The first article in this series of three summarizes the importance of filtration, the rudiments of how we measure it, and the results of research concerning how kidney stones reduce it. This article gives the details of kidney function in stone formers. It carries the key references, and supports the summary assertions of the much shorter precis. But because it does not duplicate the brief introduction to filtration per se, I advise reading the shorter first article as an introduction.
The third article tells how filtration works, and the details of its measurement in patients including the eGFR estimating equations. It illustrates how filtration affects key stone risk factors and offers a brief tour through the kidney for those who want to know where things are in it. Unlike the first and second, it is very long and complex, so perhaps only few will choose to read it.
Filtration Rates in Kidney Stone Formers
As the first article in the series mentions, physicians estimate kidney function from serum creatinine, eGFR – an index derived from serum creatinine, age, sex and race, and from clearance of creatinine CCr. This latter requires timed urine collections and we commonly calculate if from the 24 hour kidney stone evaluation urine samples when we have a corresponding paired serum creatinine measurement.
Our Population Averages
 Over 45 years of practice, we have always evaluated our own stone forming patients with three 24 hour urine samples paired with three corresponding blood samples. From this trove we published mean CCr values asking of patient values lay below those from normal controls.
Over 45 years of practice, we have always evaluated our own stone forming patients with three 24 hour urine samples paired with three corresponding blood samples. From this trove we published mean CCr values asking of patient values lay below those from normal controls.
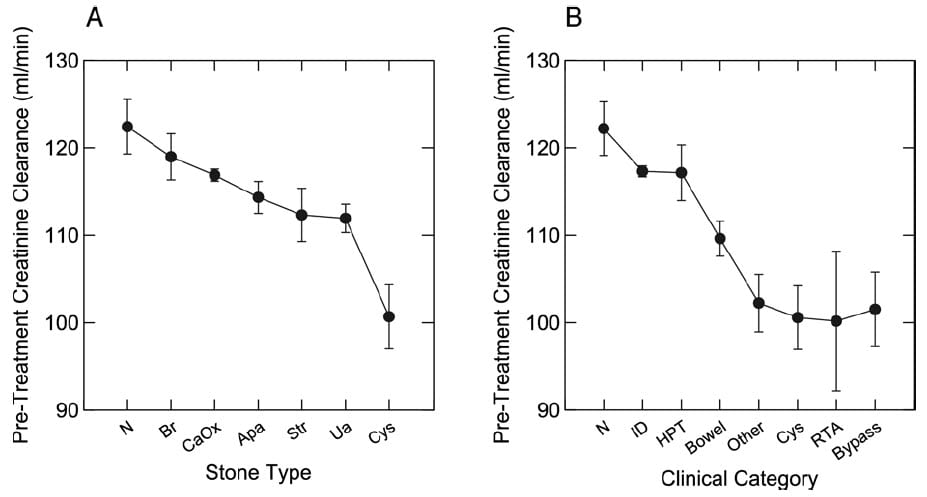
They do. Those with idiopathic calcium oxalate stones (CaOx in panel A and ‘ID’ in panel B) were below normal (N). All patients with stones due to primary hyperparathyroidism (HPT), bowel, or other systemic diseases, cystinuria, renal tubular acidosis (RTA) and obesity bypass surgery were obviously below normal.
Stone type also predicted CCr; apatite (Apa), struvite (Str), uric acid (UA) and especially cystine (Cys) stones associated with lower CCr values.
The magnitudes of CCr reduction were modest on average. If we take 125 ml/min as the normal mean, the most affected groups were down by an average of 20% meaning they had on average 80% of normal function. Cystinuria was lower than that, a fact noted by others before us. So although not normal, kidney function of stone formers might be spoken of as mildly impaired. This speaks to the value of prevention: Of more stones, and any injury or kidney tissue loss. Stone formers have a mild loss that calls for more than the usual precautions against further losses.
Loss Of One Kidney
Because of obstruction or surgical consequences, stone formers lose one kidney often enough we collected many such cases over our long 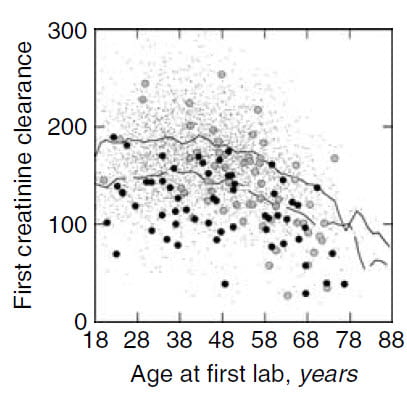 experience. In 2003 we published CCr values over time in those with two and one kidney. Given the general reduction of filtration in stone formers one might expect loss of a kidney to have significant consequences, which is the case.
experience. In 2003 we published CCr values over time in those with two and one kidney. Given the general reduction of filtration in stone formers one might expect loss of a kidney to have significant consequences, which is the case.
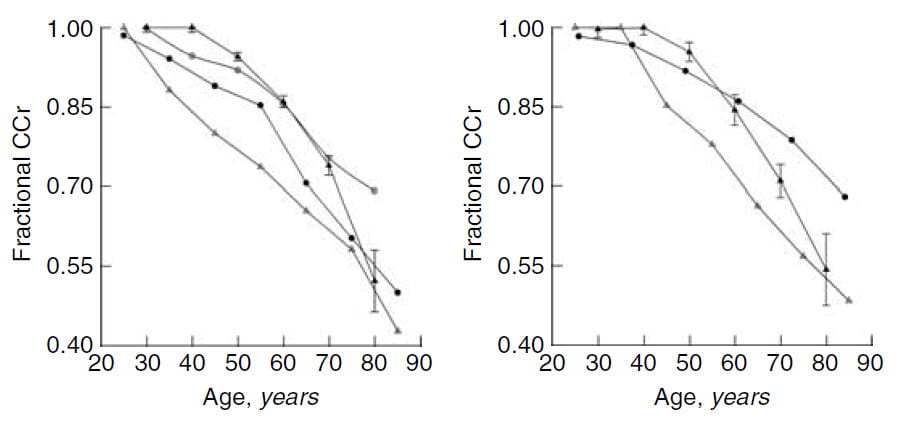
In the graph to the right, average pre-treatment CCr (mean of three measurements) is plotted against age for the two kidney patients (microdots), and those with one kidney (large circles, gray and black for men and women, respectively). Density weighted least square regression lines (solid for men and dashed for women) track the central path of the data for two kidney patients.
These regression lines make clear that CCr hardly varies between age 18 – 45, but thereafter declines in both sexes. Clearances for one kidney women lie below two kidney women, but fall at about the same rate with age. Younger men with one kidney have CCr values more or less at the two kidney level, but CCr then falls more rapidly with age. In later life, CCr of one kidney men and women lies below the lines showing two kidney averages.
This visual impression was confirmed by regression analysis in that CCr decline with age in men is higher with one kidney than with two wheres women with only one kidney lose function at the same rate as women with two kidneys.
Stone Formers vs Normals With Aging
What about stone formers with both kidneys compared to just normal people?
 In that same paper we gathered data from three prior studies that had followed non stone forming people over time.
In that same paper we gathered data from three prior studies that had followed non stone forming people over time.
Here, to the left, kidney function is plotted as a fraction of age 20 to 25. Our data are in black triangles, men are in the panel to the left, women in the right hand panel.
Whereas CCr seems to stay constant in our stone formers until about 40 years of age and then decline (black triangles), normal people display no plateau. Kidney function fell steadily with age throughout life. As a result, at later ages all values generally overlap.
Although you might sense a conflict between these results and those showing lower kidney function in stone formers than in normals, there is no conflict. These two graphs show the changes – or loss rate – of kidney function over time, but not the absolute values as shown in the preceding graph.
Association With Chronic Kidney Disease
Our observational data come from patients at a referral center. How about population studies drawn from a broader community. Does having a history of kidney stones raise likelihood of reduced kidney function outside of a clinic population like ours?
US Population Surveys
Using the NHANES database, we asked if a history of kidney stones associated with reduced kidney function. Indeed, among overweight people, history of stones did associate with reduced kidney function. This suggested to us that loss of function might require multiple insults of which high body weight and stone disease were examples. A subsequent review of NHANES data by other investigators showed that among women but not men a history of kidney stones associated with risk of CKD and dialysis. In other words, whereas we looked only at level of eGFR or serum creatinine, this later study asked about serious kidney disease. It is more common among those who had formed stones.
Local Population Outcome Studies
In Olmsted County, where one finds Mayo Clinic, Rule and colleagues found an association between development of CKD and a history of kidney stones. This reference is to an extensive review by Rule that lists his own population work and all prior studies he could find prior to 2011. In 2012, Rule established that in Olmsted County kidney stone history associated with eventual need for dialysis. Albeit uncommon, the effect was significant. Finally in 2015, our group reviewed all of the prior evidence concerning this topic of kidney disease, blood pressure, and stones. The conclusion was, as with the work by Rule, that association is undeniable.
How Much Risk?
CKD 3 is the entry level for significant disease. In the Olmsted County study about 25% of stone formers met the criteria vs. about 18% of non stone formers.
End stage kidney disease in Olmsted County has a cumulative risk of about 0.6% in 15 years for people without kidney stones. For those with stones, the rate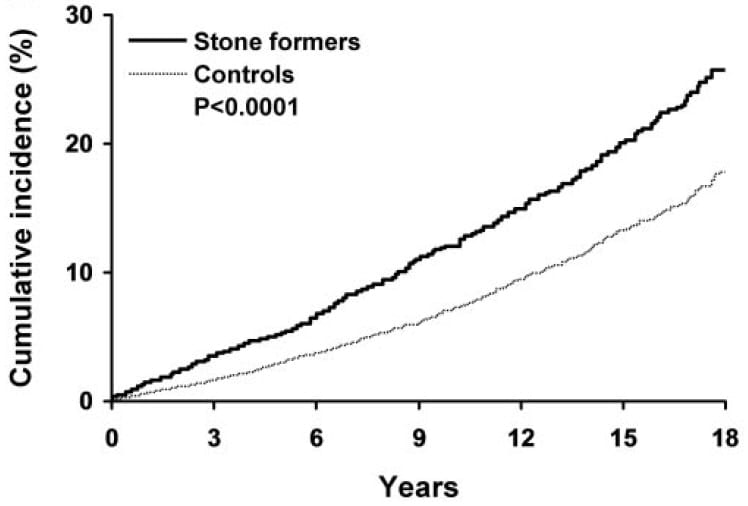 rises to 1.2 – 1.4% depending on the method used for verification. The hazard ratio – ratio of rates – for stone formers vs. controls without stones was about 2 – 2.4.
rises to 1.2 – 1.4% depending on the method used for verification. The hazard ratio – ratio of rates – for stone formers vs. controls without stones was about 2 – 2.4.
In the NHANES study of dialysis need, the odds ratio for dialylsis after full adjustments for confounders was 3.26 (1.48 – 7.16 95% CI). Actual age adjusted values of those needing dialysis (no other adjustments) were 1.61 and 1.52%, men and women, vs. 3.11 and 5.62% men and women with stones. The difference was significant for women not men.
Overview
I have shown you three kinds of data. The first are cross sectional CCr data comparing stone patients in a single center to normals. The second are data from a US national health survey comparing kidney function to people with and without a history of having a kidney stone. The third is a longitudinal study of a local community comparing the outcomes of CKD and dialysis in people with and stone disease. Because Mayo Clinic serves much of this population stones or not could be ascertained more directly.
That all three inquiries overlap in conclusion makes unlikely mere chance has associated stones and kidney disease. Since kidney disease has no mechanism to foster calcium stones – massively the predominant type – and stones a ready way to damage kidneys, association implies causality. Stone forming can damage kidneys and therefore prevention matters a lot.
Hypertension
One might imagine that increased blood pressure would be part of the process from stones to kidney disease. We found an association between stones and higher blood pressures using the NHANES database. The Rule group found it as well in the better documented Olmsted County population, even after one stone.
Taken together, one cannot easily shake the idea that stone disease can indeed lead to kidney disease of clinical consequence and also to high blood pressure. Fortunately the kidney disease only uncommonly leads to dialysis or even advanced CKD. But it does show how important prevention can be.
Last Words About Glomerular Filtration
How filtration works, and how physicians measure it, matter greatly to patients who form stones. Stone formation can lead to kidney disease, usually mild but sometimes significant. Kidney disease consists most essentially in loss of filtration. As well, stone forming may well promote hypertension.
The meaning of these results is simple and compelling. Stone forming patients need to know their eGFR values, and their physicians need to pursue any fall in eGFR with substantial efforts to locate a remediable cause such as obstruction or untreated high blood pressure. Because blood pressure itself appears to run higher among stone formers than in the general population, stone formers need to keep track of their pressures as measured in various medical settings and preferably by themselves at home using good quality OTC devices.
More fundamentally, stone prevention is always the best way to prevent kidney injury from stones. I have advocated remorselessly for early prevention and for sustained prevention. The kidney injury from stones is merely another among many reasons to pursue prevention in the service of a happier and medically sounder life.
Dr. Coe I thank you for all your work. As a past patient of yours, I follow the high volume of liquid each day as well
as a very low sodium and sugar diet. Even after a urologist doing surgery to clean out both kidneys of many stones in May of 2014, I find myself with more there now. I see a urologist in my new home in Nevada every six months and they keep a eye on the kidneys. I also get prolia shots every six months for my bones. My question is should I leave the stones (two are large) in the kidneys since they have not moved, or do I have the surgeon do another clean out of the kidneys? I appreciate your time. Thank you
Hi Midge, if new stones have formed I think your new physicians should consider adding thiazide to the diet. Prolia may have increased urine calcium, as well. I no longer know much about your actual status so this is just conjecture. As for the stones, no; find out first why they formed because if you do not do so and have these removed more may come. Regards, Fred
Thanks I just had an ultrasound and am awaiting results. Also you put me on 25mg of chlortalidone, which the doctor still has me taking. Thanks for your help.
I am currently in CKD 2. I have hypertension, spongy kidney , stones, and a kidney reflux. I am working on low salt, low sugar, low protein, and low oxalate. I need all the help I can.
Hi Debi, CKD 2 denotes a very mild loss of kidney function or else just the presence of some renal abnormalities – like MSK itself. Reflux in childhood can predispose to high blood pressure later on. For you I am sure your physicians emphasize management of blood pressure. Be sure you use 24 hour testing to monitor your sodium intake as guessing does not work. A perfect goal is 65 mEq – 1500 mg – daily. Also valuable for blood pressure: aerobic exercise and minimum body fat – lean and fit. Low oxalate diets are difficult, use your 24 hour testing to be sure you need it. Protein should never be low – 1 gm/kg is ideal and below that not helpful. Regards, Fred Coe
HI,
I’m a young woman (26) who is passing a stone. I don’t know what kind yet, but I’m going to have my doctor analyze it. I’m very worried about getting kidney disease due to this, as well as hypertension. I’m not good with statistics and such. Am I basically guaranteed these things in the long run even if I manage my diet?
Thanks
Hi Rachel, No indeed. Risk is increased for kidney disease and hypertension but certainly most – or many – have no trouble with either. But it does mean one should prevent more. I would read through the book I put together – here is a link to that part of the site. Prevention is not hard, it just needs some organized effort. Regards, Fred Coe
I develop large kidney stones around 2cm. This last one developed in 5 months. I was told I need potassium citrate-citric acid but the pills are too big for me (I had a vertical banded gastroplasty 17 1/2 years ago) and I can’t break it up, it’s hard on the stomach (I have gastritis). The FDA has not ok’d the liquid so my insurance won’t cover it and to buy it I would have to pay anywhere between $50.00-$80.00 a month which I can’t afford. What kind of damage are these kind of stones doing to my kidneys? These big stones have always been on my right side. I have gotten smaller stones on both sides. This will be my srcond surgery to my back (lithotripsy) to get these stones out within a year. Also, I do not have high blood pressure.
Hi Linda, So, the first issue is whether you need potassium citrate. Gastric surgery can itself cause stones, perhaps in your case it has or has not. SO the need here is a proper evaluation and treatment directed at the cause of the stones. Here is a good article you might find helpful. Given such large stones, I worry they are uric acid. Easy to treat. The stone analysis is really crucial here. Regards, Fred Coe
For the past three and a half years I have been producing kidney stones on virtually every incidence of urination. They range in size from slightly larger than grains fo sand to 8mm stones. In number, they range from a few stones to over two hundred in a single pass. I currently have a chain of six stones blocking my right ureter beginning with a 9mm x 6 mm stone down to a 4mm stone. They were not present at all just two weeks ago. IN my right kidney are several stones larger than 10 mm. I currently have a stent bypassing the stones, and small stones continue to work their way through the stent. I am scheduled for surgery in four weeks. Due to extensive hardware in my back, lithotripsy is out of the question so uteroscopy with a laser will be use to remove the big stones. Over this period my creatinine levels have risen from 1.2 to 1.69 and my GFR has dropped from 66 to 40. No one seems alarmed or surprised by this, but it seems disturbing to me. We have tried every treatment in the book without success. I produce both uric acid and calcium oxalate stones in about equal numbers. The calcium oxalate stones are the worst to pass, especially when they are large. I have numerous drug allergies and only morphine reduces the pain level of the bigger stones, but I only take that when the pain is really off the charts. I’ve learned to live with a constant ache in my right kidney. I do produce stones from the left kidney but they generally, but not always, are smaller and much less frequent than the right side. I am astonished at how fast the stones develop. I can have a mostly clear CT scan of my kidneys one day and two days later they are loaded with small and medium sized stones. I drink and pee like a horse, but lately, the stones seem to be getting larger and now, more difficult to pass. I use lemon juice and some tart cherry juice regularly, but there is no difference. I keep looking for information on high output of stones, but find little to nothing and my nephrologist is completely puzzled by the situation. I do have a malabsorption problem in my gut that has recently been associated with stone production. I also have some form of autonomic failure – diagnosed as Multiple System Atrophy. My most recent scans were noted as showing significant atrophic changes in both kidneys including cortical thinning and substantial scarring in the kidneys – presumably from all of the stone production. Is there anyone out there that has done significant research into high stone production and possible ways to minimize it. At one point my nephrologist indicated that she had heard of people actually removing an overprotective kidney, but I keep thinking the other kidney would just pick up the production of stones.
Hi Louis, Very serious problem. Under no circumstance remove kidney tissue because of kidney stones. The uric acid stones are completely prevented with enough potassium citrate to raise urine pH. Please read this articles. This one, too. Calcium oxalate in stones may be coming from the uric acid; otherwise, here is the right approach to prevention. Be sure and get a proper evaluation; here is an article for you. Prevention works, stones will stop. Regards, Fred Coe
Thanks for the helpful information. I will read the articles you recommended and go to my next urology appointment better prepared.
I forgot to mention that for the last five weeks, my stone production has been accompanied by a good deal of blood in my urine. The amount varies, sometimes producing only a moderate cloudiness and sometimes coloring my urine a rusty orange color. I was checked for infection and none was found. I have had a stent in place for three weeks now and I know that can sometimes cause some bleeding. I tend to be anemic and for the last month or two, my hemoglobin has ranged between 10.4 an 9.6. Lately, the amount of discoloration and cloudiness of my urine has increased again. Is that most likely just the stent, or is it something that I should contact my urologist about?
Hi Louis, bleeding enough to lower blood hemoglobin is unusual; your physicians need to figure out what is happening. Possibly your urologist needs to understand why so much bleeding and help stop it. Most of the time blood loss from stone procedures is not so serious as yours sounds. Regards, Fred Coe
Get Renavive it’s fantastic
Hi, I am allowing this endorsement on my site but wish to make clear it is one of dozens of so called kidney stone remedies and probably worthless – I say probably because without trials one can say nothing more. Fred Coe
Dr. Coe,
I am a 43 year old female and just recovered from a kidney infection and sepsis related to a large (18mm stone) on the left side, but also have a 10mm stone on the right side. I found out recently that my father and half siblings have also had many stones. I also had one stone (uric acid) in my early 20s that was smaller and I passed.
My questions are: Can both bilateral stones be removed at the same time? My doctor recommends against it. He plans to use ureterscopy for the large stone on the left first.
I’m concerned about the bilateral stones and kidney disease long term. Of course, I plan to do a 24 urine collection after the surgery and am hoping for drug and or dietary recommendations. I am otherwise healthy, not overnight, normal blood pressure, etc.
Thank you for your feedback,
Cory
Hi Cory, Many surgeons demur to operate on both sides at once. Of great importance is s/he leave you with both kidneys stone free (by CT) after surgery and that you pursue aggressive prevention. The link is to Chapter One of the Kidney Stone Book so you can read through the earlier chapters in order and follow them. Stone analysis is particularly important as uric acid was once mentioned. Regards, Fred Coe
Regards Dr. Coe,
I’m overwhelmed with gratitude for finding such informative articles on Kidney Health. Six weeks ago my husband was taken to the emergency room with extreme renal pain on his left flank. Blood work and CT scans were completed and the findings were as follows… 2mm right UVJ stone causing mild hydronephrosis and dilated left renal pelvis suggesting UPJ stenosis. Seek referral from urologist.
Since then we’ve seen a urologist who begrudgingly ( only after we insisted )prescribed pain medication and flomax. Originally he only recommended drinking water and insisted the stone would pass in 4 to six weeks. Welp, were at six weeks and still in pain even on medication. We’ve been back to our primary physician because mild flank pain has also developed on the opposite side. Additionally bloodwork and another round of CT scans has been performed for comparison at our next urology appr.
Any advice on advocating for ourselves in the situation is greatly appreciated we overwhelming feel like no one has addressed our original diagnosis and we’ve only been symptom masking instead of finding out the big picture. Thank you for your time and knowledge on this matter.
Regards,
Christie ( one concerned wife)
Hi Christie, I am as concerned as you seem. My reading of what research has been done is that obstruction should not last above a few weeks and that the 6 week guideline of the AUA is way too long. Moreover 6 weeks have been lost with pain and all the rest. Your urologist is practicing within AUA guidelines as she/he should, so I cannot criticize anything you have told me. But I would insist that if the stone is still obstructing be be removed – or else that another urologist be consulted. Regards, Fred Coe
Dr. Coe, I can not get a straight answer and am hoping you can help. I had painful urination for a year before a stone grew big enough to block my kidney. At the start of this, a CT scan had been done and indicated multiple stones in the right kidney which is atrophy from numerous kidney infections. Once the stone was removed, the painful urination resolved itself. I passed multiple little stone for 6 months after surgery. When I had the surgery in June 2021, my GFR had dropped to 57. After removal and several months of passing stones, my GFR increased to 96 in Oct 2021. I have kidney stones in both kidneys, left has a 4mm in the lower pole. My GFR has been dropping rather quickly. June 2023 it was 71. December 2023 it was 62. April 2024 it is 54. No one seems concerned that my GFR is dropping that quickly. They also say it can’t be because of the kidney stones. However, I’m a 62 year female, 5’1″, 112 pounds. My blood pressure is normal. I am not diabetic. The kidney stone they removed was 40% burshite. I had no follow-up regarding kidney stones. Why I am producing them, what I should change to reduce them, etc. I also have frequent UTIs. If not caught early, they quickly turn into kidney infections. Am I worrying unnecessarily? Thank you for any advice you can give. Suzanne
Hi Susanna, These variations in estimated GFR may well result from your stones. Brushite stones are very difficult to prevent, grow rapidly and cause a lot of trouble. The linked article is not quite finished but gives you an idea. I would try to get care at a university based stone program as your situation sounds worrisome and is indeed complex. This is not to say your present care is not good but that brushite stones in what sounds like someone with only one well functioning kidney is a very complex problem. Regards, Fred Coe