Kidney stone types

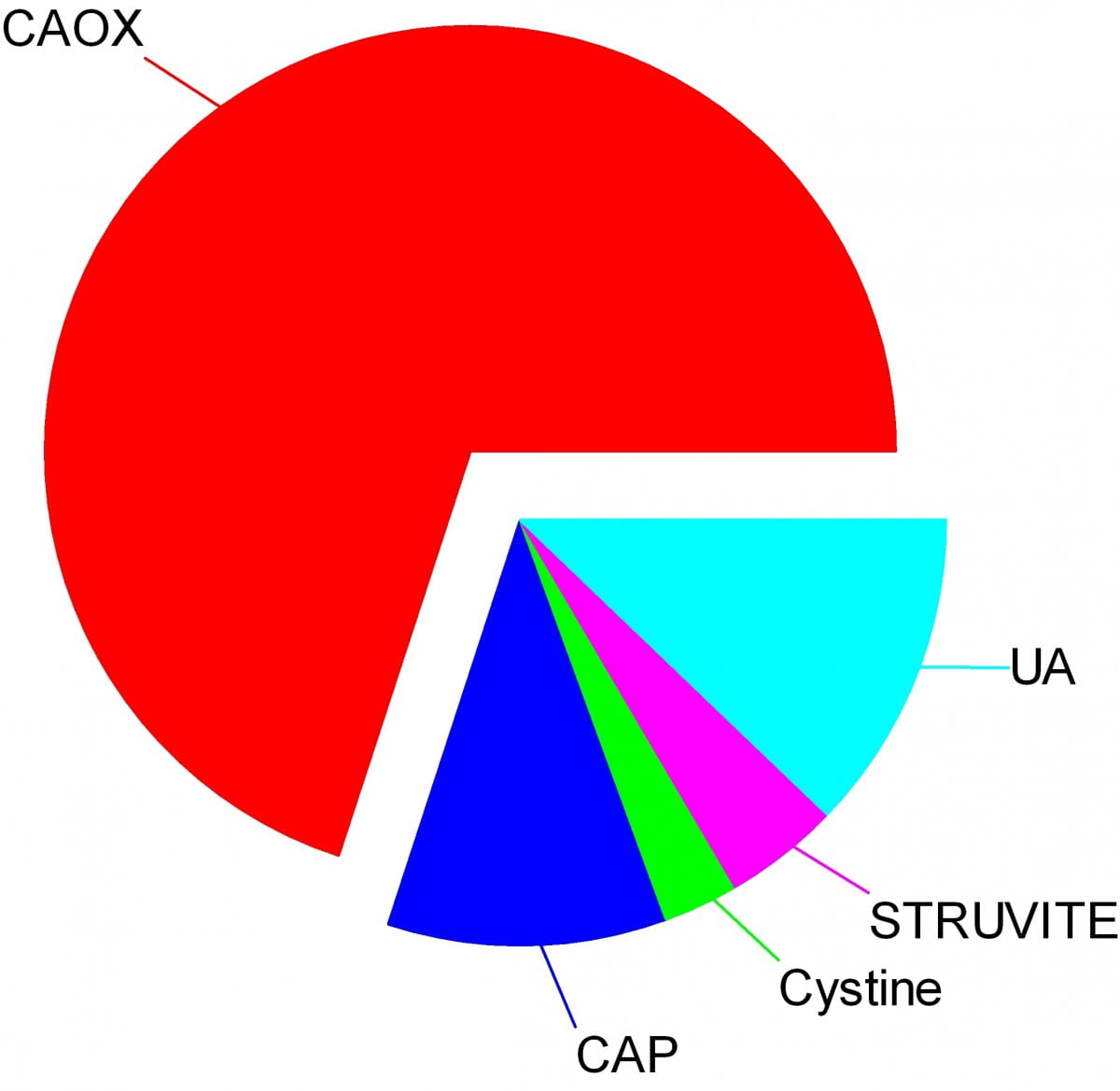
Crystals make stones and their names signify the kidney stone types. Here are the names of the crystals that make the stones: CAOX, Calcium Oxalate; CAP, Calcium phosphate; UA, Uric Acid; Cystine; Struvite.
The wedges on my pie chart show the relative abundances of stone types in our large population of stone forming patients. Calcium oxalate stones predominate by a wide margin in our clinic and in all others I know of.
The names, matter because the whole science of stone prevention focuses upon stone crystals. Each kidney stone crystal creates its own unique illness and requires specific treatment. That is why we name stones by the names of their crystals and why when stones are analysed the results are reported by these very same names.
Being a bold and rather large graphic, the featured picture does what I intended, brings the main facts into view as, at a circus, the great animals and the small animals circle the ring by way of an introduction. Come. I will show you all the common stones, like at a fashion show, or a circus parade. You can watch as they go by and remind yourself, or wonder, which ones might have been yours.
Here they are.
Which type do you have?
You might think your doctors know what stones you have formed, but don’t rely on it. People move, doctors move, health records are far from ‘all electronic’. That stone report from 4 years ago could lie in a dusty filing cabinet, your new doctors unaware it exists. Worse, it could hide in a dresser drawer and you forgot it you put it there. Perhaps even more worse, the stones might stay in that drawer, never analysed at all. Find the stones, find missing reports, urge analysis by your physicians. They can help you most if they know your stone analysis.
When they do not know, physicians can still mount prevention efforts but with less focus and probably less effect than when guided by a knowledge of the crystals. So always seek treatment. If a stone comes along the way, make every effort to get it analysed.
Why should you care to know all this?
Because you will conduct much of your own treatment, and over many years.
Since stones tend to recur, prevention requires treatment over long periods. These treatments work by altering urine chemistry in a direction that minimizes the risk of forming crystals. Such altering of urine chemistry requires control of fluid intake, lifestyle, and diet, and sometimes additional use of medications.
Just as the sailor who aims along a chosen track against the random, misdirecting, confusing sea and air maintains a constant way in proportion to that skill which comes from knowing the way of the boat, patients who aim to keep a certain kind of condition in their urine despite the demands and temptations of the world do so, I believe, in proportion to skills that come from knowing how their work and lives and foods affect their bodies, and how those crystals form which they so much desire to prevent.
Put another way, knowledge is power.
Why is this article so long?
I wanted to put all five main types of kidney stones. That makes a long story. But probably you will care to read about only your own type.
I should mention here, to save a lot of confusion, that stones often contain mixtures of crystals.
The pie chart refers to the most common crystals in a stone, for which the stone is usually named. Much of the time, minor crystal components are not crucial, but sometimes – to jump forward a bit – they are. Even a trace of struvite or cystine, for example, can have great diagnostic importance.
Calcium stones
Calcium Oxalate Crystals
In the great circle atop this page article, the calcium oxalate stone, being most common, occupies a lion’s share of the space. 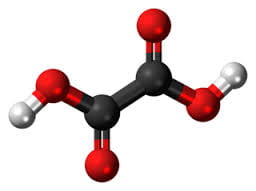
The calcium oxalate crystal forms when calcium combines with oxalic acid. Oxalic acid (at left), a dead end waste product that the kidneys remove, contains two carbon atoms (the large black spheres), four oxygen atoms, and two hydrogen atoms (silver).
At the acidity of urine, the positively charged hydrogens leave their negatively charged oxygens. As a result the oxalate molecule carries two negative charges. In the figure at right one negatively charged oxygen attracts the hydrogen of a nearby water molecule (H – O -H) while another attracts a positively charged calcium atom.
You can imagine how another oxalate ion (the name for a charged molecule in water) could attract the same calcium, or another calcium atom attract the bottom oxygen on the oxalate molecule so the chain extends and makes a crystal. You can see more about this in a video I made. Broadly speaking – though my more expert colleagues may bridle at such a simplification – the calcium atoms and oxalate molecules combine by the attraction of their opposite charges.
The calcium oxalate kidney stone comes in two varieties, calcium oxalate monohydrate and calcium oxalate dihydrate. The former are harder and therefore more resistant to fragmentation by lithotripsy. Likewise, the former appear more often when elevated levels of urine oxalate are present.
Calcium oxalate stone formers
From Systemic Diseases
Sometimes this kidney stone arises from a systemic cause, like bowel disease, primary hyperparathyroidism, or primary hyperoxaluria. Only physicians can establish that a known disease – like bowel disease – is the cause of stones. Only physicians can discover underlying primary hyperparathyroidism as a cause of stones. Patients cannot do much for themselves except provide as complete a medical record as possible.
Idiopathic
Most of the time this kidney stone arises simply from the interplay between inheritance, diet, and aspects of daily living. We call such patients idiopathic calcium oxalate stone formers, from Greek ἴδιος idios “one’s own” and πάθος pathos “suffering”.
Even though physicians discover the links between daily living and stone production, and select those changes that can prevent new stones, patients themselves must create and maintain those changes. I believe patients can so this in proportion to how well they understand what is needed, and why. When changes in daily life are not enough, physicians add medications, so even then patients remain active therapists for their own disease.
Stones usually form on kidney surfaces
About one million nephron units make up a normal adult kidney. The calcium oxalate kidney stone type does not grow in the tubules of the nephrons but ‘outside’ them, on the surfaces of the renal pelvis where final urine collects and drains through the ureter to the bladder. Here is a video that shows how they can form.
Calcium phosphate crystals
Phosphate ion and urine pH
Calcium phosphate stone crystals form when calcium atoms combine with phosphoric instead of oxalic acid and produce the calcium phosphate kidney stone.
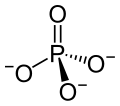 Phosphoric acid is simply a phosphorus atom (shown as the ‘P’ in the line drawing to the left) with 4 oxygen atoms bonded to it. One oxygen atom has two lines for its bond to phosphorus; this oxygen cannot provide any charge with which to bond calcium atoms to make a crystal. The other three have ordinary bonds that are shown by a line, and a dashed and solid arrow. These two arrows mean simply that the oxygens lie above and below the plane of the paper – so if you built the molecule with sticks and balls it would have a three dimensional shape.
Phosphoric acid is simply a phosphorus atom (shown as the ‘P’ in the line drawing to the left) with 4 oxygen atoms bonded to it. One oxygen atom has two lines for its bond to phosphorus; this oxygen cannot provide any charge with which to bond calcium atoms to make a crystal. The other three have ordinary bonds that are shown by a line, and a dashed and solid arrow. These two arrows mean simply that the oxygens lie above and below the plane of the paper – so if you built the molecule with sticks and balls it would have a three dimensional shape.
One of the three negatively charged oxygens never has a hydrogen on it in urine but only in exceedingly acidic solutions. A second charged oxygen is always occupied by a hydrogen atom in urine.
This makes the third oxygen, variably occupied by a hydrogen in urine, a tie breaker.
In a urine of average normal acidity (pH around 6), most of the tie breaker oxygens have their hydrogen leaving the phosphate ion only one negative charge. Not enough to make a crystal.
When the urine is abnormally alkaline (pH above 6.3 or 6.5), the variable oxygen becomes charged so the ion has two negative charges that can combine with calcium to make crystals. For this reason the calcium phosphate kidney stone tends to occur in people who produce a more alkaline urine than those who produce calcium oxalate kidney stones.
Brushite vs. hydroxyapatite
Much like calcium oxalate, calcium phosphate crystals begin simply as one to one pairings of doubly negative phosphate ions with doubly positive calcium atoms. This initial crystal is named brushite. Brushite, which is an equal mixture of calcium and phosphate ions, can convert to hydroxyapatite (HA), which has a more unbalanced proportion of calcium to phosphate. Hydroxyapatite crystals make bones hard.
Because less soluble than brushite, hydroxyapatite cannibalizes brushite. The organic molecules in urine modify this process.
Calcium Phosphate stone formers
From Systemic diseases
Primary hyperparathyroidism and renal tubular acidosis raise average urine alkalinity (higher urine pH) and foster calcium phosphate kidney stones. Many uncommon genetic diseases do the same.
Idiopathic
Idiopathic calcium phosphate stone formers share a common set of traits. Perhaps because urine contains far more phosphate than oxalate, they form more frequent and larger stones than idiopathic calcium oxalate stone formers. Often the stones originate as crystal plugs at the terminal ends of the kidney tubules. More crystals deposit over the end of the plug open to the urine, to make the final stone. Crystal plugs damage the cells that line the tubules and cause local scarring.
Uric acid stones
Uric acid crystals
Structure and charged sites
A breakdown product of DNA and RNA, uric acid forms crystals in abnormally acidic (low pH) urine. Obese and diabetic people, those with gout or kidney disease typically produce abnormally acid urine. I know how the urine becomes acid, but leave it for elsewhere on the site.
Uric acid, the molecule we are interested in here (shown to the far right), has two linked rings made of carbon atoms (they are at the angles where lines join), with  interposed nitrogen (N), oxygen (O), and hydrogen (H) atoms.
interposed nitrogen (N), oxygen (O), and hydrogen (H) atoms.
This molecule has only two charged sites, the nitrogen atoms at the bottoms of the rings. In urine of pH 6 or so, one nitrogen lacks its hydrogen and therefore carries a single negative charge. In more alkaline solutions both nitrogens lack hydrogens, but urine does not normally achieve such alkalinity (pH>8).
When urine pH is low (<5.5) and both nitrogens have their hydrogens, the molecule lacks any charged site, so water can no longer find a hold on the molecule. It crystallizes. It simply leaves the water as water droplets themselves form from the high and vaporous late afternoon clouds and fall from the air as the warm rains of springtime.
Relation to water
Water molecules are each a single oxygen atom (large ball) bonded with two hydrogen atoms (small balls) as in this picture from Wikipedia. The hydrogen side has a positive, the bare side of the oxygen a negative charge. So water molecules link to each other, 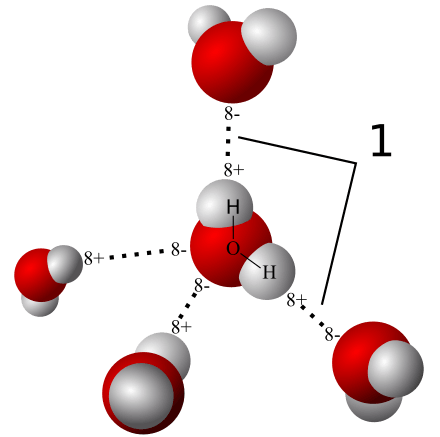 positives to negative surfaces, to make up the clear and seemingly continuous fluid we drink, swim in, and hold up umbrellas to keep off of us when it rains. They link by charge at angles, shown by the number ‘1’ so as to make up a three dimensional macrame.
positives to negative surfaces, to make up the clear and seemingly continuous fluid we drink, swim in, and hold up umbrellas to keep off of us when it rains. They link by charge at angles, shown by the number ‘1’ so as to make up a three dimensional macrame.
To be ‘in solution’ means to have some charge to which water molecules can link up with by attraction. Calcium atoms are positive and become surrounded by a shell of water molecules facing it with their bare negative surfaces. Oxalic and phosphoric acids have negative charges and are surrounded by water molecules pointing their positive or hydrogen sides to them.
Uric acid at neutral pH has its one negatively charged nitrogen water can grasp. But when pH falls, and neither nitrogen has any extra charge for water to bind with, how can the molecule remain among the water molecules? It cannot. The molecules stack into solid crystals and fall from solution.
Uric acid stone formers
The stones can be orange – red, large, and numerous
The stones can be red or orange because uric acid crystals absorb hemoglobin breakdown products that are red – orange pigments in urine. Sometimes uric acid crystals pass in urine as a red orange gravel.
Uric acid does not have to connect itself to some other atom or molecule to make a crystal, in the way that calcium must bond with oxalate or phosphate ions to make calcium oxalate or calcium phosphate crystals. When pH is low enough to extinguish its charge, uric acid can crystallize very fast, in seconds, and pass as an orange gravel in the urine. If retained, such crystals can grow rapidly into large stones. Because there is much more uric acid in urine than there is oxalic acid, uric acid stones can grow very large and rapidly. Some fill up the entire collecting system of the kidney.
Urine pH controls stone formation
But because the whole process depends almost completely on the acidity of the urine, uric acid stones are very easy to treat. Just a modest amount of supplemental alkali will make the urine of almost any patient alkaline enough that the hydrogen atoms are removed from the one crucial charged nitrogen. Water can bond there so uric acid remains in solution. Because so simple, treatment prevents stones with certainty. Relapse need never occur.
Mixed stones require special care
Unfortunately, however, stones commonly contain uric acid mixed with calcium oxalate. In this case, one needs to track down the cause of the calcium oxalate stones as well as make the urine alkaline enough to stop uric acid stones from forming. Calcium phosphate crystals mix with uric acid only rarely, because it takes a rather alkaline urine to remove the hydrogen atoms from phosphate so it has two negative charges and can bind efficiently with calcium atoms. At that higher pH, uric acid will have its charge site and remain in solution.
Struvite stones
Urea and the planet
Kidneys cannot make struvite. Bacteria make it. Not all bacteria, either. It takes bacteria that normally thrive in the soil, and they do it for ancient and compelling reasons. These bacteria produce the kidney stone named Struvite after Heinrich Christian Gottfried von Struve (1772–1851).
Animals deposit urea (at left) all over the planet when they urinate. Plants cannot use it.
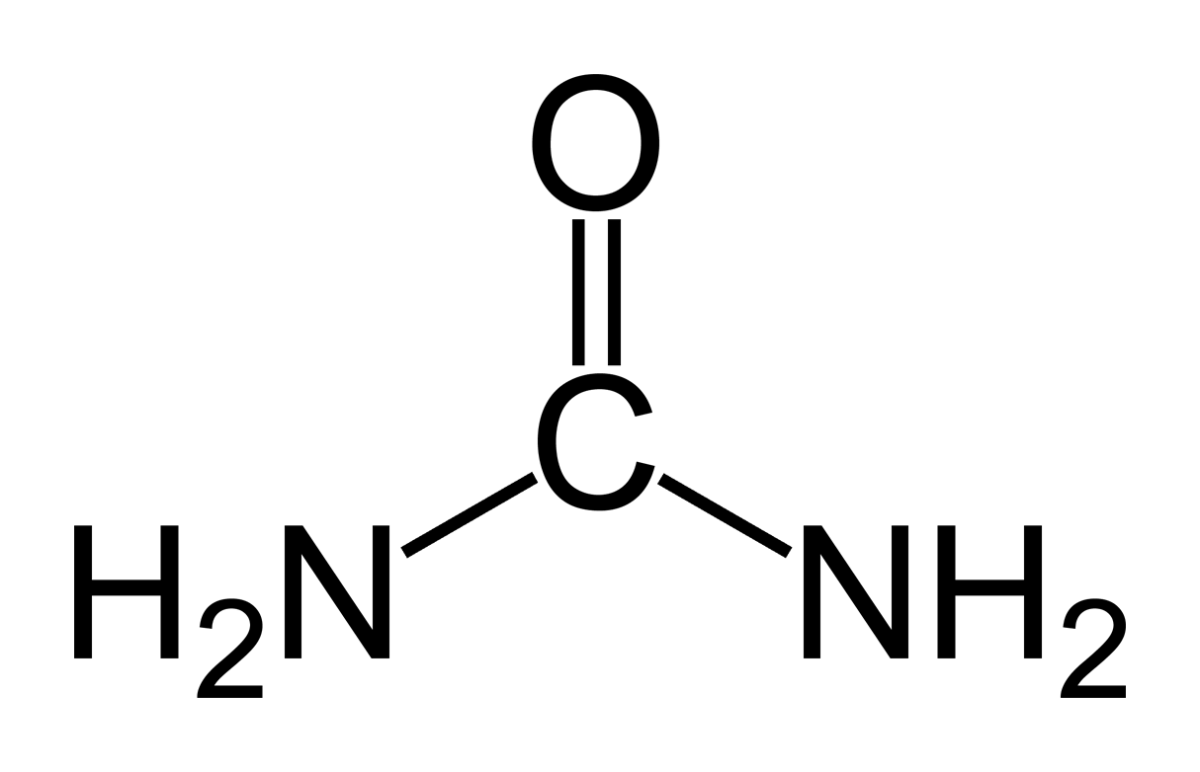 Like oxygen, nitrogen is an essential for life yet dangerous. It is integral to proteins, DNA and RNA. As these molecules are broken down and remade, some of their nitrogen slips by and can form poisonous compounds unless caught up in safe waste products. Of these, the main one, urea, contains 2 nitrogen atoms bound to a single carbon atom (‘C’ in the picture to your left).
Like oxygen, nitrogen is an essential for life yet dangerous. It is integral to proteins, DNA and RNA. As these molecules are broken down and remade, some of their nitrogen slips by and can form poisonous compounds unless caught up in safe waste products. Of these, the main one, urea, contains 2 nitrogen atoms bound to a single carbon atom (‘C’ in the picture to your left).
Uric acid contains 4 nitrogen atoms (look back at the picture of it). Birds and reptiles excrete most of their nitrogen as uric acid; mammals like us excrete nitrogen mainly as urea.
As the animals of the world urinate on the soil, their urea brings nitrogen to plant roots, but the plants cannot use it. They cannot release the nitrogens from the carbon atom that holds them. Those soil bacteria that make struvite crystals have an enzyme, called urease, that can release the nitrogen for plants to use as their nitrogen supply.
So, soil bacteria with urease maintain the nitrogen cycle of the earth.
Struvite crystals
As they release nitrogen from its carbon in urea, the nitrogen takes up a proton making ammonia (NH3). Ammonia is a powerful alkali and takes up another proton.
As it does so, the working bacteria surround themselves with spheres of very alkaline fluid enriched with ammonium ion (NH4) that carries one positive charge. Soil magnesium ( an atom with two positive charges) and phosphate sans all of its protons (an ion with three negative charges) spontaneously form their triple salt: three negative phosphate charges, two positive from magnesium, one positive from NH4).
The crystals anchor the bacteria and help create a porous nitrogen rich soul good for plants to grow in
The struvite kidney stone
Why they start
Because urine is filled with urea, soil bacteria that get into the urinary tract can break it down to ammonia and create struvite from the magnesium and phosphate urine always contains.
You might wonder how soil bacteria get into the urinary system.
Because we eat them, with foods that are not cooked, and they become part of the intestinal bacterial population from an early age. In us and around us, they find a way into the urinary system, especially in women whose shorter urethra makes entry easier. No matter how skillfully used, any instrument put into the bladder can carry our personal soil bacteria with it.
What they do
Because they live among molds and fungi, soil bacteria easily mount resistances to antibiotics, so antibiotics given for a urinary tract infection will tend to kill sensitive bacteria and select out those that can resist them.
Soil bacteria can produce struvite stones de novo, or infect calcium stones to produce a mixed stone. Either way, struvite stones are infected by their very nature. They can become huge. Their bacteria can injure the kidneys, even enter the bloodstream and cause sepsis.
Treatment is a mix of thoughtful surgery and selection of antibiotics after such surgery to kill bacteria that remain. If the stones are a mixture of struvite and calcium crystals, new calcium stones need to be prevented.
Cystine stones
Inherited kidney abnormality
 Lemon yellow with a sugary coating these form only in people who have an inherited kidney disorder called cystinuria.
Lemon yellow with a sugary coating these form only in people who have an inherited kidney disorder called cystinuria.
Although the kidneys function well, they permit abnormal amounts of four amino acids to enter the urine. Three do not matter that we know of. The fourth makes crystals and the cystine kidney stone type.
Cystine
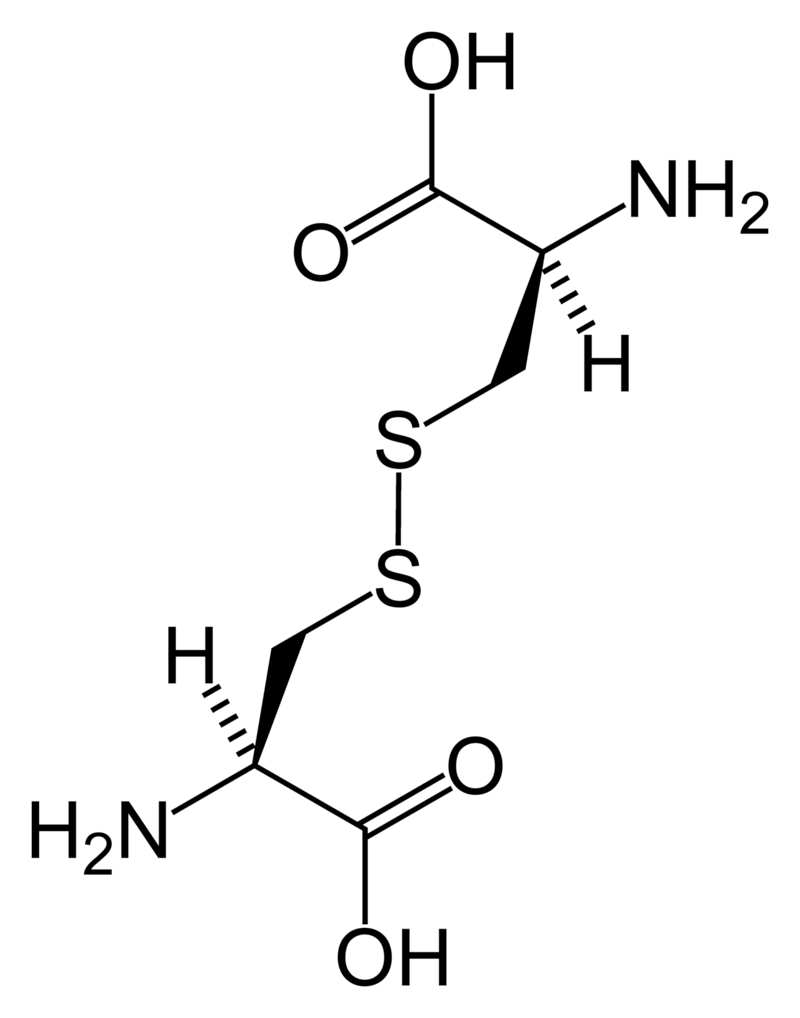
Cystine (left) forms through the coupling of two identical amino acids – called cysteine – through their sulfur atoms (‘S’ in the line drawing).
Each cysteine contains two carbon atoms – not shown except as corners – bonded together (shown by the single long line that connects the two corners) as in oxalic acid.
One carbon atom has 2 oxygens bonded to it; the other has one nitrogen (which makes it an amino – nitrogen containing – acid), a hydrogen atom, and a sulfur atom. As for phosphate, the dashed and solid arrows simply mean the hydrogens and sulfurs lie above and below the plane of the page and a stick model would have a three dimensional shape.
Cystine Crystals
Cysteine itself is very soluble because the sulfur atom has an appreciable negative charge.
But the big, long cystine molecule has very little charge because the sulfurs bind to each other. So, like uric acid, cystine loses intimacy with water molecules and simply leaves the solution as crystals. Also like uric acid, the process is fast.
Cystine stones
Because people with cystinuria lose large amounts of cystine in their urine stones readily grow large, and fast.
Stones probably form in the urine itself. But cystine crystals can plug the ends of kidney tubules, as calcium phosphate crystals do, causing cell damage.
Since cystinuria is an inherited disease, stones may begin in childhood.
Effective treatment always requires very large amounts of fluids to dilute the urine. The few effective drugs resemble cysteine. Their sulfur groups bond with cysteine to form a ‘mixed disulfide’ more soluble than cystine. But their side effects can limit use.
Rare stones
Here and there we find patients who make uncommon crystals and require very special care.
Uric acid, as an example, can form odd crystals such sodium or ammonium acid urate, especially in people with bowel disease and chronic diarrhea.
Anti-viral drugs can crystallize in urine and form stones only recognized for what they are through stone analysis.
Very rare disorders of metabolism can produce molecules which crystallize in the urine, for example 2-8 dihydroxyadenine.
Although it can take a while before the right answer emerges, stone analyses will put physicians on the right track for these special cases.
The end of a very long post
That’s my parade.
The common animals and the rarer animals have gone by, and you have glimpsed the main ones, big and small.
The one point is what it was at the beginning. Each kind of kidney stone has its own ways, and treatment requires we know which one you have.
Likewise, for whatever that one may be, it is good to know as much about it as you can know. For long term prevention of stones is hard to come by and ultimately what the patience and and consistency of patients themselves matters most.
If you don’t know which stones you have made, find out.
Track down old reports and pull them together.
Keep copies and send everything to the doctors who care for you.
Fred Coe MD
Recently i had a calcium oxalate stone 3*5 mm and the results of analysis was 85% monohydrate calcium oxalate and 15 dihydrate, after month i started to have pain again in both kidneys, honestly i am terrified and I don’t know what to do, medicine in my city is quite bad! And what kind of changes shall i do in my daily life?
Thanks a lot
Hi Ali, Here is my best on how to proceed toward treatment. I hope your city is not so bad as to preclude a proper evaluation. Regards, Fred Coe
Sorry I was diagnosed of kidney stone of size 6.9mm ,pls could it be pass or dissolve by drinking excess water pls? And if you got any tips I’m ready to listen
Hi Husain,
You cannot “dissolve” stones by drinking water. If the stone is on the move you can help flush it out quicker in many cases by drinking more fluid. But not dissolve it.
Best, Jill
Sorry I was diagnosed of kidney stone of size 6.9mm ,pls could it be pass or dissolve by drinking excess water pls? And if you got any tips I’m ready to listen
Hi Husain,
You cannot “dissolve” stones by drinking water. If the stone is on the move you can help flush it out quicker in many cases by drinking more fluid. But not dissolve it.
Best, Jill
What type might a darker , maybe about medium in color grey , jagged stone be. Felt this rushed of pain just with standing directly under perinium up into bladder after standing up after voiding which was a slower stream last night under periniem then about 24 hours later was sitting on toilet in the dark and felt a strange pain and interuption in my voiding stream so turned on the lights and saw a strange medium grey color spect in on toilet ledge so to speak was able to get fish it out of toilet and was a medium grey color jagged and pretty small. What are these color of stones related to usually. Thanks
Hi, Have the stone analyzed. Color is too unreliable and an exact analysis very valuable for your care. Regards, Fred Coe
What type might a darker , maybe about medium in color grey , jagged stone be. Felt this rushed of pain just with standing directly under perinium up into bladder after standing up after voiding which was a slower stream last night under periniem then about 24 hours later was sitting on toilet in the dark and felt a strange pain and interuption in my voiding stream so turned on the lights and saw a strange medium grey color spect in on toilet ledge so to speak was able to get fish it out of toilet and was a medium grey color jagged and pretty small. What are these color of stones related to usually. Thanks
Hi, Have the stone analyzed. Color is too unreliable and an exact analysis very valuable for your care. Regards, Fred Coe
Dear Dr. Coe,
I am a Norwegian male, 48 years old.
Since my first ever case of kidney stone started about 9 weeks ago I have visited your website many times to learn more about kidney stones, and find your information very useful. (I have also read countless other documents and sites on kidney stone and related issues to try to understand as much as I can, for weeks and weeks now.)
Within about 24 hours after initial renal colic symptoms (flank pain and nausea/vomiting) I woke up at night in a cold sweat and having violent shivers, and had a slight fever. The doctor I had seen the morning after the first symptoms had prescribed painkillers (Voltaren) and Tamsulosin to ease passing of kidney stone, and urged me to return if I were to get a fever. My wife and I therefore agreed to see a doctor that second morning. Before we were ready to go, things turned dramatically for the worse as my blood pressure must have very suddenly plunged – the following 30-40 minutes are completely erased from my memory, even though I did not pass out in the ususal sense, I even failed at an attempt to walk to the car while in this useless state, even though my wife had told me to wait for her to help me – and as things turned out I had a clear case of sepsis and was rushed to the hospital ECU in an ambulance, after having first received IV fluids and antibiotics.
At the ECU it was soon suspected that I had a hydronephrosis with a pyelonephrosis, which had led to urosepsis. A CT scan was soon made and immediately after that, a nephrostomy was found necessary to drain the kidney. Klebsiella bacteria were found in the pus from the kidney, and also in a blood culture. Proteus was also found in blood culture initially. I recovered nicely within a few days but remained hospitalized for a week while on antibiotics and with daily blood samples taken. The stone had been found to obstruct the right side ureter and measured about 8mm across, according to the study of CT images. Several urologists came to see me while at the hospital, one of them even thought it possible that the stone would pass down the ureter on its own, knowing its impossible size! I thought that was rather laughable, and as things turned out the stone had been lodged stuck the whole time until an URS laser lithotripsy procedure to remove the stone was performed about 5 weeks later, when the nephrostomy was also finally removed, Now, based on observations during the procedure and I suppose the presence of Klebsiella the urologists strongly suspected I had a case of infection stone. (What they specifically said was that they suspected dahllite stone). I was therefore anxious to learn about what would been found in stone analysis. One of the hospital doctors called me six days after the URS procedure and informed me that, based on analysis of stone fragments recovered during the procedure, indeed I had had a bacterial/infection stone. I asked for more details and only got this refered to verbally on the phone, but she told me the stone had been 60% carbonate apatite (Dahllite), and 40% calcium oxalate monohydrate. Based on this finding I was told to extend antibiotic treatment (Bactrim) for another two weeks, and that I would have to monitor my urin pH for an extended period of time to make sure it would not go alkaline (again), and if it were to go alkaline I should see my doctor and have him grow a culture on a urine sample, and to get antibiotic treatment according to known resistance patterns. Also that we would proceed to the previously outlined course of treatment: Another CT in three months, then another CT in a year’s time and then if necessary another URS to remove any remaining traces of kidney stone (a very small one having been observed already in early CT scans, in the other (left side) kidney), and with the ultimate objective of reestablishing a sterile kidney/urine environment. This clearly is the standard procedure in treating infection stones as far as I have gathered.
Now the thing that has now gotten me very puzzled and concerned, in the mean time having tried to educate myself on infection stones: Nine days after the initial call about the stone analysis, the superior at the hospital’s urology dept. sends me a letter stating that there was no infection stone, it was “just a normal calcium stone”, and that therefore (almost two weeks too late – he blames it on me – that he’d tried to call me, but I have NO missed calls from the hospital, as I have been extremely anxious to talk to these people!) he told me that only a week of antibiotics postoperative would be required, and that after a final CT scan in three months they would consider me done treated unless I were to receive notification otherwise. I called the hospital again asking them to leave him a message asking him to call me so that I could discuss this controversy. He called me yesterday, and we talked for a while, but I have to admit that conversation left me me no less puzzled. Among other things, he blamed some erratic voice recognition software for the written summary of the call that his female urology colleague had sent me along with the urine pH test kit, in which she had written – precisely as I had been told on the phone: “The stone analysis shows dahllite stone”. I had personally asked her to put this down in writing for me and to summarize what had been said during her call to me, including the instructions for the pH measurements. It was positively written by her at the keyboard and not by some voice recognition software. He then also said he had edited some of the documents previously written by her, but which were in agreement with his position at the time they were written. So what is going on here??? I have a hard time trusting this professional given the odd twists and turns and his fanciful excuses.
Her superior who I talked to yesterday also told me that it could not be an infection stone “because it was not a struvite stone”. I know I have read that infection stones can be carbonate apatite/dahllite AND/OR struvite, and it appears that stone analysis alone can not always necessarily determine for certain that the stone has been formed as a consequence of urease liberating bacteria. However, I also understand that Klebsiella and Proteus are among the bacteria often involved in cases of infection stones, and both were present in the infected urine and blood that gave me a life threatening case of sepsis which I certainly don’t want to experience one more time! I have also read that carbonate apatite stones can ONLY form in the presence of urease producing bacteria, but am not sure if this is considered an established fact? Out of curiosity I found a pH test strip at work the day before I got the first call from the hospital on the stone analysis, and measured a pH of 8. Some days later it was below 7.
Whatever the case may be, I have been on large amounts of antibiotics to deal with the Klebsiella infection during the past two months and under less fortunate circumstances it could have certainly claimed my life, had the sepsis had more time to progress before I got emergency treatment. I can not overstress how terrified I have been at the thought of what might have happened if, for instance I had been home alone when I had that plunge in blood pressure, mentally “not there”, unable to operate a phone to get help, losing hours of critical time before treatment…and the thought of possibly going through this again in another few years also does terrify me.
To me it is clear that these two urologists have come to different conclusions for some reason which I can not yet understand. I want to believe the female urologist who first called, simply because it makes more sense to me, based on what I have learned about infection stones on my own, and also as I know – from my experience, not yet in any medical records – that I appear to have had recurring mild cases of UTIs over the past decade and seem predisposed to urine infections because of what I have experienced as (occasional) bladder muscle functional irregularity, (occasional) pollakiuria, smelly urine at times etc. and since persons with recurring UTIs are at a higher risk of having kidney stones, I have read. I now of course realize I should have had these underlying conditions of mine sorted out and treated professionally by now, but following the kidney stone incident I have naturally become very interested in relevant urological issues and health. I therefore asked my doctor last week to be refered to an independent urologist locally, with whom I now have an appointment in four weeks. I will have to discuss the whole situation with him, of course. I do understand that there is some disagreement as to whether stone analysis can positively indicate infection stones, but can’t help but being confused when two presumably competent urologists come to such different conclusions, in particular when stone analysis seemed to clearly confirm their initial suspicions. In fact I also have to wonder if the latter (superior) urologist’s stance in this may be a “calculated risk” on the part of the hospital (and at my risk), in that ruling out infection stone, they will not be required to schedule another URS laser lithotripsy, which I understand is a quite costly procedure. Our healthcare system in Norway is such that the patient has no expenses associated with hospitalization or surgeries. However, the hospitals do have to worry about their expenses and surgical capacity because of their budgets and resources. The superior urologist told me to feel fortunate that I now will recognize the symptoms more easily if/when I have another kidney stone moving along, or another caseof sepsis. While that’s obviously a good thing, I would much rather feel assured that the risk of such a reoccurrence be minimized, at least based on what is known. Also because he does not know about my prior history of erratic bladder function and probable recurring UTIs (understood to be quite rare in males) I know I will definitely want an urologist to see a bigger picture on considering my kidney stone disease.
Since I could not possibly make this very brief and immediately suitable for publication I don’t know if you will want to use any of this on your website, but I would very much like to have your opinion as I have a very strong need to understand what has been going on in my body (and at the hospital!) and to feel reassured that I have been correctly diagnosed (if there is such a thing!)
I also think – whatever my case may be – that you should include further information about infection/struvite stones on your website, although I have a strong impression that these types of kidney stones are a tricky topic subject to no small amount of professional controversy. In fact the (university) hospital that treated me is curretly carrying out a research project on infection stones, and I consented to my stone samples being submitted to that project if found to be infection stones. At this point I do not really know what to make of the stone analysis anymore, but I do consider asking the lab to give it to me in writing so that at least I have all the details.
Meanwhile I hope you can spare a little of your time commenting on my situation.
Best Regards,
Thomas Dunker
Ski, Norway
Hi, Dahlite is a calcium phosphate crystal that includes considerable carbonate – the oxygens on carbonate become part of the calcium – oxygen lattice that produces the crystal – and forms preferentially at high urine pH values. Struvite is a crystal lattice of magnesium (2+) ammonium (-1) phosphate (-2), that requires an alkaline urine pH AND very high urine ammonium ion levels. Kidneys produce little ammonium ion when they produce an alkaline urine so struvite requires bacteria – urease as you noted + urea, abundant in urine. They hydrolyze urea to ammonia that promptly takes up a proton to make ammonium ion and raise local urine pH, and carbonate that forms calcium carbonate crystals at the high pH produced by urea hydrolysis. You have the right bacteria to produce struvite stones, but the wrong crystal. Stone analysis, however, is at its worst, at least in the US, when it comes to struvite. KIDNEY STONE ANALYSIS: How Bad is It? so the analysis may be wrong. One possibility is that you have a high urine pH as part of your biology and form calcium phosphate stones, received antibiotics for years, and colonized with the Gm- proteus and klebbsiela. Another is that your stone was struvite, the lab is wrong, and the bacteria are the main cause. I would ask the lab to recheck the scan (they would have used FTIR and the scan is still there, and can be compared to their library more carefully); some labs also have xray diffraction for odd cases -you are an odd case – which is exact. I would assume the worst, that the infection did it, make many ultra low dose CT studies – perhaps every 6 months for 2 years – to be sure to spot regrowth, and also do proper 24 hour urine studies that might disclose underlying causes of stones such as hypercalciuria. Any new stones should be removed promptly and re-studied to see if they are struvite or calcium phosphate, in the latter case you are very likely to have some non infectious stone cause ongoing and need treatment for it. Regards, Fred Coe
Dear Dr. Coe,
I am a Norwegian male, 48 years old.
Since my first ever case of kidney stone started about 9 weeks ago I have visited your website many times to learn more about kidney stones, and find your information very useful. (I have also read countless other documents and sites on kidney stone and related issues to try to understand as much as I can, for weeks and weeks now.)
Within about 24 hours after initial renal colic symptoms (flank pain and nausea/vomiting) I woke up at night in a cold sweat and having violent shivers, and had a slight fever. The doctor I had seen the morning after the first symptoms had prescribed painkillers (Voltaren) and Tamsulosin to ease passing of kidney stone, and urged me to return if I were to get a fever. My wife and I therefore agreed to see a doctor that second morning. Before we were ready to go, things turned dramatically for the worse as my blood pressure must have very suddenly plunged – the following 30-40 minutes are completely erased from my memory, even though I did not pass out in the ususal sense, I even failed at an attempt to walk to the car while in this useless state, even though my wife had told me to wait for her to help me – and as things turned out I had a clear case of sepsis and was rushed to the hospital ECU in an ambulance, after having first received IV fluids and antibiotics.
At the ECU it was soon suspected that I had a hydronephrosis with a pyelonephrosis, which had led to urosepsis. A CT scan was soon made and immediately after that, a nephrostomy was found necessary to drain the kidney. Klebsiella bacteria were found in the pus from the kidney, and also in a blood culture. Proteus was also found in blood culture initially. I recovered nicely within a few days but remained hospitalized for a week while on antibiotics and with daily blood samples taken. The stone had been found to obstruct the right side ureter and measured about 8mm across, according to the study of CT images. Several urologists came to see me while at the hospital, one of them even thought it possible that the stone would pass down the ureter on its own, knowing its impossible size! I thought that was rather laughable, and as things turned out the stone had been lodged stuck the whole time until an URS laser lithotripsy procedure to remove the stone was performed about 5 weeks later, when the nephrostomy was also finally removed, Now, based on observations during the procedure and I suppose the presence of Klebsiella the urologists strongly suspected I had a case of infection stone. (What they specifically said was that they suspected dahllite stone). I was therefore anxious to learn about what would been found in stone analysis. One of the hospital doctors called me six days after the URS procedure and informed me that, based on analysis of stone fragments recovered during the procedure, indeed I had had a bacterial/infection stone. I asked for more details and only got this refered to verbally on the phone, but she told me the stone had been 60% carbonate apatite (Dahllite), and 40% calcium oxalate monohydrate. Based on this finding I was told to extend antibiotic treatment (Bactrim) for another two weeks, and that I would have to monitor my urin pH for an extended period of time to make sure it would not go alkaline (again), and if it were to go alkaline I should see my doctor and have him grow a culture on a urine sample, and to get antibiotic treatment according to known resistance patterns. Also that we would proceed to the previously outlined course of treatment: Another CT in three months, then another CT in a year’s time and then if necessary another URS to remove any remaining traces of kidney stone (a very small one having been observed already in early CT scans, in the other (left side) kidney), and with the ultimate objective of reestablishing a sterile kidney/urine environment. This clearly is the standard procedure in treating infection stones as far as I have gathered.
Now the thing that has now gotten me very puzzled and concerned, in the mean time having tried to educate myself on infection stones: Nine days after the initial call about the stone analysis, the superior at the hospital’s urology dept. sends me a letter stating that there was no infection stone, it was “just a normal calcium stone”, and that therefore (almost two weeks too late – he blames it on me – that he’d tried to call me, but I have NO missed calls from the hospital, as I have been extremely anxious to talk to these people!) he told me that only a week of antibiotics postoperative would be required, and that after a final CT scan in three months they would consider me done treated unless I were to receive notification otherwise. I called the hospital again asking them to leave him a message asking him to call me so that I could discuss this controversy. He called me yesterday, and we talked for a while, but I have to admit that conversation left me me no less puzzled. Among other things, he blamed some erratic voice recognition software for the written summary of the call that his female urology colleague had sent me along with the urine pH test kit, in which she had written – precisely as I had been told on the phone: “The stone analysis shows dahllite stone”. I had personally asked her to put this down in writing for me and to summarize what had been said during her call to me, including the instructions for the pH measurements. It was positively written by her at the keyboard and not by some voice recognition software. He then also said he had edited some of the documents previously written by her, but which were in agreement with his position at the time they were written. So what is going on here??? I have a hard time trusting this professional given the odd twists and turns and his fanciful excuses.
Her superior who I talked to yesterday also told me that it could not be an infection stone “because it was not a struvite stone”. I know I have read that infection stones can be carbonate apatite/dahllite AND/OR struvite, and it appears that stone analysis alone can not always necessarily determine for certain that the stone has been formed as a consequence of urease liberating bacteria. However, I also understand that Klebsiella and Proteus are among the bacteria often involved in cases of infection stones, and both were present in the infected urine and blood that gave me a life threatening case of sepsis which I certainly don’t want to experience one more time! I have also read that carbonate apatite stones can ONLY form in the presence of urease producing bacteria, but am not sure if this is considered an established fact? Out of curiosity I found a pH test strip at work the day before I got the first call from the hospital on the stone analysis, and measured a pH of 8. Some days later it was below 7.
Whatever the case may be, I have been on large amounts of antibiotics to deal with the Klebsiella infection during the past two months and under less fortunate circumstances it could have certainly claimed my life, had the sepsis had more time to progress before I got emergency treatment. I can not overstress how terrified I have been at the thought of what might have happened if, for instance I had been home alone when I had that plunge in blood pressure, mentally “not there”, unable to operate a phone to get help, losing hours of critical time before treatment…and the thought of possibly going through this again in another few years also does terrify me.
To me it is clear that these two urologists have come to different conclusions for some reason which I can not yet understand. I want to believe the female urologist who first called, simply because it makes more sense to me, based on what I have learned about infection stones on my own, and also as I know – from my experience, not yet in any medical records – that I appear to have had recurring mild cases of UTIs over the past decade and seem predisposed to urine infections because of what I have experienced as (occasional) bladder muscle functional irregularity, (occasional) pollakiuria, smelly urine at times etc. and since persons with recurring UTIs are at a higher risk of having kidney stones, I have read. I now of course realize I should have had these underlying conditions of mine sorted out and treated professionally by now, but following the kidney stone incident I have naturally become very interested in relevant urological issues and health. I therefore asked my doctor last week to be refered to an independent urologist locally, with whom I now have an appointment in four weeks. I will have to discuss the whole situation with him, of course. I do understand that there is some disagreement as to whether stone analysis can positively indicate infection stones, but can’t help but being confused when two presumably competent urologists come to such different conclusions, in particular when stone analysis seemed to clearly confirm their initial suspicions. In fact I also have to wonder if the latter (superior) urologist’s stance in this may be a “calculated risk” on the part of the hospital (and at my risk), in that ruling out infection stone, they will not be required to schedule another URS laser lithotripsy, which I understand is a quite costly procedure. Our healthcare system in Norway is such that the patient has no expenses associated with hospitalization or surgeries. However, the hospitals do have to worry about their expenses and surgical capacity because of their budgets and resources. The superior urologist told me to feel fortunate that I now will recognize the symptoms more easily if/when I have another kidney stone moving along, or another caseof sepsis. While that’s obviously a good thing, I would much rather feel assured that the risk of such a reoccurrence be minimized, at least based on what is known. Also because he does not know about my prior history of erratic bladder function and probable recurring UTIs (understood to be quite rare in males) I know I will definitely want an urologist to see a bigger picture on considering my kidney stone disease.
Since I could not possibly make this very brief and immediately suitable for publication I don’t know if you will want to use any of this on your website, but I would very much like to have your opinion as I have a very strong need to understand what has been going on in my body (and at the hospital!) and to feel reassured that I have been correctly diagnosed (if there is such a thing!)
I also think – whatever my case may be – that you should include further information about infection/struvite stones on your website, although I have a strong impression that these types of kidney stones are a tricky topic subject to no small amount of professional controversy. In fact the (university) hospital that treated me is curretly carrying out a research project on infection stones, and I consented to my stone samples being submitted to that project if found to be infection stones. At this point I do not really know what to make of the stone analysis anymore, but I do consider asking the lab to give it to me in writing so that at least I have all the details.
Meanwhile I hope you can spare a little of your time commenting on my situation.
Best Regards,
Thomas Dunker
Ski, Norway
Hi, Dahlite is a calcium phosphate crystal that includes considerable carbonate – the oxygens on carbonate become part of the calcium – oxygen lattice that produces the crystal – and forms preferentially at high urine pH values. Struvite is a crystal lattice of magnesium (2+) ammonium (-1) phosphate (-2), that requires an alkaline urine pH AND very high urine ammonium ion levels. Kidneys produce little ammonium ion when they produce an alkaline urine so struvite requires bacteria – urease as you noted + urea, abundant in urine. They hydrolyze urea to ammonia that promptly takes up a proton to make ammonium ion and raise local urine pH, and carbonate that forms calcium carbonate crystals at the high pH produced by urea hydrolysis. You have the right bacteria to produce struvite stones, but the wrong crystal. Stone analysis, however, is at its worst, at least in the US, when it comes to struvite. KIDNEY STONE ANALYSIS: How Bad is It? so the analysis may be wrong. One possibility is that you have a high urine pH as part of your biology and form calcium phosphate stones, received antibiotics for years, and colonized with the Gm- proteus and klebbsiela. Another is that your stone was struvite, the lab is wrong, and the bacteria are the main cause. I would ask the lab to recheck the scan (they would have used FTIR and the scan is still there, and can be compared to their library more carefully); some labs also have xray diffraction for odd cases -you are an odd case – which is exact. I would assume the worst, that the infection did it, make many ultra low dose CT studies – perhaps every 6 months for 2 years – to be sure to spot regrowth, and also do proper 24 hour urine studies that might disclose underlying causes of stones such as hypercalciuria. Any new stones should be removed promptly and re-studied to see if they are struvite or calcium phosphate, in the latter case you are very likely to have some non infectious stone cause ongoing and need treatment for it. Regards, Fred Coe
HI,
Can you tell by the composition of my stone (below)
whether it was caused by oxalates or red meat consumption ?
Also do you know how quickly a stone this size can form ?
Thanks much !
9x15mm stone
Calculus Composition
50% Calcium Oxalate Dihydrate
40% Calcium Oxalate Monohydrate
10% Minor Components
Hi Steven,
Ask your doc to order you a 24 hour urine collection. This way you can find out why you are forming stones.
jill
HI,
Can you tell by the composition of my stone (below)
whether it was caused by oxalates or red meat consumption ?
Also do you know how quickly a stone this size can form ?
Thanks much !
9x15mm stone
Calculus Composition
50% Calcium Oxalate Dihydrate
40% Calcium Oxalate Monohydrate
10% Minor Components
Hi Steven,
Ask your doc to order you a 24 hour urine collection. This way you can find out why you are forming stones.
jill
Recent CT imaging for other reasons revealed a “small non-obstructive kidney stone”. My mother suffered from kidney stones but in her case the long term treatment was limiting intake of red meat and red wine. Since I already have limited intake of purines the stone is likely something else. My GP said there were two types, uric and calcium. From your article it is clearly more complex. I do not care to ignore the potential problem even though advised that the stone is small and non-obstructive. Obviously “drink more water” is a start, and I probably need to measure urine pH. It is clear to me that I must drive the investigation. What would be your initial testing suggestions to determine stone chemistry?
Recent CT imaging for other reasons revealed a “small non-obstructive kidney stone”. My mother suffered from kidney stones but in her case the long term treatment was limiting intake of red meat and red wine. Since I already have limited intake of purines the stone is likely something else. My GP said there were two types, uric and calcium. From your article it is clearly more complex. I do not care to ignore the potential problem even though advised that the stone is small and non-obstructive. Obviously “drink more water” is a start, and I probably need to measure urine pH. It is clear to me that I must drive the investigation. What would be your initial testing suggestions to determine stone chemistry?
Hi Peter, A wise note, and here is my best on how to begin. See if it works for you. Regards, Fred Coe
Good day, i just received test results of ny kiddny stine that states” Calcium Oxalate Dihydrate (Weddellite) 20% Calcium Oxalate Monohydrate (Whewellite) 80%”. Can you give me any info in what this means and how to prevent?
Hi Cornelius, That is a common kind of stone. Here is a good starting place you might find useful in planning your next steps. Regards, Fred Coe
Good day, i just received test results of ny kiddny stine that states” Calcium Oxalate Dihydrate (Weddellite) 20% Calcium Oxalate Monohydrate (Whewellite) 80%”. Can you give me any info in what this means and how to prevent?
Hi Cornelius, That is a common kind of stone. Here is a good starting place you might find useful in planning your next steps. Regards, Fred Coe
My ultrasound report dated November 11, 2020 states the following: Left kidney measures 10.3 cm and demonstrates non-obstructing upper pole 0.4 cm and non-obstructing interpolar 0.2 cm alculi.
Before the US, I passed a 0.3 cm stone which I took to the lab and the report came back that it is calcium oxalate monohydrate.
I need some opinion related to drinking tap water (which according to local authorities here in Ontario Canada, it is safe and healthy to drink) but I wanted to get your opinion if I need to drink bottled or filtered water instead of tap water.
Also are there recommendations for treatment or natural products to dissolve the kidney stones shown on my UltraSound report?
Thank you.
Hi Sherif, calcium oxalate stones will not dissolve in human kidneys. Urban tap water is not a cause of stones, so drink it liberally. As for prevention, here is my best introduction. Regards, Fred Coe
My ultrasound report dated November 11, 2020 states the following: Left kidney measures 10.3 cm and demonstrates non-obstructing upper pole 0.4 cm and non-obstructing interpolar 0.2 cm alculi.
Before the US, I passed a 0.3 cm stone which I took to the lab and the report came back that it is calcium oxalate monohydrate.
I need some opinion related to drinking tap water (which according to local authorities here in Ontario Canada, it is safe and healthy to drink) but I wanted to get your opinion if I need to drink bottled or filtered water instead of tap water.
Also are there recommendations for treatment or natural products to dissolve the kidney stones shown on my UltraSound report?
Thank you.
Hi Sherif, calcium oxalate stones will not dissolve in human kidneys. Urban tap water is not a cause of stones, so drink it liberally. As for prevention, here is my best introduction. Regards, Fred Coe
I had a 6 cmx3 cm staghorn stone removed last year. Since then, I’ve had a lithotripsy three times. My stones are Calcium Phosphate (60% brushite and 30% apatite) and 10% Oxalate. My stones grow quickly and large and I can keep them at bay by drinking 3 liters of water a day. I went a week without meeting my daily 3 liter goal due to nausea and now I fear I’ll be headed for another lithotripsy. What is the underlying cause of this rapid stone growth and how do I prevent it from happening in the first place?
I have met with an endocrinologist for initial testing and he has told me to stop taking vitamin d and calcium supplements despite a deficiency. My urology office seems content with keeping the issue under control by drinking 3 liters of water daily.
Hi L. J. Brushite stones are a very special kind of problem, and respond poorly to shock wave lithotripsy. They grow rapidly and need skilled care. This article is about calcium phosphate stones in general. In general urine calcium is high because of genetic hypercalciuria, and treatment is not lower diet calcium – vitamin D supplements have no risk at all unless serum 25D levels become abnormally high. Urine is often alkaline for reasons still in research, and cannot be lowered. If your personal physicians are not completely comfortable with brushite stone management, they may want to secure a second opinion for you from a place geographically near to you. Regards, Fred Coe
I had a 6 cmx3 cm staghorn stone removed last year. Since then, I’ve had a lithotripsy three times. My stones are Calcium Phosphate (60% brushite and 30% apatite) and 10% Oxalate. My stones grow quickly and large and I can keep them at bay by drinking 3 liters of water a day. I went a week without meeting my daily 3 liter goal due to nausea and now I fear I’ll be headed for another lithotripsy. What is the underlying cause of this rapid stone growth and how do I prevent it from happening in the first place?
I have met with an endocrinologist for initial testing and he has told me to stop taking vitamin d and calcium supplements despite a deficiency. My urology office seems content with keeping the issue under control by drinking 3 liters of water daily.
Hi L. J. Brushite stones are a very special kind of problem, and respond poorly to shock wave lithotripsy. They grow rapidly and need skilled care. This article is about calcium phosphate stones in general. In general urine calcium is high because of genetic hypercalciuria, and treatment is not lower diet calcium – vitamin D supplements have no risk at all unless serum 25D levels become abnormally high. Urine is often alkaline for reasons still in research, and cannot be lowered. If your personal physicians are not completely comfortable with brushite stone management, they may want to secure a second opinion for you from a place geographically near to you. Regards, Fred Coe
Is it possible to grow & pass two types of kidney stones? I started passing stones @ age 25 (calcium oxalate). Starting 3 years ago I started passing stones& chronic sand to the point now that it is constant. In June my stone tested as 100% phosphate & Randall’s Plaques was found in my right kidney which is the non stop kidney problem. Left is fine. I was put on K-Phos to add acid back to my PH, which was over 7. Ihave been diligent on low oxalate diet & water intake. I could really use some ideas on how to treat this and make it stop!
Hi Gina, Phosphate stones are due to a higher urine pH, oxalate is not relevant – they have none. I imagine your urine calcium is above normal, if so you need to lower it. Here is a good article on the phosphate kind of stones. Be sure the urine ammonia is not real high; it should be below your urine sulfate, or at most just a bit higher. A lot higher would mean infection. Regards, Fred Coe
Is it possible to grow & pass two types of kidney stones? I started passing stones @ age 25 (calcium oxalate). Starting 3 years ago I started passing stones& chronic sand to the point now that it is constant. In June my stone tested as 100% phosphate & Randall’s Plaques was found in my right kidney which is the non stop kidney problem. Left is fine. I was put on K-Phos to add acid back to my PH, which was over 7. Ihave been diligent on low oxalate diet & water intake. I could really use some ideas on how to treat this and make it stop!
Hi Gina, Phosphate stones are due to a higher urine pH, oxalate is not relevant – they have none. I imagine your urine calcium is above normal, if so you need to lower it. Here is a good article on the phosphate kind of stones. Be sure the urine ammonia is not real high; it should be below your urine sulfate, or at most just a bit higher. A lot higher would mean infection. Regards, Fred Coe
My stone analysis says it is 60% calcium oxalate and 40% hydroxyapatite. Seems to be a combination of two types of stones? Can you shed some light for me? Thanks.
Hi AB, I can. You form calcium oxalate stones with a lot of phosphate in them. This article speaks about why and also treatment. This article covers treatment in more depth and alludes to the fact that calcium phosphate stone treatment is not very different. Regards, Fred Coe
My stone analysis says it is 60% calcium oxalate and 40% hydroxyapatite. Seems to be a combination of two types of stones? Can you shed some light for me? Thanks.
Hi AB, I can. You form calcium oxalate stones with a lot of phosphate in them. This article speaks about why and also treatment. This article covers treatment in more depth and alludes to the fact that calcium phosphate stone treatment is not very different. Regards, Fred Coe
I found out I have multiple “punctate” stones in both kidney’s via a CT scan of my abdomen in the beginning of Oct 2020. There was no mention as to size or what they are “made of” on the report. My oncologist hasn’t even mentioned the presence of them to me which I find disturbing. I take two medications that I suspect could be the cause (Boniva -for osteoporosis and QDexy-for migraines) as the last CT 18 months ago had no mention of any stones in either kidney and both medications have stones as a possible side effect. Other than stopping these medications do you have any suggestions for treating them?
Hi Dayna, “Qudexy XR (topiramate) Extended-Release Capsules | Patients” – you are very astute. Topiramate is a prime stone producing drug, we know how it does this, enough to know the stones will be calcium phosphate, and enough to say you need to stop if right away and have your physicians find you an alternative medication. Boniva has no role in stones. Regards, Fred Coe
Very, very interesting. I’ve just undergone a lengthy lithotripsy surgery on L and R after the placements of stents the week before, due to blockage. The majority of my “numerous” stones being > 7mm. My lab results say 40% Calcium Oxalate Monohydrate/60% CA Oxalate Dihydrate. I’m trying to absorb all the information your articles gives us, which I find fascinating, but have trouble understanding with my layman mind. I will continue to read your offerings, and use my new best friend, Google, to help me understand why my body has decided on this painful retaliation. I believe we are all in appreciation of your information.
Hi Nita B, Calcium oxalate stones are the common ones, and this article speaks directly to your situation. Take a look and assure you get evaluated and treated as in the article – it is very accurate. Regards, Fred Coe
Very, very interesting. I’ve just undergone a lengthy lithotripsy surgery on L and R after the placements of stents the week before, due to blockage. The majority of my “numerous” stones being > 7mm. My lab results say 40% Calcium Oxalate Monohydrate/60% CA Oxalate Dihydrate. I’m trying to absorb all the information your articles gives us, which I find fascinating, but have trouble understanding with my layman mind. I will continue to read your offerings, and use my new best friend, Google, to help me understand why my body has decided on this painful retaliation. I believe we are all in appreciation of your information.
Hi Nita B, Calcium oxalate stones are the common ones, and this article speaks directly to your situation. Take a look and assure you get evaluated and treated as in the article – it is very accurate. Regards, Fred Coe
How long does it take from a given meal to change the urine PH? Let’s say you eat lunch and you add a good amount of fruits and vegetables, how many hours would it take for your urine PH to rise for someone with uric acid stones?
Hi Geo, The increase is from absorption of food anion that is metabolized to bicarbonate, so pH rises over a few hours. But uric acid stone formers have a peculiarly low urine pH and I guess the food response is very small at best. If you have such stones potassium citrate or another alkali like sodium citrate or bicarbonate is really right and nothing else as reliable. Regards, Fred Coe
How long does it take from a given meal to change the urine PH? Let’s say you eat lunch and you add a good amount of fruits and vegetables, how many hours would it take for your urine PH to rise for someone with uric acid stones?
Hi Geo, The increase is from absorption of food anion that is metabolized to bicarbonate, so pH rises over a few hours. But uric acid stone formers have a peculiarly low urine pH and I guess the food response is very small at best. If you have such stones potassium citrate or another alkali like sodium citrate or bicarbonate is really right and nothing else as reliable. Regards, Fred Coe
Good
Good
Thanks for the article. I have had two occurrences of calcium phosphate stones. It was quite traumatic each time, being only in my early 20’s. I’m wondering if I should limit the amount of oxalates in my diet as well? Do oxalates have an effect on calcium phosphate stones? Thanks.
Hi Allison, Phosphate stones usually contain only a little – or even no – oxalate so oxalate is beside the point. Here is an article on phosphate stone formers. Here is my best one on how to get a full evaluation and plan prevention. Regards, Fred Coe
Thanks for the article. I have had two occurrences of calcium phosphate stones. It was quite traumatic each time, being only in my early 20’s. I’m wondering if I should limit the amount of oxalates in my diet as well? Do oxalates have an effect on calcium phosphate stones? Thanks.
Hi Allison, Phosphate stones usually contain only a little – or even no – oxalate so oxalate is beside the point. Here is an article on phosphate stone formers. Here is my best one on how to get a full evaluation and plan prevention. Regards, Fred Coe
8/11 I had gross hematuria and severe abdominal pain on my lower left abdomen. The couldn’t find stones on my ct and the pain never left, and the bleeding stopped. I assumed that this a false diagnosis until a couple of days ago when the pain in the same place spiked from 6-10 and I immediately started urinating blood. This time they found a kidney stone in my left and right kidney tubes. When this started in 8/11 my border line anemia became more severe with my ferritin being 6 and iron 36. Is it possible to develop kidney stones from iron, and that I may have some rare condition where my kidneys filter iron out from my blood. I had a battery of tests from cystoscopies CT scans and MRI’s. I even had a colonoscopy and endoscopy which didn’t show any area of internal bleeding. The weird thing is that the pain is never in my back just in m lower left abdomen that doesn’t go away after passing the stone and intensity’s when hematuria starts.
Hi Michael, Complex. I would focus on the stone part by getting a full evaluation. Urine iron loss is not likely and iron stones not heard of. Some of your pain and bleeding can be coming from crystalluria, not seen unless sought for. The stone removed – be sure to get it analyzed! As for the anemia, I cannot help. Regards, Fred Coe
8/11 I had gross hematuria and severe abdominal pain on my lower left abdomen. The couldn’t find stones on my ct and the pain never left, and the bleeding stopped. I assumed that this a false diagnosis until a couple of days ago when the pain in the same place spiked from 6-10 and I immediately started urinating blood. This time they found a kidney stone in my left and right kidney tubes. When this started in 8/11 my border line anemia became more severe with my ferritin being 6 and iron 36. Is it possible to develop kidney stones from iron, and that I may have some rare condition where my kidneys filter iron out from my blood. I had a battery of tests from cystoscopies CT scans and MRI’s. I even had a colonoscopy and endoscopy which didn’t show any area of internal bleeding. The weird thing is that the pain is never in my back just in m lower left abdomen that doesn’t go away after passing the stone and intensity’s when hematuria starts.
Hi Michael, Complex. I would focus on the stone part by getting a full evaluation. Urine iron loss is not likely and iron stones not heard of. Some of your pain and bleeding can be coming from crystalluria, not seen unless sought for. The stone removed – be sure to get it analyzed! As for the anemia, I cannot help. Regards, Fred Coe
I had a bladder stone jagged and porous when I took a long road trip and could not use the bathroom for several hours. I also was not drinking enough water during that time (had been drinking iced tea caffeinated). Well a day later I thought I had come down with a bladder infection and after taking cranberry juice and seeing no improvement, I felt it was odd that I felt the most pain in the evening and none in the morning. Rare for a UTI. Also have to mention I have prolapse. So it makes it harder to pee. Anyway, I peed a few days later and a painless jagged porous stone came out not very large and the pain was then gone. I hope this helps people. Been drinking water instead and please by all means pee if you have to go! Do NOT hold it. May God truly bless your day!
Hi Anonymous, Given your symptoms the stone may have been lodged at the junction of the ureter and bladder. Regards, Fred Coe
I’ve had kidney stones periodically since my 20s despite being a voracious water drinker, I’m now 65. My Dad had them too. Of interest is we both have double collection systems. I have Ehlers-Danlos with Intestinal malabsorption. I had to have part of my stomach and small intestine removed 3 years ago. I started an even stricter elimination diet before that to reduce inflammation.
But in the last 2 years I’ve had 6 oxalate stones, passing only 2,despite being on a 30mg day diet. My weight was so low, I had a PEG tube. At least I could hydrate better (miss guzzling water). The tube is out, but these stones are wearing me down.
Hello Dr, I would presume that high urine oxalate has played a role given malabsorption and small bowel resection. In addition to fluids and diet, if urine oxalate is high one might consider ways to lower it such as calcium supplements or even cholestyramine. Because I do not know your 24 hour urine results I am hesitant to say anything more. Best, Fred
I’ve had kidney stones periodically since my 20s despite being a voracious water drinker, I’m now 65. My Dad had them too. Of interest is we both have double collection systems. I have Ehlers-Danlos with Intestinal malabsorption. I had to have part of my stomach and small intestine removed 3 years ago. I started an even stricter elimination diet before that to reduce inflammation.
But in the last 2 years I’ve had 6 oxalate stones, passing only 2,despite being on a 30mg day diet. My weight was so low, I had a PEG tube. At least I could hydrate better (miss guzzling water). The tube is out, but these stones are wearing me down.
Hello Dr, I would presume that high urine oxalate has played a role given malabsorption and small bowel resection. In addition to fluids and diet, if urine oxalate is high one might consider ways to lower it such as calcium supplements or even cholestyramine. Because I do not know your 24 hour urine results I am hesitant to say anything more. Best, Fred
Hello, two years ago I had surgery to remove a 9mm 60 percent calicum oxalate , 40 percent calcium phosphate stone. Since then 6 more tiny stones were seen on a cat scan. That was about a year ago . My Urologist just had me have an Xray, nothing remarkable showed there. I have a a Ultrasound orderd for my appointment in Sept. Does this sound like a good plan in general ? The first stone passed all the way down and was sitting on top the bladder. The Drs. Were amazed that I was able to take the pain that long . Told them many times I live with chronic flank pain. We just can’t figure it out yet. Thanks for any thoughts. Great article , I appreciate it.
Hi Lisa, You are behaving more like a calcium phosphate than a calcium oxalate stone former. Routine xrays and US do not show the many crystal deposits seen on your prior CT, because CT is far more sensitive. CT are now so low in radiation one can use them to follow the course of new stones, and should. Prevention of your kind of stone is in the article I linked to at the top of this response. Here is a more general prevention article, as well. Regards, Fred Coe
Hello, two years ago I had surgery to remove a 9mm 60 percent calicum oxalate , 40 percent calcium phosphate stone. Since then 6 more tiny stones were seen on a cat scan. That was about a year ago . My Urologist just had me have an Xray, nothing remarkable showed there. I have a a Ultrasound orderd for my appointment in Sept. Does this sound like a good plan in general ? The first stone passed all the way down and was sitting on top the bladder. The Drs. Were amazed that I was able to take the pain that long . Told them many times I live with chronic flank pain. We just can’t figure it out yet. Thanks for any thoughts. Great article , I appreciate it.
Hi Lisa, You are behaving more like a calcium phosphate than a calcium oxalate stone former. Routine xrays and US do not show the many crystal deposits seen on your prior CT, because CT is far more sensitive. CT are now so low in radiation one can use them to follow the course of new stones, and should. Prevention of your kind of stone is in the article I linked to at the top of this response. Here is a more general prevention article, as well. Regards, Fred Coe
As a chemical engineer with issues in my left kidney, I appreciate this post very much. Thank you!
As a chemical engineer with issues in my left kidney, I appreciate this post very much. Thank you!
I have a long history of stones, I’m 58 years old and the first one I remember I was 16. I don’t remember passing it but I remember the pain. Next one I was 20 before joining the Army, and I don’t have any memories of any pain. I was a Bulldozer operator in civilian life and I started throwing Stones every three months. I changed professions 19 years ago and they slowed down but got larger. I have had over 60 stones and have passed all but two on my own. My stones have most always been CAOX but have had a few Uric Acid stones for some reason. I had success with dissolving one from 9mm to 5mm before it broke into 4 pieces. I have been told that I need to become a vegetarian. I have given it some thought but I still eat meat. So as I read some of the comments I relate to a lot of what’s being said. Good luck and God Bless…
Hi Tim, The uric acid part of your stones is easily prevented. The calcium oxalate part – if those mechanisms are still working – likewise. One need not be vegetarian to be stone free. Regards, Fred Coe
I have a long history of stones, I’m 58 years old and the first one I remember I was 16. I don’t remember passing it but I remember the pain. Next one I was 20 before joining the Army, and I don’t have any memories of any pain. I was a Bulldozer operator in civilian life and I started throwing Stones every three months. I changed professions 19 years ago and they slowed down but got larger. I have had over 60 stones and have passed all but two on my own. My stones have most always been CAOX but have had a few Uric Acid stones for some reason. I had success with dissolving one from 9mm to 5mm before it broke into 4 pieces. I have been told that I need to become a vegetarian. I have given it some thought but I still eat meat. So as I read some of the comments I relate to a lot of what’s being said. Good luck and God Bless…
Hi Tim, The uric acid part of your stones is easily prevented. The calcium oxalate part – if those mechanisms are still working – likewise. One need not be vegetarian to be stone free. Regards, Fred Coe
I have had pain in my right side for years. I have many stones in both kidneys. The ones on the right side are in the “upper pole” of the kidney, at least 4.5 mm. There are at least 7 on the right side, 9 on the left. I have had lithotripsy and surgery to have them removed by basket on both sides. That was 2017. My Urologist talks me it isn’t possible to have pain if they aren’t lodged in the urethra. I’ve had so many imaging tests and nothing else is wrong.
Hi Laura, Vast numbers of people have non obstructing stones with severe pain. It is a contemporary research issue. Infection is always a possibility. Whether surgery helps is unknown. Sometimes pain is episodic, and that can be crystal passage, and fixable. Regards, Fred Coe
I’ve had kidney stones for most of my life, starting when I was 16, I’m 38 now, I’ve had 3 stones analyzed in the past 5 years, all having different makeups. The most recent one was 40% calcium phosphate, 30% calcium oxalate monohydrate, 30% calcium oxalate dihydrate. I haven’t found a physician that will work on prevention, mostly because they want to get rid of them before we get into prevention treatment and we can’t get rid of them. So I’m continually researching for myself and I never seem to find solid recommendations. What should I avoid? What do I need more of (besides water, I crave flavor and am also hypoglycemic so I can’t do anything with artificial sweeteners)?
I’ll add I am magnesium, vitamin D, and B-12 deficient, borderline hypothyroidism. My urine almost always has a high PH and frequent bacterial infections. My sodium levels in my blood are good. I’m just tired of constantly being in pain.
Hi Elizabeth, Stones since 16, high urine pH, I would guess you have genetic hypercalciuria, but that is just a guess. You need comprehensive testing to figure out if this is the cause, or something else. Here is my usual suggestions for evaluation. Your hypoglycemia may be due to abnormal insulin response to sugar, and worsened by sugar intake – rebound hypoglycemia. That can raise urine calcium in bursts after each sugar load. I am quite certain your stone production can be much lowered, but do not have enough details to say more. Regards, Fred Coe
I’ve had kidney stones for most of my life, starting when I was 16, I’m 38 now, I’ve had 3 stones analyzed in the past 5 years, all having different makeups. The most recent one was 40% calcium phosphate, 30% calcium oxalate monohydrate, 30% calcium oxalate dihydrate. I haven’t found a physician that will work on prevention, mostly because they want to get rid of them before we get into prevention treatment and we can’t get rid of them. So I’m continually researching for myself and I never seem to find solid recommendations. What should I avoid? What do I need more of (besides water, I crave flavor and am also hypoglycemic so I can’t do anything with artificial sweeteners)?
I’ll add I am magnesium, vitamin D, and B-12 deficient, borderline hypothyroidism. My urine almost always has a high PH and frequent bacterial infections. My sodium levels in my blood are good. I’m just tired of constantly being in pain.
Hi Elizabeth, Stones since 16, high urine pH, I would guess you have genetic hypercalciuria, but that is just a guess. You need comprehensive testing to figure out if this is the cause, or something else. Here is my usual suggestions for evaluation. Your hypoglycemia may be due to abnormal insulin response to sugar, and worsened by sugar intake – rebound hypoglycemia. That can raise urine calcium in bursts after each sugar load. I am quite certain your stone production can be much lowered, but do not have enough details to say more. Regards, Fred Coe
Am 30years old and the doctor says I have calcium oxalate in my utrin, he advise to keep drinking water very often to help me pass the stone what can I possibly do to pass it and any recommendation to prevent it
Hi Bello, treatment depends on cause, which is found by 24 hour and blood testing. Here is my favorite article on how to proceed. Regards, Fred Coe
Am 30years old and the doctor says I have calcium oxalate in my utrin, he advise to keep drinking water very often to help me pass the stone what can I possibly do to pass it and any recommendation to prevent it
Hi Bello, treatment depends on cause, which is found by 24 hour and blood testing. Here is my favorite article on how to proceed. Regards, Fred Coe
Calcium Oxalate stones are sharp and after breakup are like urinating sharp glass shards. Extremely ouchy.
Let’s call that 9 out of 10 sharpness.
What sharpness number would you assign
uric acid stones?
and
cysteine stones?
Hi Seth, Uric acid and cystine stones cause pain like other stones – I do not believe I can separate them by pain. Thus my emphasis on prevention. Fred
Carbonat ampatites cystine stone
Hi Muhammad, if it contains cystine, you probably have cystinuria – an uncommon, complex and treatable disease. Regards, Fred Coe
Carbonat ampatites cystine stone
Hi Muhammad, if it contains cystine, you probably have cystinuria – an uncommon, complex and treatable disease. Regards, Fred Coe
Hello Dr. Coe, I’m Beth a 64 yr. Old white female dx. with MS 23 yrs. Ago. Due to neurogenic bladder=urostomy 6 yrs. Ago. Most of my lesions are in spinal cord. 2 yrs. Ago had a stone lodged in left ureter unaware bc no pain. Annual urology check up & hydronephrosis left kidney=Or stone removed via kidney. June 2021 urologist stated 3 stones left kidney & 1 IN right kidney. Researched & read were MS pts. Like folks with spinal cord nerve damage =stones. I do not eat dairy or red meat. I drink dly 48 to 60 ozs Of h2o dly. They cannot due a bone density test=osteoporosis-calcium?
Hi Beth, I guess the obstruction damaged the left kidney and you have one in the right kidney. You must find out what is causing the stones and act to prevent more. This chapter gives a very good overview of what to do, beginning with what the stones were that were removed. I would study it and make a plan so more stones do not form. Regards, Fred Coe