrosis….. what is my position and what should i do.. in left kidney….
Hi Satwuk, The words mean obstruction of a kidney and you must have a physician caring for you. He/she is responsible for fixing the drainage system if necessary. You yourself can do nothing. Regards, Fred Coe
Hiii sir my impression is hydro uritoronephrosis….. what is my position and what should i do.. in left kidney….
Hi Satwuk, The words mean obstruction of a kidney and you must have a physician caring for you. He/she is responsible for fixing the drainage system if necessary. You yourself can do nothing. Regards, Fred Coe
Hi! I’m a recurrent stone former. My most recent report shows the following:
35% CaOx Dihydrate
50% CaOx Monohydrate
15% Ca phosphate
I see a lot of info with a mix of COM/COD, others with COM or COD with CaPh, but I can’t find much with all 3. What type of stone former would all 3 be?
Hi AmyA, your stones are made of two types of calcium oxalate admixed with calcium phosphate and are common. You are a calcium oxalate stone former. The causes are the usual ones, and you are best served by blood and 24 hour urine testing to find the cause and treat it. Regards, Fred Coe
Hi! I’m a recurrent stone former. My most recent report shows the following:
35% CaOx Dihydrate
50% CaOx Monohydrate
15% Ca phosphate
I see a lot of info with a mix of COM/COD, others with COM or COD with CaPh, but I can’t find much with all 3. What type of stone former would all 3 be?
Hi AmyA, your stones are made of two types of calcium oxalate admixed with calcium phosphate and are common. You are a calcium oxalate stone former. The causes are the usual ones, and you are best served by blood and 24 hour urine testing to find the cause and treat it. Regards, Fred Coe
I have stones both side of my kidney. The sizes are 1.2cm and 1.0 cm based on the ultrasound and ct scan result but aside from stones i also have systs on both sides, my family has a history of kidney stones so i think that my stones are cystine type. But i want to be sure, what tests should be done and what kind of specealist do i have to consult in order to surely identify the type of the kidney stone i have and does my systs affect the stones?
Hi Mac-jay, Stone analysis is best – cystine is easy to recognize. Urine screening testing for cystine is cheap and everyone can do it. It is essential to know because cystine stones can be very large and affect kidney function adversely. Regards, Fred Coe
I have stones both side of my kidney. The sizes are 1.2cm and 1.0 cm based on the ultrasound and ct scan result but aside from stones i also have systs on both sides, my family has a history of kidney stones so i think that my stones are cystine type. But i want to be sure, what tests should be done and what kind of specealist do i have to consult in order to surely identify the type of the kidney stone i have and does my systs affect the stones?
Hi Mac-jay, Stone analysis is best – cystine is easy to recognize. Urine screening testing for cystine is cheap and everyone can do it. It is essential to know because cystine stones can be very large and affect kidney function adversely. Regards, Fred Coe
My stones are 100% carbonate apotite dahllite I just got the result the urologyst said it is extremely rare and send me to a endocrinologist internist I have no idea what that means (the result) but I can tell you in just 24 days I calcify the catheter they put inside and they remove more than 30 stones
Hi Lucrecia, What the stone means is that it is a form of calcium phosphate and such crystals form when urine pH is high and usually urine calcium, as well. It is not so rare as it is less common. You need full serum and 24 hour urine testing to figure out why you form the stones and then prevention aimed at the results. There is no guesswork involved, just testing and treatment based on the results. Regards, Fred Coe
My stones are 100% carbonate apotite dahllite I just got the result the urologyst said it is extremely rare and send me to a endocrinologist internist I have no idea what that means (the result) but I can tell you in just 24 days I calcify the catheter they put inside and they remove more than 30 stones
Hi Lucrecia, What the stone means is that it is a form of calcium phosphate and such crystals form when urine pH is high and usually urine calcium, as well. It is not so rare as it is less common. You need full serum and 24 hour urine testing to figure out why you form the stones and then prevention aimed at the results. There is no guesswork involved, just testing and treatment based on the results. Regards, Fred Coe
Thank you for your article! I have been told that I have an egfr of 53 and high creatinine. I looked back and my gfr has been dropping for about three years from a high of 136 in years before that. My Endo ordered a sonogram of my kidneys that didn’t show anything and a 24hr urine that showed raised pH and brushite. I can’t see a specialist until Dec and my neurologist said that my topamax wouldn’t cause kidney failure or crystals.(through a phone message with his office). Needles to say, I am scared to death to wait that long and your article is the only thing that I have found that helps me understand. Can you please give me advice on the most important things besides sodium that I can cut from my diet so that I can try to stay syonr free until I can get all of this addressed. Thank you!
Hi Sylvia, I gather that while taking Topamax your renal function has declined and that your urine shows the expected high urine pH and urine calcium from the drug or perhaps hereditary and worsened by the drug. You may have multiple renal crystal deposits, and only a CT can visualize them; ultrasound has a sensitivity to stones of about 55%. An ultra low dose CT has very little radiation dose and will tell if there are indeed stones. I would be concerned about crystal deposits as a cause of kidney function loss, and perhaps your physicians can pursue this matter. Diet will be of little effect given the drug, and there would be some urgency to figure out its role, if any, in the loss of function. Regards, Fred Coe
Thank you for your article! I have been told that I have an egfr of 53 and high creatinine. I looked back and my gfr has been dropping for about three years from a high of 136 in years before that. My Endo ordered a sonogram of my kidneys that didn’t show anything and a 24hr urine that showed raised pH and brushite. I can’t see a specialist until Dec and my neurologist said that my topamax wouldn’t cause kidney failure or crystals.(through a phone message with his office). Needles to say, I am scared to death to wait that long and your article is the only thing that I have found that helps me understand. Can you please give me advice on the most important things besides sodium that I can cut from my diet so that I can try to stay syonr free until I can get all of this addressed. Thank you!
Just got my path report of a kidney stone removed in surgery. It states Cal Oxalate Dihydrate 40%, Cal Oxalate Monohydrate 40%, Carbonate Apatite 20%. What does this mean for me?
Hi Glenice, It means you have the common calcium stones and need prevention. Here is a very good place to start. Regards, Fred Coe
Just got my path report of a kidney stone removed in surgery. It states Cal Oxalate Dihydrate 40%, Cal Oxalate Monohydrate 40%, Carbonate Apatite 20%. What does this mean for me?
Hi Glenice, It means you have the common calcium stones and need prevention. Here is a very good place to start. Regards, Fred Coe
I have a long history of kidney stones. My most recent stone was analyzed at 10% calcium oxalate/ 80% calcium monohydrogen phosphate dihydrate (brushite), and 10% calcium phosphate. I have yet to be able to prevent stone formation. With this stone makeup, what are your thoughts on why I’m getting them and how to avoid getting them? Thanks
Hi Jamie, brushite stones are a big problem. The reason for them is a mix of high urine calcium and usually high urine pH. Treatment is like for calcium oxalate stones but more urgent. Here is an outline of what is needed. They can be made to stop, but all the details need to be attended to – see the link. Regards, Fred Coe
I have a long history of kidney stones. My most recent stone was analyzed at 10% calcium oxalate/ 80% calcium monohydrogen phosphate dihydrate (brushite), and 10% calcium phosphate. I have yet to be able to prevent stone formation. With this stone makeup, what are your thoughts on why I’m getting them and how to avoid getting them? Thanks
Hi Jamie, brushite stones are a big problem. The reason for them is a mix of high urine calcium and usually high urine pH. Treatment is like for calcium oxalate stones but more urgent. Here is an outline of what is needed. They can be made to stop, but all the details need to be attended to – see the link. Regards, Fred Coe
My father had “stones” removed last year. He had no past medical history of stones prior to 5/2018 and never appeared to be in any pain. His Nephro/Uro Doc removed 75% of the stones, placed a stent in a ureter? or the urethra. Post-procedure pain was his only reported discomfort. In 9/2019 his hemoglobin was low(7) and on examination, the stones were back. We discovered that the low hemoglobin was volume loss from an undiagnosed duodenal bleed (for which he had been flushing diarrhea for months.)
For obvious reasons, I never asked about the specifics because in general, Men don’t talk about below the waist issues with women, especially with his daughter. My question to you all is, which type of stones could he have had that never caused pain? Could stones be related to diarrhea/black tarry stools as a result of the GI bleed that lowered his Heme levels? When he went to a new doc I asked if his ureter stent could be causing a blockage. Uroteam and Radiology replied: “What stent? He doesn’t have any.” Is it common for stents in urethra or ureter to migrate or be passed in the urine? Thanks.
Hi Marie, Stents are in the ureter and I must presume it had been removed prior to the new imaging. GI bleed is not a specific reason for stones but dehydration from diarrhea certainly is. What matters here is what the stones are made of – I might guess uric acid. And then, what caused them. That is a lot, and here is a decent place to begin learning so you can help your dad. Regards, Fred Coe
My father had “stones” removed last year. He had no past medical history of stones prior to 5/2018 and never appeared to be in any pain. His Nephro/Uro Doc removed 75% of the stones, placed a stent in a ureter? or the urethra. Post-procedure pain was his only reported discomfort. In 9/2019 his hemoglobin was low(7) and on examination, the stones were back. We discovered that the low hemoglobin was volume loss from an undiagnosed duodenal bleed (for which he had been flushing diarrhea for months.)
For obvious reasons, I never asked about the specifics because in general, Men don’t talk about below the waist issues with women, especially with his daughter. My question to you all is, which type of stones could he have had that never caused pain? Could stones be related to diarrhea/black tarry stools as a result of the GI bleed that lowered his Heme levels? When he went to a new doc I asked if his ureter stent could be causing a blockage. Uroteam and Radiology replied: “What stent? He doesn’t have any.” Is it common for stents in urethra or ureter to migrate or be passed in the urine? Thanks.
Hi Marie, Stents are in the ureter and I must presume it had been removed prior to the new imaging. GI bleed is not a specific reason for stones but dehydration from diarrhea certainly is. What matters here is what the stones are made of – I might guess uric acid. And then, what caused them. That is a lot, and here is a decent place to begin learning so you can help your dad. Regards, Fred Coe
I had three procedures last month to get rid of a 15mm stone that was finally broken down and pieces individually removed with what I believe they called a basket procedure. (I had lithotripsy and ESWOL with stent placement, all three procedures within two weeks time.). I went for follow up U/S today and there is now a cyst in my right kidney, where the 15mm perpetrator formed, and four more stones on the left, thankfully only 4mm. My stone evaluation was also detailed today and was 50% calcium oxalate dihydrate and 50% carbapatite (Weddellite and Dahllite). I had most of my thyroid removed in 2012 due to a five inch footer that extended down beneath my collarbone and displacing my trachea. I’m on both T3 and T4 now for hypothyroidism. My question is: Does this make it likely that I have hyperparathyroidism causing these stones? Could the thyroid surgery have affected my parathyroid? I do plan to see my PCP ASAP but it will probably be December before I can get in so I was hoping you could give me some information from the analysis. Thank you!
Jennifer
Hi Jennifer, Your stone has considerable phosphate, and poses special problems. PHPT is diagnosed from fasting serum calcium levels, and as part of your evaluation for causes of stones is always an important possibility. Given you have multiple stones, full evaluation is paramount, and I am sure the 24 hour urines and serums – be sure they are fasting! – can be ordered in advance of your visits so the visits are best used. Regards, Fred Coe
I had three procedures last month to get rid of a 15mm stone that was finally broken down and pieces individually removed with what I believe they called a basket procedure. (I had lithotripsy and ESWOL with stent placement, all three procedures within two weeks time.). I went for follow up U/S today and there is now a cyst in my right kidney, where the 15mm perpetrator formed, and four more stones on the left, thankfully only 4mm. My stone evaluation was also detailed today and was 50% calcium oxalate dihydrate and 50% carbapatite (Weddellite and Dahllite). I had most of my thyroid removed in 2012 due to a five inch footer that extended down beneath my collarbone and displacing my trachea. I’m on both T3 and T4 now for hypothyroidism. My question is: Does this make it likely that I have hyperparathyroidism causing these stones? Could the thyroid surgery have affected my parathyroid? I do plan to see my PCP ASAP but it will probably be December before I can get in so I was hoping you could give me some information from the analysis. Thank you!
Jennifer
I HAD A 24 HOUR SUPERSTATPROFILE OF MY URINE AND EVERY CRYSTAL WAS LOW OR IN THE NORMAL RANGE EXCEPT HYDROXYAPATITE CRYSTAL WHICH WAS HIGH AT 4.42 DG REFERENCE RANGE WAS 3.96 DG. SHOULD I BE WORRIED
Hi Keith, These SS values are not helpful taken in a vacuum. What kind of stone did your form, calcium oxalate or calcium phosphate? What is abnormal in your urine beside the HA SS? If you provide more, I can try to be helpful. Regards, Fred Coe
I HAD A 24 HOUR SUPERSTATPROFILE OF MY URINE AND EVERY CRYSTAL WAS LOW OR IN THE NORMAL RANGE EXCEPT HYDROXYAPATITE CRYSTAL WHICH WAS HIGH AT 4.42 DG REFERENCE RANGE WAS 3.96 DG. SHOULD I BE WORRIED
Hi Keith, These SS values are not helpful taken in a vacuum. What kind of stone did your form, calcium oxalate or calcium phosphate? What is abnormal in your urine beside the HA SS? If you provide more, I can try to be helpful. Regards, Fred Coe
Hi i have stone issue since 10 years or more. every after 8 to 9 months i have to face this problem, stone type is calcium oxalate with the ratio of 30/70. usually stone size is about 2 to 3 mm but this time it was 11.4mm. and off-course that was alarming. but after some medicine treatment it is broken and released. please pass any suggestion to prevent in future. or should i share my medical examination history.
Hi Minhass Ali, I guess this whole site is about prevention. Here is a very good place to begin. Regards, Fred Coe
Hi i have stone issue since 10 years or more. every after 8 to 9 months i have to face this problem, stone type is calcium oxalate with the ratio of 30/70. usually stone size is about 2 to 3 mm but this time it was 11.4mm. and off-course that was alarming. but after some medicine treatment it is broken and released. please pass any suggestion to prevent in future. or should i share my medical examination history.
Hi Minhass Ali, I guess this whole site is about prevention. Here is a very good place to begin. Regards, Fred Coe
I had Lithotripsy on Oct 24th. This is my stone analysis: 66% calcium oxalate monohydrate: 30% calcium oxalate dihydrate; 2% calcium phosphate (hydroxyl form); 2% protein. My calcium & magnesium were high & out of range on my 24 hour urinalysis, everything else was in range. My blood test showed everything normal with no parathyroid indications. I would appreciate your advice. I also have osteoporosis, so I take 1000 mg of calcium plant based daily & D-3 4000 IU.my Urologist said I absolutely need to adhere to a low oxalate diet.
Hi Ellie, You have a high urine calcium and apparently normal blood calcium, and bone disease. I believe you have idiopathic – familial – hypercalciuria. This condition causes stones and bone disease and is treated with diet and if needed with meds. This article details treatment and clinical evaluation. Diet oxalate seems irrelevant if urine oxalate is not high and urine calcium is very high. I would suggest mentioning this to your physicians to see if they are in accord. By all means, they are responsible for your care and may know things you have not mentioned in your note. Regards, Fred Coe
I had Lithotripsy on Oct 24th. This is my stone analysis: 66% calcium oxalate monohydrate: 30% calcium oxalate dihydrate; 2% calcium phosphate (hydroxyl form); 2% protein. My calcium & magnesium were high & out of range on my 24 hour urinalysis, everything else was in range. My blood test showed everything normal with no parathyroid indications. I would appreciate your advice. I also have osteoporosis, so I take 1000 mg of calcium plant based daily & D-3 4000 IU.my Urologist said I absolutely need to adhere to a low oxalate diet.
Hi Ellie, You have a high urine calcium and apparently normal blood calcium, and bone disease. I believe you have idiopathic – familial – hypercalciuria. This condition causes stones and bone disease and is treated with diet and if needed with meds. This article details treatment and clinical evaluation. Diet oxalate seems irrelevant if urine oxalate is not high and urine calcium is very high. I would suggest mentioning this to your physicians to see if they are in accord. By all means, they are responsible for your care and may know things you have not mentioned in your note. Regards, Fred Coe
Hello Dr Coe,
My urine tests show alkaline ph and high phosphates. I’ve been eating a plant-based vegan diet recently, drinking mostly water. I am confused by how I can correct my diet to make my urine less alkaline and to lower the level of phosphates. What I am finding on the internet is that most of the plant-based foods are alkalizing. Should I eat more grains and drink tea/coffee? Thank you!
Hi Anna, It is true that plants contain a lot of alkali. But do you have more than high pH? For example, is your urine calcium high. One really treats the ensemble of abnormalities. Are your stones calcium phosphate? If you provide more information I can try to help more. Here is a good introduction to the problem of prevention. Regards, Fred Coe
Hello Dr Coe,
My urine tests show alkaline ph and high phosphates. I’ve been eating a plant-based vegan diet recently, drinking mostly water. I am confused by how I can correct my diet to make my urine less alkaline and to lower the level of phosphates. What I am finding on the internet is that most of the plant-based foods are alkalizing. Should I eat more grains and drink tea/coffee? Thank you!
I have images and a collection of rare kidney stones I produce daily.
Hi Aaron, I am sorry you form so many stones, and rare ones at that. If you wish to share details perhaps there are ways to help prevent them. Regards, Fred Coe
I have images and a collection of rare kidney stones I produce daily.
Hi Aaron, I am sorry you form so many stones, and rare ones at that. If you wish to share details perhaps there are ways to help prevent them. Regards, Fred Coe
Hi Dr. Coe, I had a kidney stone removed via laser last week and a Stent placed in because I have several more in the kidney (s). The stone analysis results came back as unknown constituents after repeated analysis. Is this common? All I know is the Dr. Said it was a soft material. But without knowing what they are made of I am sort of left in limbo in terms of prevention.
Hi Eric, Not a total loss. Since CT scans show stones in your kidneys, your physician can measure the radiographic density of the stones. Low values suggest uric acid high values calcium based stones. As for unknown constituents, that is not an acceptable lab report and suggests the lab is inferior in quality. The technology of infrared spectral analysis usually can identify crystals of all kinds. Perhaps the report is that there are no crystals, making the stones mainly protein. But such stones will not show up on a CT, as one does need some heavy atoms to retard the radiation. I would find out the radiographic density, and work from there. Regards, Fred Coe
Thank you so much Dr. Coe. I had a CT scan at the ER. They said I had several stones in both kidneys. My urologist did a Diag-ABDOMEN-AP VIEW Details Impression: “No densely calcified urolithiasis identified.” Their was a DIAG-FLUORO SVCS IN SURGERY-Details Impression: Fluro time=0 minutes 35 seconds, “no component information for this result” POCT AMB URINE DIPSTICK -Details Color yellow, Clarity clear, Glucose negative, Bilirubin negative, Ketones negative, Spec Grav 1.020, Blood negative, pH 7.0, Protein negative, Urobilinogen 1.0, leukocytes negative. KIDNEY STONE ANALYSIS: “kidney stone (N20.0) Hydronephrosis of right kidney (N13.30) Nidus not observed, After repeated analysis, we were unable to identify the constituents of this material. Test performed by Quest Diagnostics. I go back in Tuesday to have the stent removed and I hope they explain more to me than what they have so far, I am kind of hanging in limbo for the time being until they tell me what the next plan of action will be since this type of stone doesn’t appear to be run of the mill stones. I have learned for more from you, so thank you!
Hi Eric, As I mentioned, the radiographic density of stones from the CT can give a clue as to whether the stones are uric acid or calcium based. The abdominal – AP view is very insensitive to stones, and one cannot rely on it. Of course the fluoroscopy was not meant to specifically identify stones but to aid in the surgery. Regards, Fred Coe
Hi Dr. Coe, I had a kidney stone removed via laser last week and a Stent placed in because I have several more in the kidney (s). The stone analysis results came back as unknown constituents after repeated analysis. Is this common? All I know is the Dr. Said it was a soft material. But without knowing what they are made of I am sort of left in limbo in terms of prevention.
Hi Eric, Not a total loss. Since CT scans show stones in your kidneys, your physician can measure the radiographic density of the stones. Low values suggest uric acid high values calcium based stones. As for unknown constituents, that is not an acceptable lab report and suggests the lab is inferior in quality. The technology of infrared spectral analysis usually can identify crystals of all kinds. Perhaps the report is that there are no crystals, making the stones mainly protein. But such stones will not show up on a CT, as one does need some heavy atoms to retard the radiation. I would find out the radiographic density, and work from there. Regards, Fred Coe
Thank you so much Dr. Coe. I had a CT scan at the ER. They said I had several stones in both kidneys. My urologist did a Diag-ABDOMEN-AP VIEW Details Impression: “No densely calcified urolithiasis identified.” Their was a DIAG-FLUORO SVCS IN SURGERY-Details Impression: Fluro time=0 minutes 35 seconds, “no component information for this result” POCT AMB URINE DIPSTICK -Details Color yellow, Clarity clear, Glucose negative, Bilirubin negative, Ketones negative, Spec Grav 1.020, Blood negative, pH 7.0, Protein negative, Urobilinogen 1.0, leukocytes negative. KIDNEY STONE ANALYSIS: “kidney stone (N20.0) Hydronephrosis of right kidney (N13.30) Nidus not observed, After repeated analysis, we were unable to identify the constituents of this material. Test performed by Quest Diagnostics. I go back in Tuesday to have the stent removed and I hope they explain more to me than what they have so far, I am kind of hanging in limbo for the time being until they tell me what the next plan of action will be since this type of stone doesn’t appear to be run of the mill stones. I have learned for more from you, so thank you!
Hi Eric, As I mentioned, the radiographic density of stones from the CT can give a clue as to whether the stones are uric acid or calcium based. The abdominal – AP view is very insensitive to stones, and one cannot rely on it. Of course the fluoroscopy was not meant to specifically identify stones but to aid in the surgery. Regards, Fred Coe
Dr Coe,
I am currently stone free – with a history of multiple calcium oxalate stones. (IH) all removed a year and a half ago. I’m on Moduretic 5-50 one a day.
I use litholink for my 24 urines.
Here is my question. I feel my risk for calcium oxalate is relatively low now but I worry that I have an increased risk of calcium phosphate stones based on a high urinary ph. I will give all my numbers below but is there a dietary change I can make to lower my urine ph? I have a banana and apple a day. Melons when they are in season. I don’t eat a lot of meat but 4oz when I do. And I drink 8 oz milk twice a day and liquid yogurt once a day. My fluids per day are over 3 liters.
Vol- 4.06
SS CaOx – 1.87
Urine calcium- 243
Urine oxalate – 23
Urine citrate- 1006
SSCaP- 1.20
24 hr urine pH – 7.022
SS Uric acid – 0.04
Urine uric acid – 0.663
Thanks!
Julie
Dr Coe,
I am currently stone free – with a history of multiple calcium oxalate stones. (IH) all removed a year and a half ago. I’m on Moduretic 5-50 one a day.
I use litholink for my 24 urines.
Here is my question. I feel my risk for calcium oxalate is relatively low now but I worry that I have an increased risk of calcium phosphate stones based on a high urinary ph. I will give all my numbers below but is there a dietary change I can make to lower my urine ph? I have a banana and apple a day. Melons when they are in season. I don’t eat a lot of meat but 4oz when I do. And I drink 8 oz milk twice a day and liquid yogurt once a day. My fluids per day are over 3 liters.
Vol- 4.06
SS CaOx – 1.87
Urine calcium- 243
Urine oxalate – 23
Urine citrate- 1006
SSCaP- 1.20
24 hr urine pH – 7.022
SS Uric acid – 0.04
Urine uric acid – 0.663
Thanks!
Julie
Hi Julie, There is no way to lower urine pH without causing more problems, but your SS values are low enough I might not worry. Urine calcium remains a bit high and you do not quote urine sodium. I would try to reduce the latter to 1500 mg (65 mEq)/day which may make the final difference in your CaP SS. Regards, Fred Coe
What can I eat with this diagnosis of my recent surgical procedure…
I REALLY want to get this under control… It is my life .. .. ..
Results from procedure : : :
60% Calcium phosphate (apatite)
30% Calcium oxalate monohydrate
10% Calcium oxalate dihydrate
Please advise as I do not want to be where I was once again as an emergency patient…
Thank-you very much
Hi Carah, Your main stone component is calcium phosphate, and I suspect your main problems are not urine oxalate but rather high urine pH and calcium, and perhaps also low urine volume. You do not mention your 24 hour urine values, but I presume you have been properly evaluated. Here is a good place to start and be sure what has been done and what is known about you so far. Regards, Fred Coe
What can I eat with this diagnosis of my recent surgical procedure…
I REALLY want to get this under control… It is my life .. .. ..
Results from procedure : : :
60% Calcium phosphate (apatite)
30% Calcium oxalate monohydrate
10% Calcium oxalate dihydrate
Please advise as I do not want to be where I was once again as an emergency patient…
Thank-you very much
Hi Carah, Your main stone component is calcium phosphate, and I suspect your main problems are not urine oxalate but rather high urine pH and calcium, and perhaps also low urine volume. You do not mention your 24 hour urine values, but I presume you have been properly evaluated. Here is a good place to start and be sure what has been done and what is known about you so far. Regards, Fred Coe
Sorry corrected versuon, Hello, I had an 11mm stone remove with , I am 45 and this is my first, this is what shown in my scans, There is an 11 x 10 x 7 mm nonobstructing left lower pole renal stone. nonspecific 1.5 cm left adrenal nodule which is incompletely characterized on this postcontrast study. However, there is mild left hydronephrosis and peripelvic fat stranding. No ureteral stone is currently present to account for this. 40% Calcium oxalate monohydrate
40% Calcium oxalate dihydrate
20% Calcium phosphate (apatite),. I also was diagnosed with NASH, mild iron in my liver and HyperPortal tension,. They are triing to figure out my high bilerubin and ferritin and high blood pressure. They did find mild iron in my liver. Can this all be related to the nodule. Also any advice would help, and if you can tell me about my stone computition, I also have high blood pressure….. Thank so much. They say I’m a mystery….I’m don’t like being a mystery…
Hi Mike, The stone is commonplace and often arises because of high urine calcium or oxalate – or both, low volume or citrate. I am not expert in liver disease and cannot offer any opinion. The hypertension could be from primary aldosteronism but usually serum potassium is low. A form of hemochromatosis is obviously being considered by your physicians. I forgot if you are being cared for at a university medical center. If not, you should be as your problem is far outside the commonplace. A mere adrenal nodule is often not functional, so its being there raises suspicion. Specific treatment against high aldosterone might lower your blood pressure, a useful therapeutic test. Of course, I presume your aldosterone levels and corticoid levels have been measured already. Regards, Fred Coe
Thank you for comments back, the University doctor didn’t offer alot in diagnoses but rather seem to be studying me. I do not think they looked at my aldosterone or corticoid level, I will ask,. They did a Hemochromatosis test that said neg. What should I ask them about the adrenal nodule, they never mentioned it, I just seen it on my report…..thank you for all the help..
Sorry corrected versuon, Hello, I had an 11mm stone remove with , I am 45 and this is my first, this is what shown in my scans, There is an 11 x 10 x 7 mm nonobstructing left lower pole renal stone. nonspecific 1.5 cm left adrenal nodule which is incompletely characterized on this postcontrast study. However, there is mild left hydronephrosis and peripelvic fat stranding. No ureteral stone is currently present to account for this. 40% Calcium oxalate monohydrate
40% Calcium oxalate dihydrate
20% Calcium phosphate (apatite),. I also was diagnosed with NASH, mild iron in my liver and HyperPortal tension,. They are triing to figure out my high bilerubin and ferritin and high blood pressure. They did find mild iron in my liver. Can this all be related to the nodule. Also any advice would help, and if you can tell me about my stone computition, I also have high blood pressure….. Thank so much. They say I’m a mystery….I’m don’t like being a mystery…
Hi Mike, The stone is commonplace and often arises because of high urine calcium or oxalate – or both, low volume or citrate. I am not expert in liver disease and cannot offer any opinion. The hypertension could be from primary aldosteronism but usually serum potassium is low. A form of hemochromatosis is obviously being considered by your physicians. I forgot if you are being cared for at a university medical center. If not, you should be as your problem is far outside the commonplace. A mere adrenal nodule is often not functional, so its being there raises suspicion. Specific treatment against high aldosterone might lower your blood pressure, a useful therapeutic test. Of course, I presume your aldosterone levels and corticoid levels have been measured already. Regards, Fred Coe
Thank you for comments back, the University doctor didn’t offer alot in diagnoses but rather seem to be studying me. I do not think they looked at my aldosterone or corticoid level, I will ask,. They did a Hemochromatosis test that said neg. What should I ask them about the adrenal nodule, they never mentioned it, I just seen it on my report…..thank you for all the help..
My husband recently had a kidney stone removed, 8mm, 80% uric acid and 20% calcium oxalate. Any suggestions? Should he focus on increasing alkali in his urine?
Hi Sheila, He should. Here is a good article on uric acid stones, they can be prevented completely and he should do that. Regards, Fred Coe
My husband recently had a kidney stone removed, 8mm, 80% uric acid and 20% calcium oxalate. Any suggestions? Should he focus on increasing alkali in his urine?
Hi Sheila, He should. Here is a good article on uric acid stones, they can be prevented completely and he should do that. Regards, Fred Coe