
 I love the blurry pixillated image of OTC medication crowded onto shelves. Somehow it conveys armies of hopefuls pushing forward into the harried buyer who wants a remedy. The title points to 9 hopefuls for kidney stone prevention.
I love the blurry pixillated image of OTC medication crowded onto shelves. Somehow it conveys armies of hopefuls pushing forward into the harried buyer who wants a remedy. The title points to 9 hopefuls for kidney stone prevention.
WHAT AM I OFFERING?
My friends at the kidney stone center at University of Texas Southwestern Medical School just published a wonderful paper detailing just how much citrate alkali is in each of the current OTC remedies, and I want to bring their work to all of you who read this site.
Some OTC Remedies Contain Two Alkali
All of the remedies contain some alkali as citrate. Potassium citrate tablets, the standard medically prescribed alkali tested in trials against stone formation, are only potassium citrate. In some OTC products some alkali comes not from citrate, but also from bicarbonate.
Citrate produces new bicarbonate in the blood as it is metabolized by cells. That is a process that takes some time. Bicarbonate is the prime alkali in blood and acts as soon as it is absorbed by the GI tract. So for a given amount of alkali the two forms will produce a different time pattern of urine pH and perhaps citrate – Citrate being presumably more stable, bicarbonate more peaks and valleys.
The Two Alkali May Not Confer Equal Protection
The 24 hour urine stone risk will not disclose whether the alkali has been steady or spiky. All it can tell us is the average for the 24 hours. This is the same limitation we face for fluids, calcium, even supersaturation.
But – that word! – we have no trials for sodium or potassium bicarbonate as stone prevention, only potassium citrate. The peaks and valleys might compromise protection. The Dallas article, by purifying the alkali measurement, literally begs the obvious question. Could simple potassium bicarbonate prevent stones? So inexpensive an agent, were it effective, would surely benefit all stone formers who could benefit from alkali. That remains for some future research.
The Benefits of Alkali
As I detail below, there are two. If urine pH needs raising, as in uric acid stone formers, these products may well be sufficient – dosage is not as simple as with prescribed K citrate, a matter noted in the individual product reviews. Alkali can raise urine citrate excretion, the other benefit. How and to what end is discussed below.
Why, then, put this here?
Because at least one person, highly educated, did not notice the citrate effect, and therefore it needs repeating.
THE PRODUCTS
Their Names
First, the proper names of each one: Moonstone® Powder; Litholyte® Powder; Litholyte® Coffee; Kidney COP®; KSP tabsTM; LithoBalanceTM; NOW® Potassium Citrate; Horbaach® Potassium Citrate; TheraLith XR®. With apologies, but understandably, I abbreviate their names here (In order of their proper names): MSP; LLP; LLC; KCOP; KSP; LB; NOWPC; HORPC; TLY.
What They Can Do
Lets be clear. All of them have only one established medical benefit for kidney stone disease – alkali. Alkali when absorbed or when produced by metabolism of citrate, signals the citrate transporter to release into the urine citrate that has been filtered at the glomerulus. The linked article details citrate regulation and how potassium citrate pills – the conventional prescribed form of alkali – work.
The nine remedies reviewed here were created to achieve results like those of medicinal potassium citrate. Unlike potassium citrate, none of these remedies have ever been tried as stone preventions. The link takes you to trials showing that medicinal potassium citrate can prevent kidney stones. Instead these remedies rely on a reasonable logic: Potassium citrate prevents stones by raising urine citrate; equivalent amounts of alkali from a remedy that has no trial can increase urine citrate; therefore such a remedy should be able to prevent stones.
Put another way, there is no reason to doubt that an equivalent amount of alkali from one of these remedies will raise urine citrate to the same extent as an equal amount of alkali from potassium citrate itself. But given some contain two kinds of alkali, and given most contain more than potassium citrate, we cannot know if they are effective against stones.
CITRATE ALKALI IN THE NINE REMEDIES
Citric Acid vs. Citrate
An enormous service from Dallas was to measure how much citrate alkali a serving of each remedy provides. The amount of citric acid in a a serving gives no clue to the amount of alkali. If the product is very acid – has a low pH when dissolved in water or taken orally – most of the citric acid has its protons, and when metabolized produces no new alkali. If the product has a high pH, most of the citric acid lacks its protons (citric acid has three proton acceptor sites). It can only be metabolized with its protons, so metabolism takes up protons from the blood buffers, producing bicarbonate alkali. (I used a link to a sophisticated article that has a lot about alkali.) It is best to use the term citric acid (has its proton) and citrate (lacks its proton, produces alkali when metabolized) to distinguish the two.
In passing, I remind you that citrate is at the center of an ancient energy producing pathway. When we eat it, our cells are prone to use it in that pathway. As they do, the citric acid produces energy but not alkali. The citrate produces alkali and energy.
Below I focus on citrate alkali. Some products also contain alkali as bicarbonate.
Citrate Alkali and Price In the Nine Products
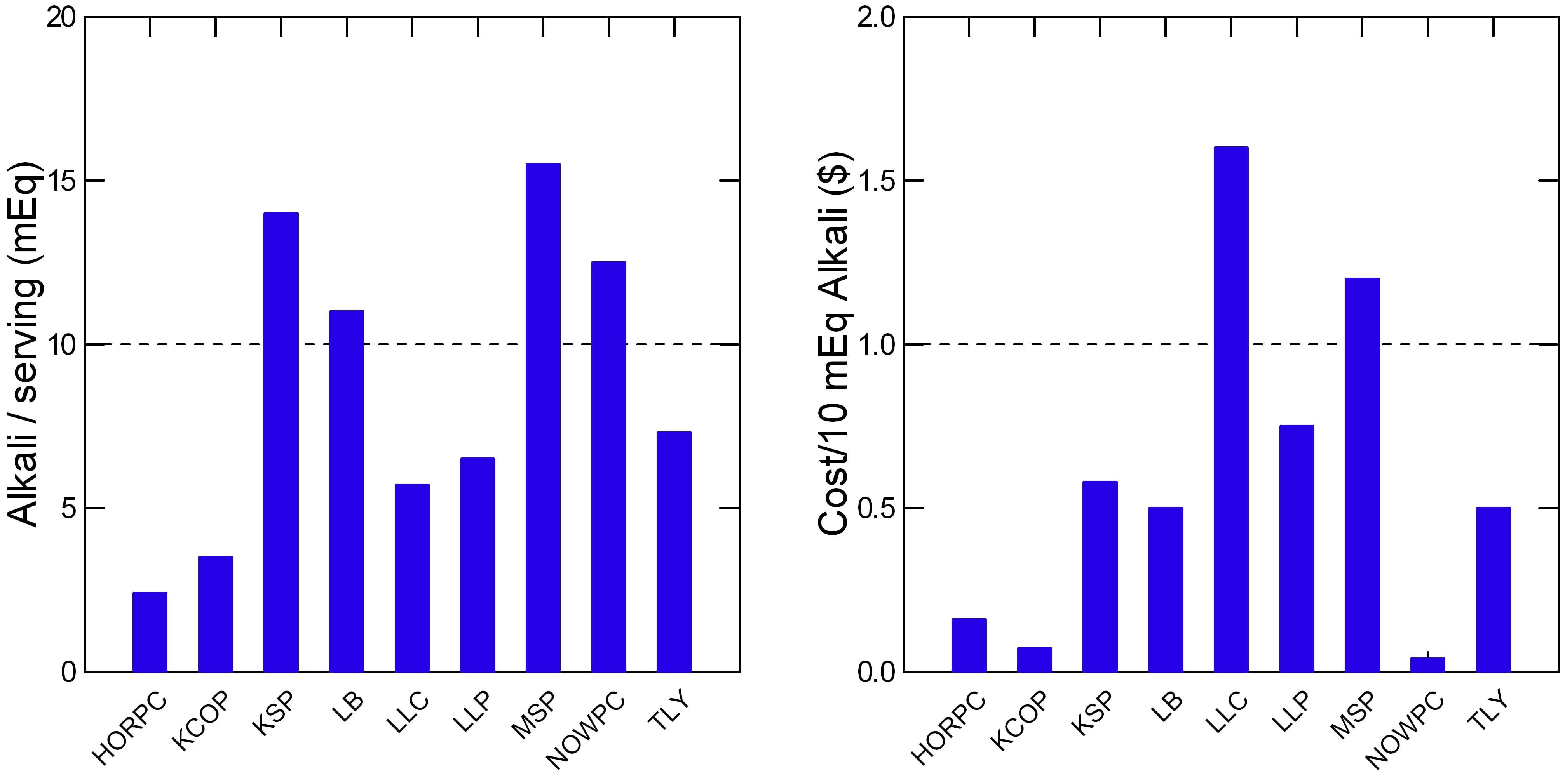 The products differ over an 8 fold range in the amount of citrate alkali per serving (left panel of the figure). KSP, LB, MSP, and NOWPC all have in each serving as much or more alkali as standard medicinal potassium citrate tablets (Dashed horizontal line is at 10 mEq of citrate alkali, the amount in a standard medicinal tablet). This might matter to patients as a convenience.
The products differ over an 8 fold range in the amount of citrate alkali per serving (left panel of the figure). KSP, LB, MSP, and NOWPC all have in each serving as much or more alkali as standard medicinal potassium citrate tablets (Dashed horizontal line is at 10 mEq of citrate alkali, the amount in a standard medicinal tablet). This might matter to patients as a convenience.
The right panel shows the cost in dollars of 10 mEq of citrate alkali from each product – how much each costs to give the citrate alkali in a single potassium citrate tablet. NOWPC is noticeable for a very low price as are HORPC and KCOP. Because the latter two do not have so much alkali in a serving they require one swallow more servings. NOWPC, however has an excellent price and each serving has just over 10 mEq of alkali. MSP and LLC are more expensive.
How to choose is not something I need to discuss. Remember, alkali is alkali, and cost per 10 mEq dose of alkali allows direct price comparisons. So shoppers can make decisions without further medical input. Matters such as flavor, or color, for example, may make a more expensive product desirable – or not. My main point is that nothing about any of the products has any relationship to stone prevention – so far as we know – except alkali, to raise urine citrate.
ADVERTISED VS ACTUAL ALKALI
The main paper I have reviewed here, from Dallas, notes some considerable discrepancies between the advertised and actual amounts of citrate in these products. An excellent review provides considerable additional material as a check against how the Dallas group interpreted product contents. This is important because product content is not so simple to find. I shall refer to the review as ‘this’ article, and ‘Dallas’ for the main one here.
Modest Discrepancies are Common
NOW® Potassium Citrate is listed in this article as containing only potassium citrate – 5 mEq in 1/4 teaspoon of the product. But the Dallas group measured 12.5 mEq of citrate in 1/4 teaspoon and given the high pH about 12 mEq of citrate alkali. Presumably this is a problem with what the vendor provides as information.
Litholyte®, I presume the powder, is listed as containing per packet 6.5 mEq of citrate and 3.5 mEq of sodium bicarbonate. The Dallas group indeed found about 7 mEq of citrate alkali and about 70 mg (3 mEq) of sodium, presumably all bicarbonate. So this product seems consistent between measurement and product information.
TheraLith XR®, presumably per tablet is listed as 2.1 mEq of citrate (1.2 as Mg, 0.9 as K); Direct measurement for 2 tablets was 7 mEq of citrate, and given the high pH about the same citrate alkali. As for NOW® the discrepancy (4.2 vs 7 mEq) is not explained.
Kidney COP®, is listed at 4.5 mEq citric acid + 0.6 mEq Mg citrate or 5.1 of potential citrate alkali. That is indeed what was found – 5.4 mEq but given the low pH only 3.5 mEq is citrate alkali.
KSP tabsTM, 2 mEq of citrate (0.9 Mg, 1 as K) and 2 mEq of sodium bicarbonate giving 4 mEq of alkali in a tablet. Directly measured citrate was 26 mEq of which about 14 mEq was citrate. Measured sodium in one effervescent tablet was 224 mg (9.7 mEq). I suspect this is because of a difference on counting. The measurements in one tab seem about 2 times the advertised content for sodium. For citrate the discrepancy is so large one cannot explain it.
LithoBalanceTM, citrate of 4.4 mEq in one scoop (0.6 as Mg); direct measurement gave 28 and 39 mEq of citric acid providing 9.7 and 13.9 mEq of citrate alkali in a scoop.
Moonstone® Powder. It was not in this article. With more difficulty than I should have encountered I found a label showing/4 capsules: Mg 210 mg (8.75 mmol x 2 = 17.5 mEq); 140 mg (6.1 mEq) sodium; 280 mg K (7.18 mEq); 30 mEq of citrate as these three salts. The Dallas group studied 1 package (26 gm) of the powder and found 60 mEq of alkali advertised. Indeed this much citric acid was found but given the low pH the actual content was only 16 mEq.
These Products are Lightly Regulated
Nothing about the preceding is to impugn the products. They are commercial products more like lima beans or tomato soup than actual medications used against disease. Perhaps they even less regulated than lima beans or tomato soup. That, too, is not a criticism. Government decides how to regulate and views these kinds of supplements as benign enough to regulate lightly. The seeming variability poses no direct risk except that one may not get from the product what is advertised on the label.
The best defense is to test. If your physician requests you take one of these remedies, presumably to raise urine citrate or pH, be sure and retest to see if citrate or pH has risen. The products are not held to the standards of prescribed medication, so be sure it works for you.
WHAT ELSE EACH PRODUCT CONTAINS
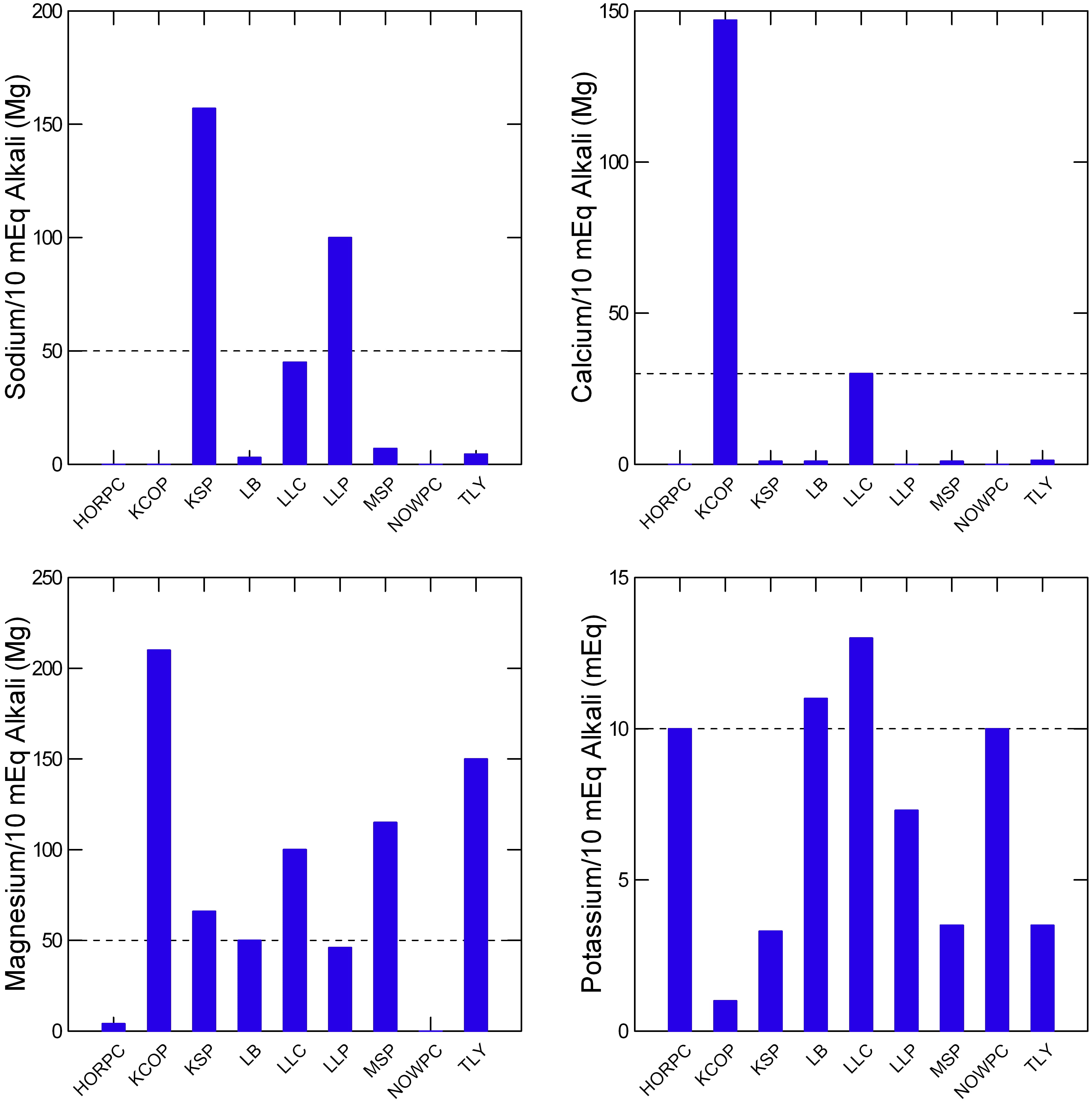 To varying extents each may contain considerable sodium, calcium, or magnesium. The Dallas group conveniently provides measurements standardized to 10 mEq of citrate – how much sodium, calcium, magnesium, or potassium you get from the equivalent of one 10 mEq potassium citrate tablet.
To varying extents each may contain considerable sodium, calcium, or magnesium. The Dallas group conveniently provides measurements standardized to 10 mEq of citrate – how much sodium, calcium, magnesium, or potassium you get from the equivalent of one 10 mEq potassium citrate tablet.
Sodium
KSP and LLP contain 150 and 100 mg of sodium for each 10 mEq of alkali. If one takes a common dose equivalent to four 10 mEq potassium tablets a day, KSP will provide an additional 4 x 150 = about 600 mg of sodium (my figures here are approximate and rounded for simplicity).
That is a lot considering that the US tolerable upper limit for sodium is about 2300 mg, and 1500 mg is considered, by many authorities, as ideal. LLP will provide about 400 mg for the same daily dose of 40 mEq citrate (equivalent to four 10 mEq potassium citrate pills).
Calcium
KCOP contains almost 150 mg of calcium in a dose that delivers 10 mEq of citrate. So if you use it at the common dose of 40 mEq alkali a day (four 10 mEq potassium citrate tablets) you get just about 600 mg of calcium. The ideal daily intake of calcium is about 1000 to 1200 mg, meaning this remedy provides nearly 1/2 of a very liberal daily intake.
Is that a problem? In way it might be. We need real foods, including dairy products, whereas this remedy is essentially a hefty calcium supplement. Given that calcium is most important for bone, and the main study I know of concerning calcium intake and bone mineral balance used supplements with meals, I would think KCOP should be used with meals. Typically people take potassium citrate 2 10 mEq tabs twice a day. Because they contain just that – potassium citrate, timing to meals is not necessary. If four KCOP doses are taken and food calcium is at US ideal levels, calcium intake can be very high (1200 + 600 = 1800 mg/d). That might be too high for some people. Those with even mild kidney impairment, for example, a not uncommon result of stone disease.
Magnesium
KCOP, TLY, MSP and LLC all have abundant magnesium. For KCOP, a conventional 40 mEq dose of citrate alkali (four potassium citrate tablets a day) will give over 800 mg of magnesium. Most magnesium is in cells, and I know of no special hazard from an additional 800 mg/d from pills. Present US daily intake recommendations for magnesium are around 400 mg, so the 800 mg added to food does raise one’s eyebrows. Corresponding values for TLY (600 mg/d), and MSP (500 mg) also seem high.
Potassium
At their highest, none of these products provides appreciably more potassium than 40 mEq of standard potassium citrate would provide (40 mEq). Many have little potassium, so if one needs to replete potassium in a kidney stone patient they will not do. Stone patients not rarely are given thiazide diuretics, which cause potassium loss, and require significant replacement. This is often in the form of potassium citrate. Another common reason is diarrhea, a cause of stones in GI disease.
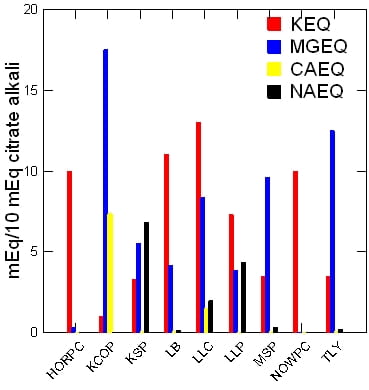
All Four At Once to Make it Easy to See
 With a little magic and a little counting up, I got all the four together in one place. Each bar shows how much potassium, magnesium, calcium, and sodium are in each product. All are in mEq, meaning their actual comparable units of charge to balance citrate or bicarbonate. In general sodium will be with bicarbonate. The other three are usually with citrate. All are presented in amount/10 mEq of citrate alkali.
With a little magic and a little counting up, I got all the four together in one place. Each bar shows how much potassium, magnesium, calcium, and sodium are in each product. All are in mEq, meaning their actual comparable units of charge to balance citrate or bicarbonate. In general sodium will be with bicarbonate. The other three are usually with citrate. All are presented in amount/10 mEq of citrate alkali.
A few (HORPC, HOWPC) are almost all potassium citrate. KSP and LLP have notable sodium presumably as bicarbonate. KCOP is remarkable for its high calcium, and KCOP, LLC, MSP, and TLY for their magnesium. None of this is by way of criticism, merely to illustrate the variety of formulations. Magnesium may cause GI symptoms, and so may potassium.
WORK BY OTHER SCIENTISTS
Several groups have reported studies using these OTC alkali, and I would be an ecumenical reporter.
A crossover study – each subject gets each product – tested citrate response in 10 people to “LithoLyte (20 mEq 2 times per day) or KSPtabs (1 tablet 2 times per day).” The last would provide about 30 mEq of alkali – take a look at my first figure, left panel. For Litholyte, given about 7 mEq of alkali per serving this would have required about 3 – 4 servings twice a day. Litholyte did not raise urine citrate significantly, but KSPtabs did (758 vs 597, and 797 vs 597). Note these were 10 normal people, and patients with low urine citrate would show more dramatic results.
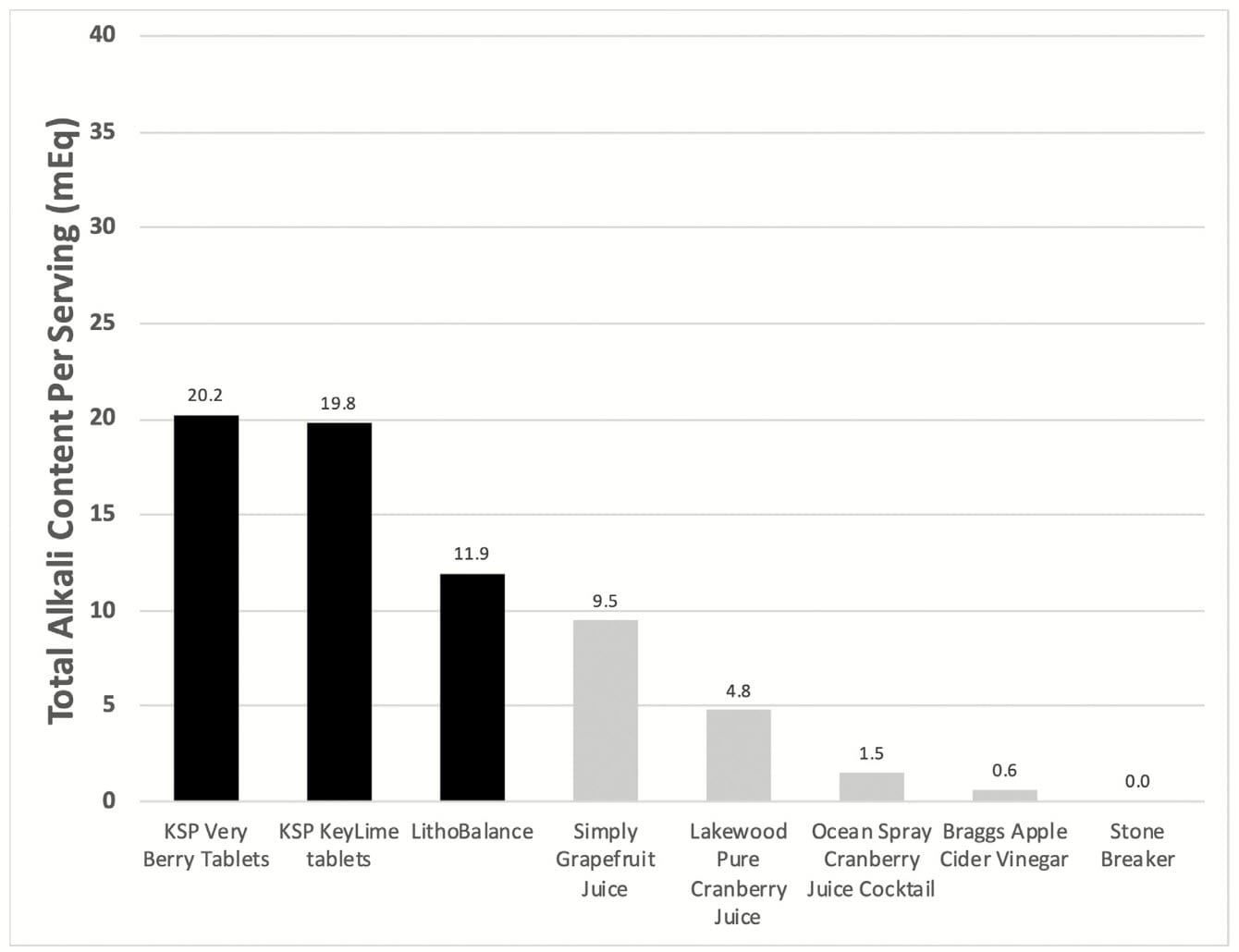 A structured interview study included useful analytical data on the total alkali available in a range of products which only slightly overlap those studied in Dallas.
A structured interview study included useful analytical data on the total alkali available in a range of products which only slightly overlap those studied in Dallas.
Of interest, the total alkali in the KSP products and in LithoBalance are near to those of similar products from the same distributor. Stone Breaker stands out as having no alkali but presumably some other power to eradicate stones.
About the interviews, what brought people to an item, who used them, why, that is all outside what I have to say here. As well, outside my expertise, as I know nothing about opinion research.
WHO SHOULD USE THESE REMEDIES?
Patients Who May Benefit From Alkali Supplements
“These remedies” refers to all the products here, though my main interest is in those studied in Dallas. All are, if anything, alkali, and of use when alkali are of use. When alkali are not of use, they are not of use. Nothing about them has anything to do with kidney stone prevention – that is established by any science at all – apart from increase of urine citrate or pH via the imposition of an alkali load on the blood buffers.
Who Benefit From Alkali Supplements?
Stone Formers with Low Urine Citrate
Certainly not all stone formers. We do not prescribe potassium citrate just because someone has formed calcium stones. For example more is not sensible in calcium stone formers who have very high urine citrate. Some stone formers have very high urine pH and form calcium phosphate stones. Extra alkali in such people has has never been tested for stone prevention, and to me at least has some risk of worsening things.
The best data relating risk of new stone onset to urine citrate came from the Curhan group at Harvard. They found risk increased as urine citrate fell below 400 mg/d. Therefore I accept that number as a not unreasonable basis for one of these remedies, or for potassium citrate tablets themselves.
Those with Other Specific Conditions
Alkali supplements have their place to prevent uric acid stones. Extra alkali may benefit bone disease. Alkali supplements are needed for some GI diseases with diarrhea and alkali loss. Ileostomy is a clear example, but often requires sodium alkali. Some experts recommend alkali supplements for chronic kidney disease. Alkali raise urine pH and that can help reduce cystine supersaturation in cystinuria. Alkali are always used to treat the metabolic acidosis of distal renal tubular acidosis. But these are medical conditions with real medical decisions that need making, and need for real medical supervision. It is the physician who chooses alkali, the proper dose, and perhaps one of these supplements.
The Special Case of Uric Acid Stones
Curiously, ads for these products are not aimed at uric acid stone formers. Alkali can prevent such stones to absolute, and even dissolve them, from time to time. This because it is low urine pH that causes them, and alkali can raise urine pH. Of course, routine potassium citrate tablets will do the same.
Uric acid stone formers would be ill advised to use these remedies on their own. Label citrate content does not gauge citrate alkali. Repeated testing is required to be sure urine pH rises and remains high – these products are not regulated like drugs and composition is not guaranteed in the same manner. Patients need their physicians to adjust dosage in accord with actual alkali content as presented in the Dallas report and to monitor 24 hour urine pH. With such supervision, any of the products should work well.
PEOPLE IN GENERAL WILL NOT BENEFIT
To say that one should buy and take any of these products just because one has formed a kidney stone – that is as unacceptable as it is to prescribe potassium citrate itself for the same ‘just because’ reasons. Alkali are not a general nostrum, not some invariable benefit to kidneys, or to the body.
For the common person without evident disease, alkali supplements are not in any way known to improve health – kidney health, bone health, or any other kind. I might say, though it is not the topic here, that the vast richness, beauty, and appeal of fruits and veggies includes such an abundance of alkali, mainly as potassium, that they alone can provide 60 to 100 mEq daily along with pleasure, too. I wonder, sometimes, why people might want to choose supplements for that which fills their grocery stores and graces the tables of those who gather it into their kitchens and prepare it into divine sustenance.
What I mean by all this high talk is that fruits and veggies provide such ample alkali healthy people never need pill supplements. The US diet guidelines call for ample fruits and veggies for everyone, every day. Let’s do that and leave pills for those with diseases that somehow force them upon us.
I WILL NOT RECOMMEND THE ‘IDEAL’ CHOICE
Because these are commercial products, like tomato soup, or green beans, that compete on price and other qualities for consumer dollars, and because this site abjures connection to commerce I leave purchesers to their own judgement.
But I, for stone formers, have about the entire product group a potent and general prejudice.
It is your physician who should point you to a product, if that is medically proper. If it is clear from your physician that alkali are suitable as a treatment, and your physician has recommended some amount of alkali, one can safely use these products and benefit from them provided dosing is adjusted for how much alkali each contains in a serving, and provided the extra sodium, calcium, and magnesium are not a concern for the physician who is responsible for your care. Though they may reside on OTC shelving, these products should be used with the guidance of physicians. For it is upon them that society, law, and custom have placed the robe, the seal, and the yoke of authority.
Dr. Coe, You are recognized as an expert in your field and certainly as relates to Kidney Stones. I have a simple question. As a nurse for over 35 years and 30 plus years in I.C.U., many friends, associates and acquaintances come to me when they have medical challenges. I would like to know your thoughts on utilizing the dietary supplement Kidney C.O.P. to help stop stone recurrence for those patients with a known susceptibility to getting calcium oxalate stones. From what I read, the five active ingredients Citric acid, Magnesium citrate, Vitamin B6, Phytin (Ip6) and banana stem (Musa) are all ingredients that make sense as I have found several clinical studies with positive results utilizing these ingredients. Kidney C.O.P. looks like a possible safe cost-effective solution, but I am not a medical doctor and I am certainly not an expert in the field, so I am reaching out to you. In advance, your input and/or thoughts are greatly appreciated.
Hi Cindy, COP and its similars – moonstone etc – are potassium citrate replacements: Lower prices and supposedly better tolerance. The B6, phytin, and banana lack real data supporting stone prevention – trials are very poor for them. But COP is not at all unreasonable if the stones are thought to benefit from alkali, which essentially all act by increasing urine citrate or – in the special case of uric acid – urine pH. Of course the article is a stub – I have not had the time to expand it. Regards, Fred Coe
Hi Dr. Coe,
I just had a follow-up ultrasound that showed I have two new kidney stones in my left kidney. This comes after surgery for a blockage where the ureter meets the kidney in Nov 2020. One large kidney stone was removed in a basket at that time. Some smaller ones were detected in October but must have passed without notice.
I see my urologist on Tuesday. The only advice I got at my last visit was a list of high oxalate foods and told to drink more water with lemon in it. I’ve also used the Moonstone powders in water. I also have cysts in both kidneys.
I just found your website and that of your colleague, who promotes a kidney stone prevention diet.
My doctor did not order a 24 urine collection or a referral to a nephrologist or a dietitian.
My urologist is the chief urologist for the Univ of Arizona Medical School and Banner Hospital. I should add that we moved to Tucson in August 2019.
I won’t have a lot of time with this doctor. What are the most important questions I should ask about going forward?
Thanks,
Ramona Hensrude
Hi Ramona, Of course one is concerned if the stone is due to continued obstruction at the uretero-pelvic junction. He will absolutely know that being a surgeon. If it is not from obstruction, the stone is coming from urine abnormalities and I imagine he will want to order 24 hour urine testing with proper serums, or send you to someone who does prevention work as his colleague. To attempt stone prevention with proper studies is futile. Moonstone, lemons, all that is walking in the dark. There is no reason at this advanced time in history to attempt prevention without diagnosis of cause. Regards, Fred Coe
Hi Dr. Coe,
I have had multiple large Kidney stones 10+ in size I’ve had 2 lithotripsy’s and 1 PCNL. I have had a 24 hour culture and the urologist found no trace of citric acid in my urine. I have been told to eat a low oxalate diet drink plenty of water and exercise. None of this helps and my left kidney continues to makes stones at a remarkably alarming rate. I stumbled across the kidney cops tablet but I can’t take it (I don’t think because I’m allergic to bananas) is there anything you can suggest?
Thank you in advance for any help you can offer.
Connie Hearn
Hi Connie, I am embarrassed that you commented on what is a draft of a proper article – I should hide it until I get a chance to do more. That you have no citrate is very important and requires an explanation for what appears to be active stone forming and an unusual urine finding. Can you tell me if your stones are calcium phosphate? Is your urine alkaline? I can try to help but need more information. In the meantime, these alternatives are merely forms of potassium / sodium citrate of which any would do, but I would not use them until you know more about what is really wrong. If you like, you can post more details. Regards, Fred Coe
Thank you so much for the very interesting article. It was so good to read what you thought and found out. We are so lucky you keep us informed.
I have been trying for several weeks to make an appointment with Dr Coe. I have been following his website for many years. Ive read all the articles. I am a stone maker since
college days and have had 11 litholinks, a lithotrpsy and 2 ureteroscopy’s. The Doctors tell me that it is in my dna like my dad and that nothing can be done preventitive.
My primary doc and myself decided it was prudent to get an appointment with Dr.coe
Can you please help. Sincerrely, John Carlucci 4849196153
and
Hi John, Sorry you had to write about delays. I believe this has been taken care of. Best, Fred
Hi Dr. Coe,
I am a nephrologist, and during training it probably won’t surprise you to hear that our kidney stone teaching was wanting. So, I’ve essentially learned all my kidney stone physiology and management from your website, and your papers on Randall’s plaques. A very basic and important thing you state in the article above surprises me. My understanding was that citrate, in addition to serving as alkali to help reduce uric acid stone formation, can chelate calcium within the urinary lumen and help reduce calcium stones (if urine citrate levels are quite low). There is often a reason, as you’ve pointed out, for the low levels- either a partial RTA, or a dietary aversion to anything green and leafy, but my confusion remains. Your article above says that the only role for citrate is to provide alkali buffer. Is there not also a role for citrate in calcium chelation within urine?
Hi Dr Johnstone, I have emended the article to emphasize the effect of oral alkali to raise urine citrate. Thank you, Fred
I have polycystic kidney disease with relatively preserved renal function for my age (GFR of 64 at age 74). About 15 years ago I developed recurrent uric acid stones which I presume is somehow related to my ADPKD. I have been on potassium citrate 15 meq bid and have not formed a stone since. Recently, after major surgery I developed a stress ulcer and felt it best that I stop the potassium citrate, because, as you know, it is hard on the stomach. (I had no prior GI problems with the med previously.) My urine pH untreated is usually 5.5. I thought I would go on one of the supplements in your article as a replacement since it would be easier on my gut. Any recommendations as to which would be best in my case? In your experience, are patients able to go back on potassium citrate tabs after an ulcer has healed?
Hi Jason, Given you have an underlying kidney disease, and given that you need alkali to prevent more uric acid stones, Moonstone might be best. It has alkali and does not have excesses of calcium, sodium, magnesium, or potassium. Of course your physicians need to be in charge here, as my ‘advice’ is merely technical, and I do not know your actual renal function or pattern of serum electrolytes. If the ulcer heals K citrate should again be feasible. Regards, Fred Coe
Dr. Coe –
I’m slightly confused about your calculation of the mEq of citrate alkali being contributed by the magnesium citrate in Moonstone, which you give as 17.5 mEq. You note that there is 200 mg of elemental magnesium in 4 capsules. Given that mag citrate is 16% elemental magnesium by weight, that would mean that those capsules contain a total of 1250 mg of magnesium citrate salt (200/.16).
Keep in mind also that – technically – the form of mag citrate used in all OTC supplements is trimagnesium citrate. Dividing the weight of the salt by the molecular weight of trimag citrate (451), then multiplying by the valence (2) – you get a total mEq of 5.5 – not 17.5. (1250/451 X 2 = 5.5)
What accounts for this difference?
Hi Mark, I believe you are referring to this part of the article:”Moonstone® Powder. It was not in this article. With more difficulty than I should have encountered I found a label showing/4 capsules: Mg 210 mg (8.75 mmol x 2 = 17.5 mEq); 140 mg (6.1 mEq) sodium; 280 mg K (7.18 mEq); 30 mEq of citrate as these three salts. The Dallas group studied 1 package (26 gm) of the powder and found 60 mEq of alkali advertised. Indeed this much citric acid was found but given the low pH the actual content was only 16 mEq.”.
So I am reporting the label citrate content. The Dallas group found 15 mEq of citrate alkali per single dose (one pill) or 60 /4 pills, the amount in the powder for which I had a label to go on. They report about 10 mEq of magnesium peer 10 mEq of citrate alkali. In other words although I am sure the trimagnesium citrate salt was used there are other magnesium salts in the product. The actual available alkali is totally dependent on the pH of the final solution and the variation of pH cannot be just from dissolving the mg citrate salt, but from other processes. That is why the Dallas group measured citrate alkali directly. Put another way we do not know the exact composition of any of these products. I think I have it right, and so do you. If uncertainty remains lets ask the Dallas group to help us. I did already. Regards, Fred
While the research shows that these products can help prevent kidney stones, I am concerned
about the additives, specifically, the artificial sugars. I know they are added to make the products
palatable but isn’t there research that shows that artificial sweeteners are not healthy? I would
not be so concerned if these products were to be taken once in a while or for a short period of
time but I imagine I will need to take something indefinitely to prevent future stones. Thank You
Hi Ellen, You make a very sensible point and I can add to it. Indeed none of these products have any proof of efficacy against new stones. Potassium citrate itself has two trials showing efficacy, but these contain addition materials – some a lot of sodium, some a lot of magnesium, etc, and may not perform the way potassium citrate did in its trials. That is why they cannot make the claim to prevent stones – or should not. As for what is in them, I did what I could with the wonderful work from the Dallas group and there things stand. Best, Fred
I have a simple question about Moonstone that my doctor prescribed on top of calcium citrate. If a diabetic with an AlC of 7.4, will the “Maltodextrin” increase my sugar and AlC? Thanks
Hi Sally, It should not. Fred
Thank you. When I took the Moonstone, it felt like my face and lips were going numb. That’s why my first question.
Sally that might be an allergy. did you figure it out?
From the article: “NOW® Potassium Citrate is listed in this article as containing only potassium citrate – 5 mEq in 1/4 teaspoon of the product. But the Dallas group measured 12.5 mEq of citrate in 1/4 teaspoon and given the high pH about 12 mEq of citrate alkali.”
The NOW product label states that 1/4 teaspoon provides potassium (elemental) 448 mg (from 1,400 mg potassium citrate) whereas a potassium citrate prescription that I use provides 1080 mg (10 mEq). NOW’s 1,400 mg versus pharmaceutical’s 1080 mg seems to indicate an mEq of 12.96. The NOW product does not list any mEq value on its label, however this derived 12.96 mEq is a closer match to the Dallas figure of 12.5.
Perhaps I am applying faulty thinking here.
Hi Barry, The label was confusing to me as well. The product contains about 12.5 mEq of alkali and that is just about right (1400/1080 mg k citrate crystals) or 12.9 vs 10 meq. I am sure the company provides the information required by low of OTC products and it is just not enough. I believe the Dallas measurements. The NOW product has no sodium, calcium or magnesium, so I presume most of the charge balance is indeed from potassium. It is like food grade potassium citrate one can buy in bulk. Regards, Fred
Dr. Coe,
Kidney C.O.P. lists at its website 5 patents for its product. I used Google Patent to find the first patent application for its Patent 9233135. I found extensive disclosures about the ingredients and references to supporting academic literature. As someone who buys and uses this product, I would like to know if the disclosures of the 5 patents changes your analysis.
Hi Paul, You really far surpass my work as I do not know how to evaluate patents. I did indeed read the patient you quote. The citrate has trial data to support stone prevention. Magnesium has no trials but is a common remedy of uncertain value. Pyridoxine and phytin as well. Musa is not known to me. My article focused on the potassium alkali of the products, and derive from excellent work at Dallas that I merely review. The included reference on my site shows the citrate treatment effects. All I have asked from COP was its citrate. I doubt the other included materials cause harm. Musa is a derivative from plantain species and an ancient stone remedy of unproven significance. I quote the most colorful if not the most recent reference. Regards, Fred Coe
plantain like the lawn weed, or plantain the fruit that looks like a banana?
The fruit. Fred
Dr Coe. Is Kidney COP safe to take to attempt to determine its efficacy works for my personal situation?
Hi Frank, Given I do not know what you want the material to do for you, I cannot do much by way of answer. In general – but granted here I have no specific knowledge about your medical situation – when used as directed the material should not be dangerous, but there are exceptions – kidney disease, as an example. So I cannot really say lacking enough information to say anything. Regards, Fred Coe
I have kidney stone formation from time to time. Recently I was taken to the emergency room because my blood test was bad and there were several stones. They were all taken out. Then they found that one of my kidneys is month functioning.
Hi Frank, This is a very concerning story. Perhaps a stone obstructed one kidney and damaged it, but the other one should maintain normal kidney function. I presume your physicians are attending to this matter. It needs close attention. Regards, Fred Coe
Dr, Coe,
I had 4 mm stone (unspecified) last year which resolved itself after a month. The doctor prescribed Noculi syrup which has 1 mEq magnesium per ml, 2 mEq potassium per ml and 3mEq citrate per ml.
24 hour urine test was not done (typically not done here in India), My urine pH was 5.4
I have been taking 15 ml twice. My present urine pH is 6.5.
It comes to 90 mEq citrate per day and 60 mEq potassium.
My serum potassium has climbed to 5.94 mmol/L from 5.0 mmol/L at the time of stone.
I am trying to see if 24 hour urine test is possible here but do you think the quantities I am taking of potassium citrate are reasonable. And is the high serum potassium needs to be lowered?
My diet is dairy-rich. Approx 500-600 ml of milk plus other yogurt sometimes. and 200 ml of buttermilk. Do I need to look at calcium intake?
Hi Vishal, So you are taking 15 ml of a solution with 2 mEq/ml of potassium, meaning 30 mEq per dose and your serum potassium rose from a baseline of 5 to 5.94 mEq/l. Baseline is high, and you do not report your serum creatinine. Also you do not say if the blood was drawn after a dose – I suspect it was. The dose of potassium is itself within the common adult range but perhaps you have less than normal potassium response – diabetes, reduced kidney function, some other drug. I cannot tell from here, but your physicians will know. The diet itself should not cause potassium problems and the material you are taking should raise urine pH. So, this is an issue your physicians must look into, and resolve. Regards, Fred Coe
Thanks for the reply. There is a question regarding the use of calcium ingestion to bind with oxalate in the intestine. What is the form of oxalate that we have in the food? Is it not bound with some ion like calcium in the first place?
Or it is free oxalate in food like spinach and it is only bound in the intestine as you say?
I could not find any information as to the form of oxalate in the food. Is it free oxalate or bound with something?
I do think it would be helpful to make it clearer.
Hi Vishal, food oxalate will form electrostatic bonds with whatever cations are around, including calcium. The latter is tight enough to prevent oxalate absorption. The molar equivalents of calcium far outweigh food oxalate so calcium absorption proceeds as it will, oxalate is reduced. Food oxalate bound with calcium is oxalate bound with calcium, as noted. Fred
So, the food oxalate may be bound with calcium but then why do we need extra dietary calcium to bind oxalate?
Does the bound food oxalate eg calcium oxalate becomes unbound in stomach or intestines?
Hi Vishal, indeed, it does ‘unbind’ from food materials because stomach pH runs about 1-2. The colon is a main site of absorption, along with ileum. Regards, Fred Coe
Many years ago, I started eating Tums for a month or two because I thought it was a good idea for bone health and promptly got what I think was a kidney stone. It hurt a lot. It’s in the top 3 pain experiences of my life. I spent the night on the cold tiles of the bathroom floor waiting to pee again, peeing again, until finally I was done. Then I looked up what happened and decided to stop it with the Tums and it never happened again. Is there a type of kidney stone that’s likely to have been? I’m curious. Thanks!
Hi ‘but one…, Tums are calcium carbonate and calcium phosphate stones have been reported as a consequence – not trial data but observations. Regards, Fred Coe
Can excessive calcium intake as food lead to calcium phosphate stones?
As we try to avoid oxalate stones by consuming calcium-rich foods like dairy and
simultaneously try to raise urine pH by taking citrate supplement, can it be unsafe at some point to lead to phosphate stone?
Hi Vishnal, GI calcium absorption is regulated so the fraction absorbed falls as diet calcium increases. Net bone uptake rises as absorbed calcium overtops urine losses, or falls with the converse. One does not raise diet calcium in a stone former randomly. The proper diet is low diet sodium, so urine calcium cannot increase markedly, then increased diet calcium to bind oxalate and preserve bone. Regards, Fred Coe
Hi Vishnal, GI calcium absorption is regulated so the fraction absorbed falls as diet calcium increases. Net bone uptake rises as absorbed calcium overtops urine losses, or falls with the converse. One does not raise diet calcium in a stone former randomly. The proper diet is low diet sodium, so urine calcium cannot increase markedly, then increased diet calcium to bind oxalate and preserve bone. Regards, Fred Coe
Any information on litholyte and its affects on colitis would be appreciated
Hi Denice, I am afraid I do not have such information. Regards, Fred
Hi Dr Coe, I have Short Bowel Syndrome with less than 2 feet of small bowel left so with chronic diarrhea my citrate levels were 0. I have had to take Potassium Citrate and citric acid solution for 3-4 years 30-40cc 3-4 times a day. Now I have started having difficulty getting it filled for some reason. Also, it is very expensive even with Good Rx at $106 a month. I was looking at the OTC Alkali citrate. I was thinking about trying Moonstone combo of powder x1 daily and tablets x2 daily. My last 24-hour UA showed Citrate at 228 on 40cc 3x a day. The rest of my labs are great without TPN. I know I will probably need a liquid potassium with it but hope the combination of both will work. Do you have any suggestions?
Hi Laura, Short bowel patients lose a lot of sodium alkali, so you could replete with sodium bicarbonate – very inexpensive – and potassium chloride for the potassium losses – also very inexpensive. Perhaps your physicians might want to consider that alternative. Regards, Fred Coe
Hi Laura, Short bowel patients lose a lot of sodium alkali, so you could replete with sodium bicarbonate – very inexpensive – and potassium chloride for the potassium losses – also very inexpensive. Perhaps your physicians might want to consider that alternative. Regards, Fred Coe
Hi Laura, Short bowel patients lose a lot of sodium alkali, so you could replete with sodium bicarbonate – very inexpensive – and potassium chloride for the potassium losses – also very inexpensive. Perhaps your physicians might want to consider that alternative. Regards, Fred Coe
Good afternoon DR. Coe.
I need your help. I already had surgery twice to remove a bladder stone made of 100% uric acid. One in January 2022 and then it formed again and I had to have another surgery in December 2023. Both times the stone was 3cm so it was bothering me and I was having blood in urine. After the first removal the stone formed again after a few months cause my urine ph was 5.3/5.5 and I was not taking potassium citrate. I tried potassium citrate for a few but it didn’t t dissolve it.Maybe it dissolves them in the kidney and not in the bladder? Now after the second operation I m taking 40 meq a day of potassium citrate. ( 15 after lunch and 25 after dinner and after 5 months I did an ultrasound yesterday and no stones.
The problem is that my blood potassium is now 5.3 and all the previous exams was 4.7/4.9 and the cardiologist told me it can t go higher than this because is going to be dangerous. I m very worried because if I stop taking the potassium citrate I ll get the stone again but if I keep taking I fear the potassium is going more high.
Can you suggest me what to do or if I can substitute the potassium citrate with something else or at least lower and take something else maybe only during the day. Thank you for your time
Hi Giovanni, Sodium bicarbonate will work as well, in the same doses (in milliequivalents) and post no potassium risk. Being the bicarbonate, not the chloride salt of sodium it will not raise blood pressure or cause fluid accumulation. Regards, Fred Coe
Hi. Thank you very much for your prompt answer. Can I find it over the counter? Which dose should I take?
Any side effects? Thank you
Hi Giovanni, sodium bicarbonate tablets are sold OTC in the US at about 6 mEq/tablet. So 2 three times a day will raise urine pH effectively. Regards, Fred Coe
Hi Dr Coe,
I have dementia and struggle to understand this article. I also have a urologist whose suggestion to avoid the development of further kidney stones after I passed a 5 mm calcium oxalate kidney stone of just hours before a scheduled ureteroscopy and am left with a 10 mm stone still sitting in my left kidney is to lower dietary oxalate.
I assume these stones were developed due to a diet heavy on white and sweet potatoes, cashews, dark chocolate, strawberries, and blueberries. My diet has been totally predicated on a need to avoid gluten, dairy, and foods high in salicylates due to Hashimoto’s and Hereditary Hemorrhagic Telangiectasia.
I’m homebound and mostly bedridden from other health issues and need to avoid clinic and ER visits as much as possible. I will try to find another urologist who will provide greater help. In the meantime, other than increasing my water intake and trying to find anything to eat that meets the requirements of all of my health conditions, do any of these products in this article make sense for me? I’m too ill otherwise to also be ill with kidney stones and infections. What should a person do who cannot tolerate dairy? I considered a calcium supplement but read in a Harvard article that such supplements may actually increase stone formation.
Any help would be so appreciated.
Hi Tanya, Your physicians should offer to evaluate you for causes of stones and focus on what is found. Here is the right place to read about that. I would not try to prevent stones without the 24 hour urine and blood tests listed in the article. The urines can be collected at home and samples mailed back to the company. Best, Fred Coe
Dr. Coe
I have had around 8 stone removal procedures, both sides, and it is not getting better. These are calcium oxalate stones. I have had trouble with the Pot citrate 1080 tablets that the urologist gave me. They are very hard for me to swallow. I have purchased all the Moonstone and Kidney COP products. I am comparing ingredients and appreciate your postings. All of this happened after I had a bowel resection in the lower area of the small bowel due to an over abundance of adhesions of scar tissue from appendix removal 45 years ago. They removed by Ileocecal valve and the ileum which has caused me to have malabsorption of bile acids. Without Welchol medication I have chronic diarrhea every day. That is when this stone forming took off. What would be your recommendation of medication including OVC drugs and the prescription Pot Citrate1080mg x 3 daily.
Hi JP, given your surgery high urine oxalate is very likely a major factor in stones. You do not show 24 hour urine data so there is not much more I can add. Best, Fred Coe
Dr. Coe
I forgot to add I am 66 in great health and vital otherwise. I do not take any other drugs at all except B12 due to malabsorption issue.
JP’s Supersaturation Profile 24hr urine:
Calcium Oxalate Crystal value 2.00
Brushite Crystal value -2.01
Hydroxyapatite Crystal value 0.30
Uric Acid Crystal value 3.67 (high)
Collection Duration value 24hr
Volume value 1100ml
Sodium, U 105 mmol/24h
Potassium, U 42 mmol/24h
Calcium, U value 220 mg/24h
Magnesium,U value 66mg/24h
Chloride,U 119mmol/24h
Phosphorus,U 451 mg/24h
Sulfate Urine 14 mmol/24h
Citrate Excretion value 199 mg/24h
Oxalate, U .14 mmol/24h
Oxalate, 12.3 mg/24h
PH Urine 5.0
Uric Acid, U 297 mg/24h
Creatinine 1452 mg/24hr
Osmolality, Urine 684 mOsm/kg
Ammonium, 24 hr, U 30 mmol/24h
Urea Nitrogen, U 8.4 g/24h
Protein Catabolic Rate, U 78 g/24h
Patient Surface Area 1.73m(2)
Height/Weight Adult values are not corrected for body surface area
Hi JP, Your urine is very acid, with high risk for uric acid stones.The reason is not known to me, but I see an ammonia excretion of 30 mmol/d with an acid load from sulfate of only 14 mmol/d and a protein intake of only 0.78 gm/d, which suggests a GI problem with alkali loss. I see a low citrate of 199 mg/d which is consistent. I know nothing more. Best, Fred Coe
Hello Dr. Coe. Thank you for providing this great information.
I’m 54 yo with a 40 year history of stones. In the last few years the number of stones has increased significantly (I pass about 4 stones/year).
My history includes hypertension, celiac disease, fatty liver, DM,
I do a good job of keeping hydrated although I have frequent diarrhea (despite following a strict gluten free diet).
My labs are as follows:
Na 140
K+ 4.0
Cl 105
CO2 27
Anion Gap 8.0
Glucose 110
BUN 8
Creatinine 0.77
BUN/Cr Ratio 10
Protein 7.3
Albumin 4.4
A/G ratio 1.5
Calcium 9.4
T Bill 0.9
AST 34
ALT 50
Alk Phos 50
TSH 2.294
Urine microalbin 2.294
Ur creatinine 114
PTH 67
Ur PH 7.0
Ur leukocytes, nitrite, protein, glucose, ketones, bilirubin are all negative
Uric Acid 6.6
24 hr urine:
Calcium oxalate 2.14
Brushite Crystal 1.32
Hydroxyapatite 7.22
Uric acid crystal -4.77
Volume 2300ml
The only medication I’ve been prescribed by my urologist is Indapamide 1.25mg daily.
I’m curious if any of the aforementioned OTC medications would help.
Thank you very much for your time.
Hi Tom, The labs you post are mainly normal and the urine data too scant to make any sense of. What are the stones made of? What are the 24 hour urine value for key measurements like calcium oxalate citrate etc? If you send more I can try to be helpful. Best, Fred Coe
Hi Dr. Coe,
Here is some additional information regarding my lab tests.
Thanks again for your help.
Tom
CALCIUM OXALATE CRYSTAL,
Normal value: Reference Mean= 1.89 DG
Value
2.14High
BRUSHITE CRYSTAL,
Normal value: Reference Mean= 0.46 DG
Value
1.32
HYDROXYAPATITE CRYSTAL,
Normal value: Reference Mean= 4.19 DG
Value
7.22High
URIC ACID CRYSTAL,
Normal value: Reference Mean= 1.18 DG
Value
-4.77
My stone analysis is 60% Calcium oxalate dihydrate. 40% Calcium phosphate
Hi Tom, These composite scores tell us that your urine is overly saturated with respect to the two crystals in your stones. But it is the constituent analytes that we manipulate to alter these saturation. This report seems like Mayo Clinic and they give all of them. Best, Fred Coe
Hello,
My urine PH is high, my urine calcium is high, and my urine citrate is low. I have tried to take the K citrate many times, but it really upsets my GI tract. I have then been prescribed ORACIT and I react to the artificial sweeteners used. I am trying to find something I can tolerate. My nephrologist insists none of his other patients have trouble with these. I was going to try Litholyte, but after reading this, I am not sure if it is worth it or not. I also take Chlorthalidone.
Hi Julie, Moonstone is often tolerated well. Fred Coe