 How bad is kidney stone analysis?
How bad is kidney stone analysis?
I have pointed out the crucial importance of kidney stone analysis. Likewise, if possible, I analyse every stone because crystal type can change.
But does this not raise the obvious question: How good are stone analysis labs? At first one might say why ask? We use labs all the time and trust them. As things turn out, stone analysis varies more in quality than serum electrolytes, or blood hemoglobin. Moreover, some stone crystals pose greater problems than others.
There is a gold standard
X Ray Diffraction
Basiri et al recently reviewed all available papers concerning analysis of kidney stone crystals. Like prior investigators, some of whom they reference, X-ray diffraction does indeed reveal stone crystal structures and is a gold standard.
You need to sample several regions of a stone because stones can contain multiple crystals. If you do, you can rely on x ray diffraction as the ideal method on which to base research or against which to compare other methods. But commercial kidney stone analysis cannot rely on x ray diffraction – too time consuming and expensive.
High Resolution CT Scanning of Stones
My own co-workers regularly use high resolution CT scanning of individual stones. Although unlike x ray diffraction, high resolution CT scanning of a stone does not reflect crystal structure, it does offer highly calibrated density measurements. These measurements identify stone crystals with considerable accuracy. Moreover, the CT technique shows not only some selected part of a stone but can show the whole stone and reveal its separate crystal components.
Even so, commercial kidney stone analysis cannot use high resolution CT – too time consuming and expensive, like x ray diffraction.
How bad is kidney stone analysis?
Struvite is a problem
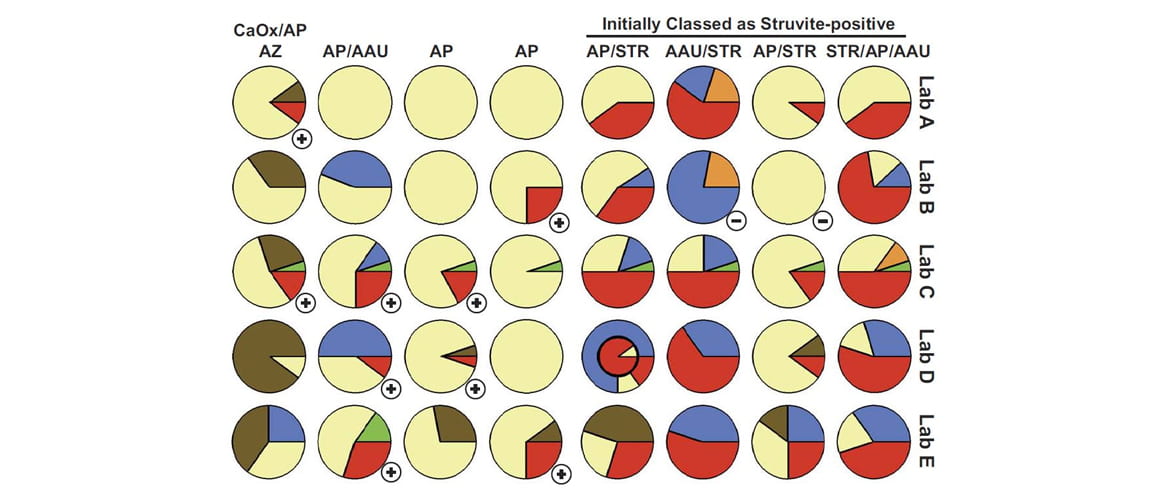
Krambeck et al collected stone fragments whose composition they determined with considerable precision and accuracy. They then sent multiple samples of the fragments to 5 commercial laboratories.
The laboratories failed to detect struvite about half of the time. The featured pictures note this as a negative sign (-). On the other hand, the laboratories reported struvite in stone fragments that had none (+ signs).
Being a result of infection with bacteria that possess urease, struvite stones pose complex surgical and medical treatment problems. The bacteria can produce large stones that grow rapidly and damage kidney tissue. They may super-infect more common calcium stones more easily identified by stone analysis laboratories. Thinking only of those common stones clinicians may miss opportunities to prevent enlargement of struvite fragments not passed or removed at surgery.
Atazanavir, a common antiviral medication was frequently missed
Because of their chemical structures the antiviral drugs often possess spare solubility in urine. This agent is insoluble enough to produce drug stones. All five laboratories failed to detect this drug crystal.
Hydroxyapatite (HA) was missed too frequently
The HA content of stones gives clinicians important clues to renal papillary histopathology, clinical course of stone disease, and even urine chemistries. So the fraction of stones HA comprises matters.
For example, in patients whose stones were >50% calcium oxalate on average, stones were found growing outside the kidney on the papillary surface over deposits of interstitial apatite plaque. Among patients whose stones are predominantly calcium phosphate crystals terminal collecting ducts are plugged with hydroxyapatite deposits. Their phosphate stones are rarely found on plaque but rather seem either to form in free solution or as overgrowths on the open surface of ductal plugs – the end exposed to the urine.
Most remarkably, even the distinction between stone formers whose stones did or did not contain brushite seemed to matter. Those whose stones were entirely hydroxyapatite in their phosphate component formed numerous small tubule plugs whereas those whose stones contained brushite formed few but very large ductal plugs.
Is there a problem?
Struvite and HA failures suggest one exists
I want the highest accuracy in stone analysis, but realize $25 or so per test buys only so much. This study makes one concerned that laboratories frequently miss struvite. Likewise, but less often, they under report calcium phosphate crystals. Even worse, they report struvite when not present, needlessly raising the specter of infection.
Our own research suggests circumscribed failure
On the other hand, commercial stone analyses must possess considerable accuracy if one leaves struvite to one side. Our own research group has pioneered in tissue biopsy of renal papillae of stone forming patients during the course of surgical stone removal. In the course of the work we found a remarkably stable relationship between tissue changes and average stone calcium phosphate vs. calcium oxalate composition.
The analyses for these studies did sometimes arise from the sophisticated methods I have already mentioned. But often, perhaps even usually, they arose from a variety of commercial sources over a period of many years. If random commercial laboratory reports were adequate to support distinctions of such subtlety, how bad can they be?
Likewise, we have published that the percent of phosphate in kidney stones correlates very well with the urine calcium phosphate supersaturation of the patients who produced these stones.
However, these observations concern mainly the calcium oxalate and calcium phosphate crystals, leaving aside the problem with struvite identification.
Do we need more research on this issue?
I would think perhaps we might.
My questions concern the clinical consequences of errors that laboratories make. For example, missing minor apatite components in a stone would make no difference to me. On the other hand, missing apatite when abundant could change diagnosis, prognosis, and even treatment. Likewise, failure to report struvite might delay treatment of infected stones. Failure to report uric acid would obviate proper treatment with potassium alkali.
If I were doing research in this area I might seek designs that capture these kinds of clinical consequences from errors.
Judging from the several references I have shown, we do not yet know the frequency of such consequential errors.
Hi. My stone composition is Calcium Oxalate Dihydrate (Weddellite) 40%
Calcium Oxalate Monohydrate (Whewellite) 40%
Carbonate Apatite (Dahllite) 20%
Is the 20% Carbonate Apatite something to be concerned about?? My urologist did not even mention it to me. I only know because I got a copy of the report. Thank you!!
Hi Cathy, In a way yes, and no. People with 20% CaP often have slightly higher 24 hour urine pH values – 6.3 or higher – and a risk of conversion to calcium phosphate stones that engender kidney tissue damage. So I would pursue active stone prevention. Here is my favorite article on the subject. Regards, Fred Coe
Hello, my kidney stone test reported finding my stone as carbonate appatite at 100%
my urologist was not sure if this is a calcium stone or not. Can you please send me any help or information on what type of stone this is? They report that I have 20-50 of them in both kidneys from my CT Scan. I am determined to resolve this health issue. Thank you so much.
Hi Dee B, It is a calcium phosphate stone, and has its own special problems and treatment opportunities. Here is a good overview of how to get evaluated. The large number of stones makes prevention a major priority. Regards, Fred Coe
Hello is dahllite the same as carbonate apatite? Another doctor said my stones are 100% carbonate apatite dahllite. No one seems to know what causes this type of stone. Thank you.
Hi Dee B, Yes. Carbonate apatite is not rare in kidney stones and reflects an alkaline urine pH usually with high urine calcium excretion. You should get proper testing for kidney stone prevention including 24 hour urine and serum measurements. Treatment is usually effective for prevention of this kind of stone. Regards, Fred Coe
Hello – I received results that say my kidney stone is 20% calcium oxalate dehydrate and 80% carbonate apatite.
Can you please let me know how to interpret these results and move forward? Specifically with diet/medications? My doctor did not provide much information.
Hi XYZ, You are a calcium phosphate stone former. Here is a good review of this special problem. Evaluation for cause is critical, as in the article. Never try prevention without a diagnosis of cause in this kind of stone. Regards, Fred Coe
Hello,
My stones are 85% Dahllite (carbonate apatite) 15% Struvite (ammonium magnesium phosphate) I had the 24 hr urine tested done but my doctors still won’t tell me how to prevent future stones. I heard struvite is from uti but I have never had one in my life. I am so afraid of another blockage.
Calcium, Urine 24hr 100.8 100.0-30 0.0 mg/24h
Sodium, Urine 24hr 154 39-258 mmol/day
Phosphorus, Urine 24hr 468.8 400.0-1300.0 mg/24h
Uric Acid, Urine 24hr 419 250-750 mg/24h
Potassium, Urine 24hr 44.3 25.0-125.0 mmol/day
Chloride, Urine 24hr 149 110-250 mmol/day
Citric Acid, U, 24hr 302 L 320-1240 mg/24h
Oxalates, Urine 24hr 19 4-31 mg/24hr
Magnesium, Urine 24hr 93 12-293 mg/24h
Sulfate, Urine 24hr 26 0-30 mEq/24 h
Cystine, Urine 24hr 9.79 L 10.00-100.00 mg/24h
Osmolality, Urine 448 300-900 mOsm/kg
Creatinine, Urine 24hr 998.4 800.0-1800.0 mg/24h
pH, Urine 6.3
Ammonia, Urine 24hr 30 Not Estab. mEq/24 h
Calcium Oxalate 2.41 0.00-6.00 ratio
Brushite 0.77 0.00-3.00 ratio
Monosodium Urate 2.84 0.00-4.00 ratio
Uric Acid 0.59 0.00-1.20 ratio
Struvite 0.04 0.00-1.00 ratio
Also all my urologist says is drink lots of water, last year I had to have a stone removed in my right after causing a blockage in my tube and I have one in my left with mild hydronephrosis and has not moved or grown.
Hi Nikki, Water is always a good thing, I have added more below. About the obstructing stone, be sure your surgeon has every opportunity to observe things, as obstruction can damage kidneys – the left stone sounds a bit worrisome. Regards, Fred Coe
Hi Nikki, Your urine is a bit alkaline and has low citrate, and you form calcium phosphate stones – this is not an unusual pattern. The struvite is worrisome as it is from infection, but it may be an error. Stone analysis is not so good about struvite. Your urine ammonia is not very high and with bacteria producing struvite one expects it to be higher. As a check, your physicians can culture your urine to see if stone forming bacteria are present. Usually removed stones are cultured – perhaps yours? Your urine SS are all very low, so stone risk is not high right now, this makes me wonder if a lot has changed since you formed the stones. Regards, Fred Coe
Hi! My X-rays came back negative for any more stones, could a CT find more? I’m still in some pain. My stone was 90% carbonate apatite, and 10% calcium ox
Hi Casey, Indeed a CT is a low better than a plain x ray. Given phosphate stones you need a full evaluation and treatment for prevention. The linked article is my best. Regards, Fred Coe
A recent kidney stone analysis revealed a stone composition of 80% Carbonate Apatite (Dahllite) and 20% Calcium Oxalate Dihydrate (Weddellite). Past stones were comprised mostly of Calcium Oxalate Dihydrate. As a result, a nephrologist put me on a large daily dosage of Potassium Citrate which should be capturing the Oxalate over the past 4 years. Now I am apparently producing Carbonate Apatite stones in the absence of the excess Oxalate.
That being the case, a brief scan of the literature indicates a somewhat weak linkage to infection and the production of Carbonate Apatite stones. If we rule out infection, what is the method of formation of Carbonate Apatite and what should I avoid in my diet (or add to my diet) to prevent Carbonate Apatite stones? Alternately, would better hydration with water correct the pH of my urine such that Carbonate Apatite would not form and precipitate out of solution to form stones?
Hi Robert, Conversion from calcium oxalate to calcium phosphate stone is not so rare – we reported on it years ago. Potassium citrate prevents calcium oxalate stones – I presume by raising urine citrate, a powerful calcium binding agent that inhibits calcium crystal nucleation and growth. The higher urine pH from potassium citrate may have converted your stone type. Here is a pretty good overview of calcium phosphate stones, which you now form. Potassium citrate has never been tested in calcium phosphate stone formers, so I presume alternative treatment is now needed – usually urine calcium is high, and given the tendency for calcium phosphate stones to become rather large and numerous, thiazide might be a best alternative. Of course your personal physician is responsible for your care, and my comments are just that. Regards, Fred Coe
I started passing calcium oxolate stones and told to drink 12 glasses of water a day, which I did and keep passing stones over the years. Then I found your site and took Jill’s course. And eat low salt, low sugar, low oxolate. This year I had a 13 mm struvite infected stone and my urologist told me to make sure I take my antibiotics every day. and 1 week ago I passed a carbonate Apatite stone. I also have vesicoureter reflux and on a daily antibiotics. I have called my nephrologist to see about changing antibiotics. I feel like I just can’t win with kidney stones.
Hi Debi, Struvite arises from infection with bacteria that can make the crystal. I suspect you became infected because of your prior stones, and now have a new problem. Struvite stones are a mixed surgical /medical issue – infected stones need to be removed and antibiotics used to sterilize the kidneys when stone free – stone free outcomes from surgery are very important for this to work. The diet will not help infection stones, unfortunately, but is healthy and helps prevent more calcium oxalate stones. Regards, Fred Coe
I am feeling a bit concerned. I’ve had 2 surgeries. My Kidney Stones result is Ammonium-Magnesium Phosphate Hexahydrate (Struvite) 60%
Carbonate Apatite (Dahllite) 40%.
Any feedback would be very helpful.
Hi Zakeye, Your stone forms because of infection with bacteria that convert urea – present in all human urine – into ammonia. This is a very complex kind of stone usually requiring surgery and very enlightened medical aftercare. I really need to write an article about the problem. Regards, Fred Coe
Hello Dr. Coe,
I was wondering if you could give me any insight on the type of stone, based on the analysis I received:
– Calcium Oxalate Dihydrate (30%)
– Calcium Oxalate Monohydrate (35%)
– Carbonate Apatite (35%)
I am in my mid 20’s and have produced at least 4 stones over the past 15 years, but this is the only one I was able to get analyzed after surgery. I had done a 24-hour urine test about 8 months prior to this stone (because of a different stone) and my doctor had said all she saw from that test was that I need to increase my fluid intake. I also have never had a UTI to the best of my knowledge, so that Carbonate Apatite is a little confusing to me. I appreciate any feedback. Thank you for the work that you do!
Hi RC, It is a calcium oxalate stone highly enriched with calcium phosphate. This usually arises from increased urine calcium and urine pH. Younger women often have increased urine pH vs. med and vs. themselves at a later age I suspect that although your 24 hour urine values are all ‘normal’ apart from volume, a closer look might reveal stone risks. Take a look, regards, Fred Coe
Hello, I’ve been having kidney stones for 15 years, countless surgeries of every kind, currently 28 weeks pregnant with a nephrostomy tube in my left kidney with two cyst, and at least 5 stones they can see with the ultrasound, I feel like I’m always in pain from passing stones or infections, this is my most recent stone analysis calcium oxalate dihydrate (weddellite)20% carbonate apatite (dahllite) 80%. Many drs tell me it’s hereditary, a two years ago I had a stag horn the size of a fist in my right kidney removed. Please help 😔
Hi Ka, Calcium phosphate stones are often very recurrent and can grow rapidly. Given prevention efforts have been unsuccessful, I would suggest your physicians might want to seek a consultant to help out. With modern telemedicine, that person can be anywhere. Regards, Fred Coe
I had bilateral stones–the largest (8mm) was removed at the end of November. Results are showing as:
Calcium Oxalate Dihydrate (Weddellite) 25%
Carbonate Apatite (Dahllite) 50%
Ammonium-Magnesium Phosphate Hexahydrate (Struvite)25%
Had pain off and on from May-October. 4mm stone was removed and then this larger 8mm which had begun to cause some mild hydronephrosis was then removed after a stent had been placed to enlarge the ureter.
I will have a consult with my urologist to discuss this and the 24 hr urine sample, but love any additional insight. Thank you.
Hi Josh, This is very complex disease. Dahlite stones are a special problem – calcium phosphate, oxalate plays no role. Mg ammonium phosphate stone is either forming because of infection or has been mislabeled by the lab. That is not rare for this crystal. KIDNEY STONE ANALYSIS: How Bad is It?You need very complete 24 hour and serum testing to figure out why you are forming this kind of stones. Regards, Fred Coe
Hi. I was 24 years old at the time when I had this stone analysis done after I was admitted with 2 obstructive kidney stones, a UTI, and sepsis. I wasn’t told what the cause or what the stone was made out of. I just had surgery at age 25 for the last kidney stone but haven’t gotten those analyzed yet. What were my stones made of the first time? This is what I got from QuestDiagnostics;
Calcium Oxalate Dihydrate (Weddellite) 40%
Calcium Oxalate Monohydrate (Whewellite) 40%
Carbonate Apatite (Dahllite) 20%
Thank you for your time.
Hi Allena, basically you have calcium oxalate stones, the 20% calcium phosphate suggest a high urine alkalinity – pH – which will be clearer when you get your 24 hour urine studies. Do a full evaluation and treat what is wrong. Do analyze the newer stones, too; they may have more phosphate in them. Regards, Fred Coe
Hey, I’m 32 and just had my first surgery to remove a stone that came out of the kidney and got stock in the Urinal. and I have one more in the other kidney. the lab results are:
weddellite
weddellite
carbonate apatite
50/45/5
what is that mean?
and how do I make sure it wont happened again?
Thanks a lot!
Tamar
Your stone is calcium oxalate dihydrate, the common one. A full evaluation should disclose the cause and the means for prevention. Regards, Fred Coe
Hello ,
My son (10 years old at the time is now 11) passed a stone on December 5, 2021. Recently got the results back and I have no clue what I am looking at. He goes to Pediatric Urology in a month, but would be nice to have an idea of what there talking about in the mean time. He passed a 4mm kidney stone with the following results.
Calcium Oxalate Dihydrate (Weddellite) 60%
Calcium Oxalate Monohydrate (Whewellite) 20%
Carbonate Apatite (Dahllite) 20%
DNR and weighed .15g.
This is a new world for as I have Neprocalcinosis of the righg kidney but have never produced stones. Any thoughts would be so helpful. Thank you for your time
Nicole
Hi Nicole, Children with stones usually have genetic high urine calcium.But some have uncommon diseases. So all need 24 hour urine and serum testing.This is bests done before the visit so the results are available. That you have some form of stone disease is itself not rare, the disease is very familial. You should probably be tested as there are uncommon diseases in which mothers have a mild version and their sons a more severe version. The stone is the common calcium oxalate stone and because the COD predominates I suspect high urine calcium – so called idiopathic hypercalciuria. Regards, Fred Coe
I suffer from chronic kidney stones which started in High School. I am now in my 30s. Past stones have been made up of Oxalate but now I am beginning to have LARGE stones. Most recent made up of: Carbonite Apatie Dahllite 85% and Ammonium Magnesium Phosphate Hexadydrate STRUVITE 15%. What does this mean exactly? What can I do to prevent further stones? Treatment options? I due to have ESWL this month.
Hi Brittany, I suspect you are transforming from calcium oxalate to calcium phosphate stones, and usually the problem is a rising urine pH and too high a urine calcium. The struvite component may be a lab artifact or possibly your urine is colonized with bacteria that can make this crystal.Everything depends on the serum and 24 hour urine study results, which you have not forwarded. Look there for the answer. Regards, Fred Coe
I’m a 42 yr old white male in great physical condition in the hospital now after having PN surgery on my right kidney( my left was done last month removing two 2CM stones). I had a 5cm in my right and that was mostly removed along with smaller stones, this surgery was done 3 days ago. because he said my stone was grown into my kidney and he wasn’t able to get it all, he hopes to get the rest next surgery. He is also doing biopsy on kidney tissue, until then I have a tube in my back draining. My analysis came back on my stone this morning from large 5CM stone which showed it was a 100% Carbonate Apatite (Dahllite). I have had stones in the past and received shockwave therapy. Last episode was 2010, I was able to pass them with a stent. I was told then in 2010 that I had several other stones that were in a spot I didn’t need to worry about immediately, I’m assuming the little stones I didn’t need to worry about are what turned into a 5 CM stone. I will do a 24hr urine analysis once I’m back to normal. Is this really uncommon what I’m going through and do you have and suggestions?
Hi Jason, Phosphate stones can grow rapidly and large, like yours did. The carbonate part implies a high urine pH (alkaline urine) of considerable degree so the 24 hour urines will be very important. Prevention is crucial as recurrence is likely. The goal is to lower the saturation with respect to calcium phosphate – this measurement will be on the lab report. It is measured with respect to brushite, an initial calcium phosphate crystal in human urine. Regards, Fred Coe
Hi Frederic.
My 3 y.o son has a 2cm stone in his left kidney causing hematuria, but not pain.
He also has an UTI with Proteus mirabilis that doesn’t disapear even with antibiotic therapy.
He recieved a first shockwave therapy, that, after a year, had virtually no effects.
His stone was analyzed through pieces we found in his urines and collected, it’s 60% Carbonate appatite, 20% Struvite and other 20% are calcuim and some other small percentages.
My questions are :
1- does inhibiting urease from P. Mirabilis with phenolic acids like Vanillic acid from vanillin may induce a decrease in the growth rate of it’s stone ?
2- Are shockwave therapies good, when repeated and agressive (we talked about 4 procedure a year with the surgeon) ?
3- Is it possible for the UTI or the stone itself to endamage his kidney and make it disfonctionnal or dead ?
3.a- In such a case, wouldn’t it be better to surgically remove the stone for once before it happens ?
Please note that he never had sepsis and the infection was under control and he is tested every month for this. Usually, the infection is P. Mirabilis 10*4 but never disapears.
He had many echography that showed no kidney disfonction of malformation.
We made urine test that shows a good creatinine/cystine ratio.
We found only 1 time out of the 10 times we tested his during this year, the presence of crystals in his urines. It was ammonium + magnesium + phosphate (struvite i guess). In april 2022.
We’re very affected since his stone is very big and the infection is there, colonizing the stone for a year now.
Thank you very much for all your work.
Reading you website and educating myself about this problem is a real source of hope as a father.
Hi Shawn, Given the crystals I imagine you are right and it is a struvite stone from Proteus bacteria. Multiple SWL is not ideal in a child or adult, and your child is in a very high complexity situation. He should be treated at a major university based Children’s hospital that has special expertise in management of this kind of problem. If you tell me where you live I can try to identify possible places near you. You are wise to inquire. Regards, Fred
Thank you so much for replying.
We are from France, Lille (northen france) to be more precise.
Despite all this he is a normal child with good health.
The UTI is kept under control and I created a regimen of analysis we have every 2 weeks consisting in checking his urine with a lab test. Full cytobacterioligical urine exam, crystal analysis (the last one came without any crystal 06/25/2022) and creatinuria (not made on 24h but in the second urine after waking up).
His two kidneys develops at the same rate and there’s no trace of dilatation or kidney problem with the multiple echography we made.
Parenchyma seems intact and in good condition.
A doctor adviced us to do a scintigraphy DMSA to evaluate his kidney health more precilsy but i have to say that between the 5 radiological exam he already had and this new scintigraphy DMSA i start worrying about his radioactive exposition … I also question the necessity of this new exam that seems very heavy, especially for him at only 3.5 year old.
I thank you again for everything you do, because you are a real carrier of hope for me and my familly.
Hi Shawn, Given the struvite in the stone, one might want to measure urine ammonia – high levels in relation to urine sulfate signify active urea hydrolysis by bacteria in the stone – it is how such stones form. Low values are reassuring. Regards, Fred Coe
I recently had a PCNL in my left kidney, the stone is still there 8mm and tight kidney 7 mm. Sent the stones for analysis, got back with:
Carbonate apatite (Dahlite) 40%
Ammonium urate 31%
Struvite 29%
My doctor prescribed me to take magnesium citrate for a month and do the ultrasound again.
My husband has kidney stones. After the analysis done with FT-IR:
Dahlite 90%
Struvite 10%
What can he do to prevent them and cure them? We live in Italy and it seems they treat all stones the same. He’s always has major pain when they occur. They give him a few shots of Tora-Dol to try and ease his pain but many times this just takes the edge off but nothing else.
Thank you for any help you might be able to give.
Amelia
I wanted to include the fact that he takes pantoprazolo for acid reflux as well as maalox and/or bicarbonate. I read that these can cause stones.
Thanks again.
Hi Amelia, possibly these can matter, but it is better if you can contact Dr Gambaro who either him self or someone he knows can sort things out and get some prevention against the stones. The calcium phosphate stones are of much concern and prevention correspondingly important. Regards, Fred Coe
Hi Amelia, Dr Giovanni Gambaro is a noted expert in stone prevention in Italy. I know him personally and suggest you contact him – I believe he is in Verona. Regards, Fred Coe
I have been dealing with kidney stones since 2009. They reoccurrence of stones has gotten worse since 2014. I’m hospitalized at least twice a year with SWL twice a year, stents and I’ve had a nephrostomy tube x2. My most recent hospitalization was in July. I had a stone analysis on August 25 100% Dahllite then an analysis on September 1, 20% Struvite 80% Brushite. The stones were obtained after SWL on August 19 and August 25. I’m just so confused about how can these be treated. I have a 24 hour urine study to do in 2 weeks. I always have stones in both kidneys, even currently. As soon as they do SWL more stones form. They are usually 7mm -1.3cm one year. I would love any feedback. It’s affecting my life and employment. I miss a lot of work due to my episodes. Thank you for any advice.
Hi Carla, Brushite stones are indeed rapidly growing and require very aggressive treatment for prevention. Ureteroscopy is the usual approach because they are hard and difficult to break with extra corporeal shock wave treatments. This is generally true for all of the phosphate stones. Given your chronic problem perhaps your physicians might want to refer you to a convenient university program, because prevention is rather complicated and you may have other issues from the many stones and procedures. Regards, Fred Coe
Hi Dr. Coe,
I had 9 stones removed from my right kidney from 7mm-3mm recently via cystoscopic lithotripsy.
Analysis came back as 100% carbonate apatite (Dahllite)
My urologist also said Randall’s plaque was visualized in that kidney as well during procedure. They gave me IV antibiotics day of procedure and a 5 day course of cefalexin. I have asked about next steps to prevent these and they really don’t have much to say……
Do you have any recommendations for university programs near Harrisburg, PA?
Thank you!
Hi, You are in reach of U Penn in Phila and Hopkins in Baltimore. Both are outstanding. Fred
Hi,
I too had a stone analysis came back as 100% carbonate apatite (Dahllite). Any idea what could cause this?
Hi Mikala, This is a form of calcium phosphate stone. Here is the article that best fits this problem. See if it helps. Regards, Fred Coe
Hi Mikala, This is a calcium phosphate stone, and this article concerns them specifically. I hope helps orient your thinking about what to do next. Regards, Fred Coe
Greetings Dr Coe
Thank you for taking time to write such an informative article . I am losing faith battling constant reoccurring staghorn stones
I’ve had over dozen surgeries in past decade . My first dr was amazing and kept me stone free for a cpl years but retired & the last dr I saw was horrific and dismissive . She conducted one failed attempt surgery – only retrieving a couple stones (whereas I have estimated around a dozen in both kidneys right now)
The one and only follow she gave me after surgery she spent 5 minutes w/me to remove stents and said I was too complex & to find a new Dr?!? Leaving me with all these infection stones & w/out even a refferal
I am still in shock of her care & treatment
Having been fighting these for a while – I am afraid she may have made things worse by going in and trying blast them but failing at removal. She literally wrote in surgical report was too bloody couldn’t see?!
I fear it’s just a matter of time until I go septic again. I have been spending my days googling Drs and trying to find one who CAN & will help me. As you know these types of stones are highly infectious and shouldn’t be left – do you have anyone you’d recommend in CT? (CONNETICUT)
Hi Your instincts are correct, struvite stones are dangerous and complex to manage. One resource is the University of Connecticut, but I did not find a stone program there last time I looked. Another is NY if you can get there. Dr David Goldfarb at NYU is a real expert and works with surgeons who are of a very high caliber. REgards, Fred Coe
I was diagnosed in 2017 with medullary sponge kidney and nephrocalcinosis. I have had 3 stone analysis done in this time and each time, they have changed composition. The most recent one showed carbonate apatite (dahllite) 100%. I currently take 50mg HCTZ, flomax and tricitrates. What else needs to be done?
Hi Cathy, I doubt the MSK and suspect it is the phosphate stones doing all of the evils. I am not sure about the tricitrates as they increase urine pH and increase stone forming propensity for dahlite. I am sure your urine pH is too high all the time, citrate low, and urine calcium likely high, but I do not know this. I do know in your case detailed evaluation is crucial, and strongly advise it. If the urine testing includes supersaturations, the one to follow is that for calcium phosphate. Regards, Fred Coe
Thank you so much for your quick response. I have not been able to find a urologist that is knowledgeable in MSK in my local area. I have heard that I should not have chronic pain with non-obstructing stones from almost every doctor I have had encountered whether it is my primary doctor, ER, urologist, etc. CT scan from today says nonobstructing right renal collecting system stones. I have been reading up on the carbonate apatite stones and saw articles that mention that they can be infected. Just trying to do as much research as I can to be informed as well as be able to advocate for myself.
Thank you so much for your quick reply. I was diagnosed with MSK back in 2017. My first stone analysis (2017) showed 50% Calcium oxalate monohydrate, 40% Calcium oxalate dihydrate, and 10% Calcium phosphate (apatite). My second analysis (2021) showed 60% Calcium oxalate monohydrate, 30% Calcium phosphate (apatite) and 10% Calcium oxalate dihydrate. Most recent analysis (2/20/23) was Carbonate Apatite (Dahllite) 100%. I only see my nephrologist once a year (her suggestion) since she said there is nothing more she can do for me “medically speaking” (her words). I have reached out to her regarding the recent change in composition and have heard nothing back yet. I am afraid to keep using the tricitrates, especially since I am reading that the calcium phosphate stones are the hardest to treat and that they form in alkaline urine (urine pH is always above 7). I am using a herbal tea that my sister in Christ brought to church for me that includes dandelion, ginger, marshmallow, ginko and red clover. Any other suggestions or recommendations are appreciated. Would it be possible to have my nephrologist reach out to you for help with treatment?
Hi Cathy, I do not see where you have had 24 hour urine studies but you do need them. With calcium phosphate stones, your high urine pH is an important factor, but urine calcium loss rate is equally important, and urine citrate as well. You might want to ask your physicians to make a complete evaluation for cause. You are on hydrochlorothiazide which may not be as effective as longer acting drugs such as chlorthalidone or indapamide, but before doing more testing is best. Regards, Fred Coe
I have had several 24-hour urine tests and would love to send the results to you to analyze. Would you mind sending me your email?
Hi Cathy, If I interpret your results one on one it is practice medicine and that requires a formal visit, record, etc. Often people post results and I an free to comment on the results in general, which is not medical practice but merely laboratory data. Regards, Fred
Dr. Coe, My daughter has several stones measuring up to a 9mm stone in the lower pole of her left kidney
– Carbonate Apatite(Dahllite) 100%.
She is 26 weeks pregnant.
What are her options for treatment? Can you recommend an expert treating pregnant women with this condition?
We are in Connecticut. New York and Boston are also doable. Thank you for your assistance
Hi Ginny, During pregnancy one cannot do much about prevention. In NY Dr David Goldfarb at NYU is outstanding and your best alternative. Regards, Fred Coe
Hello Dr Coe,
I had a kidney stone and received the following lab results but am unclear what in my diet may have caused it. Any idea from the results?
Calcium oxalate dihydrate (weddellite) 20%
Calcium oxalate monohydrate (whewellite) 60%
Carbonate apatite (Dahllite) 20%
Thank you!
Hi Rick, You need a proper evaluation. Your kind of stone usually goes with high 2r hour urine calcium and pH. But testing is a lot better than guessing. Regards, Fred Coe